You might also like
- NCM 117 Lecture - Prelim PDFDocument32 pagesNCM 117 Lecture - Prelim PDFKimberly Ann BoricanoNo ratings yet
- Characteristics of a mentally healthy personDocument8 pagesCharacteristics of a mentally healthy personNP YarebNo ratings yet
- Mental Health: Understanding Etiology for Effective ManagementDocument22 pagesMental Health: Understanding Etiology for Effective ManagementMashfique AhmedNo ratings yet
- Mental Health and Mental IllnessDocument39 pagesMental Health and Mental IllnessChristopher MohammedNo ratings yet
- Fathering Loneliest Gen HIMPSIDocument45 pagesFathering Loneliest Gen HIMPSIhcintiland sbyNo ratings yet
- Words Are Not Enough Slide HandoutDocument21 pagesWords Are Not Enough Slide HandoutedytagancNo ratings yet
- NCM 117 Lec Prelim WK 1 2Document96 pagesNCM 117 Lec Prelim WK 1 2lynmercadejas27No ratings yet
- Trends and Issues in Mental Health and Drug AbuseDocument38 pagesTrends and Issues in Mental Health and Drug Abusekristine joy saulerNo ratings yet
- Understanding Depression and SuicideDocument21 pagesUnderstanding Depression and SuicideNikky SilvestreNo ratings yet
- Mental Health Challenges in the PhilippinesDocument41 pagesMental Health Challenges in the PhilippinesKimberly Ann BoricanoNo ratings yet
- Community HealthDocument5 pagesCommunity HealthMiguel C. DolotNo ratings yet
- Abnormal Psychology 2 (SEU-Austin)Document34 pagesAbnormal Psychology 2 (SEU-Austin)Beatriz GilNo ratings yet
- Understanding Mental Health Care for People with Intellectual DisabilitiesDocument65 pagesUnderstanding Mental Health Care for People with Intellectual DisabilitiesFrancois CreweNo ratings yet
- SAS REVIEWERS | Mental Health FactorsDocument10 pagesSAS REVIEWERS | Mental Health FactorsMarion NavarroNo ratings yet
- Psychia NotesDocument6 pagesPsychia NotesMaria Theresa BuscasNo ratings yet
- OK - HP8003 NotesDocument71 pagesOK - HP8003 NotesjamesngNo ratings yet
- Mental Health Awareness and Suicide Prevention PDFDocument44 pagesMental Health Awareness and Suicide Prevention PDFRynbie Quilantang Galan LptNo ratings yet
- SP Final Re-WriteDocument8 pagesSP Final Re-Writeapi-613889182No ratings yet
- Of Mice and MenDocument12 pagesOf Mice and MenAkshitaa PandeyNo ratings yet
- 1 - Introduction To Psychiatric Nursing PDFDocument13 pages1 - Introduction To Psychiatric Nursing PDFDiana CalderonNo ratings yet
- Effects of Racism FinalDocument5 pagesEffects of Racism FinalthatusernameistakejustkiddinNo ratings yet
- Mental Health On Adolescence: The OneselfDocument1 pageMental Health On Adolescence: The OneselfEdison Acosta LimbagaNo ratings yet
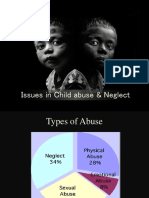
- Issues in Child Abuse & NeglectDocument28 pagesIssues in Child Abuse & NeglectAmrutha KrishnanNo ratings yet
- Effects of Child Abuse and Neglect On Children and Their Development-Alekhya, Nebiyu, Jessica, Zahra, ReneeDocument14 pagesEffects of Child Abuse and Neglect On Children and Their Development-Alekhya, Nebiyu, Jessica, Zahra, ReneeZahra RiazNo ratings yet
- New 1Document27 pagesNew 1Amrutha KrishnanNo ratings yet
- Mental HealthDocument55 pagesMental HealthEricLumogdaLegadaNo ratings yet
- Definitions of Mental Health, Mental Health Problems, and Mental IllnessDocument3 pagesDefinitions of Mental Health, Mental Health Problems, and Mental IllnessEinsen AngelesNo ratings yet
- Mentalhealth 160721120329Document49 pagesMentalhealth 160721120329Mangala bote Nair PSMNo ratings yet
- Mental Illnesses in Children and Youth: Learn AboutDocument4 pagesMental Illnesses in Children and Youth: Learn AboutStefan BasilNo ratings yet
- Mhu Community Mental Health Handbook English 1Document22 pagesMhu Community Mental Health Handbook English 1Justus AshabaNo ratings yet
- Interpersonal TheoryDocument21 pagesInterpersonal TheoryKaren AcuarioNo ratings yet
- 10 ChildPsychiatry PDFDocument45 pages10 ChildPsychiatry PDFCetVital100% (1)
- Mental Health Week (2018)Document23 pagesMental Health Week (2018)Katrina MillaNo ratings yet
- 117 NotesDocument17 pages117 NotesMARYISABEL �ERNINo ratings yet
- The Psychological and Social Consequences of HomelessnessDocument23 pagesThe Psychological and Social Consequences of HomelessnessnaleahNo ratings yet
- Child Abuse AND Battered Child SyndromeDocument90 pagesChild Abuse AND Battered Child SyndromeAmy Lalringhluani ChhakchhuakNo ratings yet
- Kesehatan Mental KomunitasDocument29 pagesKesehatan Mental KomunitasAyunita FajarNo ratings yet
- Clase 6 - Maltrato InfantilDocument7 pagesClase 6 - Maltrato InfantilFelipe AguileraNo ratings yet
- SSWD AutismDocument22 pagesSSWD Autismapi-663471551No ratings yet
- 1) Distorted Thinking Patterns 2) Problematic Emotional Responses 3) Over-Or Under-Regulated Impulse Control 4) Interpersonal DifficultiesDocument38 pages1) Distorted Thinking Patterns 2) Problematic Emotional Responses 3) Over-Or Under-Regulated Impulse Control 4) Interpersonal Difficultiesnico ValenzonaNo ratings yet
- Child AbuseDocument49 pagesChild Abuseviola gondweNo ratings yet
- Neurocognitve Developmet DisordersDocument53 pagesNeurocognitve Developmet DisordersMUZE TELANo ratings yet
- PsychosisDocument61 pagesPsychosisJohn CabilanNo ratings yet
- 1Document4 pages1Jhon LeonorNo ratings yet
- Child Psychiatry1Document21 pagesChild Psychiatry1mariam tarekNo ratings yet
- Chap 5 eDocument10 pagesChap 5 eNovendi RizkaNo ratings yet
- Intro Child PsychiatryDocument122 pagesIntro Child PsychiatryayunisallehNo ratings yet
- Adolescent For Ho 4Document38 pagesAdolescent For Ho 4Habib HajiNo ratings yet
- Attitudinal TransformationDocument23 pagesAttitudinal Transformationhussham100% (1)
- Mental HealthDocument16 pagesMental HealthMarivic SonidoNo ratings yet
- Research Log 1Document3 pagesResearch Log 1api-549018895No ratings yet
- Conduct Disorder: Dr. Jayanta Kurmi Junior Resident Dept of Psychiatry SMCHDocument50 pagesConduct Disorder: Dr. Jayanta Kurmi Junior Resident Dept of Psychiatry SMCHJayanta Kurmi100% (1)
- What Is SexualityDocument2 pagesWhat Is SexualityYasmen MendezNo ratings yet
- CHC Mental Health Facts 101Document16 pagesCHC Mental Health Facts 101meezNo ratings yet
- Adol. Psych. - Cognitive-Emotional Immaturity during AdolescenceDocument30 pagesAdol. Psych. - Cognitive-Emotional Immaturity during AdolescenceTaremwa PeterNo ratings yet
- Personality DisordersDocument95 pagesPersonality Disorderscatherine faith gallemitNo ratings yet
- Lack of Mental Health Awareness in India Terrible ConsequencesDocument3 pagesLack of Mental Health Awareness in India Terrible ConsequencesSomya BansalNo ratings yet
- Mental HealthDocument4 pagesMental HealthJihan Izzatun NisaNo ratings yet
- Yipee AbpsychDocument223 pagesYipee AbpsychYsabel VictoriaNo ratings yet
- Resume: Name: Ni Made SuastiniDocument3 pagesResume: Name: Ni Made Suastiniduz tha100% (1)
- The HOME - EU Project On Housing First As A Path To End Homelessness in EuropeDocument13 pagesThe HOME - EU Project On Housing First As A Path To End Homelessness in EuropeInês PereiraNo ratings yet
- DIASS Module 2 Lesson 2Document15 pagesDIASS Module 2 Lesson 2Liza G. Renomeron - MalateNo ratings yet
- Diass Topic 5 Social WorkDocument13 pagesDiass Topic 5 Social Workjstaana219No ratings yet
- BAC English Oral Exam TopicsDocument15 pagesBAC English Oral Exam TopicsOdette Müller-DoganNo ratings yet
- DOCUMENT VAESENDocument1 pageDOCUMENT VAESENJosé Thomaz Nonô BisnetoNo ratings yet
- Handling Stress & Emotions at WorkDocument6 pagesHandling Stress & Emotions at WorkLijoy LijuNo ratings yet
- Self Injury in Adolescents That May Disturb The Mental HealthDocument13 pagesSelf Injury in Adolescents That May Disturb The Mental HealthRiyn NamjungNo ratings yet
- Concepts and Principles of AgingDocument8 pagesConcepts and Principles of AgingTrixie GulokNo ratings yet
- Physical Fitness HandoutDocument4 pagesPhysical Fitness HandoutDianna Rose QuintoNo ratings yet
- Afternoon II Workshops 2015Document6 pagesAfternoon II Workshops 2015lauryn_biancoNo ratings yet
- Zhang Et Al., 2022Document49 pagesZhang Et Al., 2022VictoriaNo ratings yet
- Prophetic Dreams 2016 PDFDocument7 pagesProphetic Dreams 2016 PDFElena AndronacheNo ratings yet
- Domestic Violence Against Women in MalaysiaDocument15 pagesDomestic Violence Against Women in MalaysiaStephen NyakundiNo ratings yet
- Final CHN g1Document52 pagesFinal CHN g1Cariology YuNo ratings yet
- Chapter 7: Staffing: Didik, Elizabeth, ShintaDocument12 pagesChapter 7: Staffing: Didik, Elizabeth, ShintaElizabeth Alexandria LaurenNo ratings yet
- Performance and Development Review (PDR) Form: Part A: Objectives - What Is Expected of Me in My Role?Document7 pagesPerformance and Development Review (PDR) Form: Part A: Objectives - What Is Expected of Me in My Role?Arrow LazarusNo ratings yet
- 3F - RLE 1M 1st DraftDocument24 pages3F - RLE 1M 1st DraftDominic DegraciaNo ratings yet
- Nola Pender's Health Promotion ModelDocument4 pagesNola Pender's Health Promotion ModelJoy PelpinosasNo ratings yet
- L.P. of Transcultural NursingDocument14 pagesL.P. of Transcultural Nursingvikas takNo ratings yet
- Neuropsychological Test Uses: BrainDocument2 pagesNeuropsychological Test Uses: BrainElisa TapalesNo ratings yet
- BRM Part IiDocument349 pagesBRM Part Iimolalign tekalignNo ratings yet
- Ricaro FA2 EthicsDocument3 pagesRicaro FA2 EthicsMiguel RicaroNo ratings yet
- Anger Management-Lesson PlanDocument7 pagesAnger Management-Lesson Planapi-430630903100% (1)
- Cause and Effect..dll Lesson PlanDocument4 pagesCause and Effect..dll Lesson PlanJessaMyn HLNo ratings yet
- Infernal Might Common Lore - DTF (With Bookmarks) 3-29-2019Document14 pagesInfernal Might Common Lore - DTF (With Bookmarks) 3-29-2019Jordan DeWittNo ratings yet
- Meta-Programs - Neuro Linguistic Programing in Agile CoachingDocument9 pagesMeta-Programs - Neuro Linguistic Programing in Agile CoachingCorina ModorceaNo ratings yet
- The Nursing Theories of Faye Abdellah and Virginia HendersonDocument4 pagesThe Nursing Theories of Faye Abdellah and Virginia HendersonVictor VeraNo ratings yet
- Case Study Method In-Depth AnalysisDocument9 pagesCase Study Method In-Depth AnalysisFia ekaNo ratings yet
- Keep Your Resolution: Hypnotist Vance Romane's Online Seminar To Stop Smoking, Manage StressDocument4 pagesKeep Your Resolution: Hypnotist Vance Romane's Online Seminar To Stop Smoking, Manage StressPR.comNo ratings yet
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (38)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (140)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaFrom EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaRating: 4.5 out of 5 stars4.5/5 (56)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONFrom EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONRating: 4.5 out of 5 stars4.5/5 (24)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- Overcoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsFrom EverandOvercoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsRating: 4.5 out of 5 stars4.5/5 (48)
- When Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionFrom EverandWhen Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionRating: 4 out of 5 stars4/5 (11)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- Embrace Your Weird: Face Your Fears and Unleash CreativityFrom EverandEmbrace Your Weird: Face Your Fears and Unleash CreativityRating: 4.5 out of 5 stars4.5/5 (124)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisFrom EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (5)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (249)
- Summary: Psycho-Cybernetics: by Maxwell Maltz: Key Takeaways, Summary & AnalysisFrom EverandSummary: Psycho-Cybernetics: by Maxwell Maltz: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (2)
- Vagus Nerve: A Complete Self Help Guide to Stimulate and Activate Vagal Tone — A Self Healing Exercises to Reduce Chronic Illness, PTSD, Anxiety, Inflammation, Depression, Trauma, and AngerFrom EverandVagus Nerve: A Complete Self Help Guide to Stimulate and Activate Vagal Tone — A Self Healing Exercises to Reduce Chronic Illness, PTSD, Anxiety, Inflammation, Depression, Trauma, and AngerRating: 4.5 out of 5 stars4.5/5 (16)
- The Secrets of Vagus Nerve Stimulation: 18 Proven, Science-Backed Exercises and Methods to Activate Your Vagal Tone and Heal from Inflammation, Chronic Stress, Anxiety, Epilepsy, and Depression.From EverandThe Secrets of Vagus Nerve Stimulation: 18 Proven, Science-Backed Exercises and Methods to Activate Your Vagal Tone and Heal from Inflammation, Chronic Stress, Anxiety, Epilepsy, and Depression.Rating: 5 out of 5 stars5/5 (14)
- Triggers: How We Can Stop Reacting and Start HealingFrom EverandTriggers: How We Can Stop Reacting and Start HealingRating: 5 out of 5 stars5/5 (58)
- Anxious for Nothing: Finding Calm in a Chaotic WorldFrom EverandAnxious for Nothing: Finding Calm in a Chaotic WorldRating: 4.5 out of 5 stars4.5/5 (1244)
- The Anatomy of Loneliness: How to Find Your Way Back to ConnectionFrom EverandThe Anatomy of Loneliness: How to Find Your Way Back to ConnectionRating: 4.5 out of 5 stars4.5/5 (162)