You might also like
- Enrollment FormDocument3 pagesEnrollment FormgauravpassionNo ratings yet
- What Is State Pension Non-Contributory?Document20 pagesWhat Is State Pension Non-Contributory?noor bashaNo ratings yet
- AcupunctureDocument8 pagesAcupunctureNabendu SahaNo ratings yet
- Prauth FormDocument2 pagesPrauth FormAwesome CriticNo ratings yet
- AS CombineDocument2 pagesAS Combinelee100867No ratings yet
- Claim Form B Medical Attendant CertificateDocument1 pageClaim Form B Medical Attendant Certificatesuja01974No ratings yet
- Social Care Health Self-Declaration Form For Use During COVID-19 PandemicDocument8 pagesSocial Care Health Self-Declaration Form For Use During COVID-19 PandemicMary's CatzNo ratings yet
- Application Form For Private ApplicantsDocument1 pageApplication Form For Private Applicantskavinda jayamahaNo ratings yet
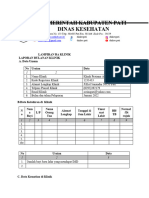
- Laporan Lampiran Ba Kesesuaian KlinikDocument5 pagesLaporan Lampiran Ba Kesesuaian KlinikYENI AYU OKTAVIANo ratings yet
- Working Family PaymentDocument12 pagesWorking Family PaymentGordonPhillipsNo ratings yet
- What Is The Free Travel Scheme?Document8 pagesWhat Is The Free Travel Scheme?alexandrazdziarskaNo ratings yet
- Medical Local FormDocument4 pagesMedical Local FormNeezam PauziNo ratings yet
- Citizenship c3 c4Document5 pagesCitizenship c3 c4yinjian0001No ratings yet
- Habitual Residence Condition: What Does Habitual Residence Mean? How Do I Qualify For Habitual Residence?Document24 pagesHabitual Residence Condition: What Does Habitual Residence Mean? How Do I Qualify For Habitual Residence?rolexNo ratings yet
- Starhealth AL I L ED Nsuran E O., LTD C C I 1 8 0 0 4 2 5 2 2 5 5 1 8 0 0 4 2 5 5 5 2 2Document2 pagesStarhealth AL I L ED Nsuran E O., LTD C C I 1 8 0 0 4 2 5 2 2 5 5 1 8 0 0 4 2 5 5 5 2 2Awesome CriticNo ratings yet
- 2324 SFE PFF2 Form - 1Document20 pages2324 SFE PFF2 Form - 1MarioNo ratings yet
- Permission To Change Banking Details: Contact UsDocument2 pagesPermission To Change Banking Details: Contact UsOngegund5No ratings yet
- Ontabilidad Financiera VDocument3 pagesOntabilidad Financiera VJorge Santiago Real MedinaNo ratings yet
- DH ApplicationDocument5 pagesDH Applicationharish sappaNo ratings yet
- Sfe FULLFILLEDDocument20 pagesSfe FULLFILLEDJosep SetóNo ratings yet
- MSI Health ServicesDocument16 pagesMSI Health ServicesHihiNo ratings yet
- Blank Editable Consent Form (1) - ScoutsDocument2 pagesBlank Editable Consent Form (1) - ScoutsGiovanni RossiNo ratings yet
- Discovery - Group - Risk and Funeral - Beneficiary - Nomination - Form - Member - Comms - V3Document4 pagesDiscovery - Group - Risk and Funeral - Beneficiary - Nomination - Form - Member - Comms - V3Monde CeleNo ratings yet
- IELTSDocument11 pagesIELTSombir sainiNo ratings yet
- NEW Domiciliary Claim Form PDFDocument1 pageNEW Domiciliary Claim Form PDFHimanshu ChoukseyNo ratings yet
- Domiciliary Treatment - Claim Form - Borl: Details of Primary InsuredDocument1 pageDomiciliary Treatment - Claim Form - Borl: Details of Primary InsuredHimanshu Chouksey100% (1)
- Mediprime: Claim FormDocument4 pagesMediprime: Claim FormMunna Bhai MbaNo ratings yet
- A 058285296Document2 pagesA 058285296Funn TimeNo ratings yet
- Vitality Wellness Network For DoctorsDocument3 pagesVitality Wellness Network For DoctorsjoatdhsNo ratings yet
- Kidney Disease Questionnaire For Proposed Insured/OwnerDocument1 pageKidney Disease Questionnaire For Proposed Insured/OwnerSincerely ReynNo ratings yet
- Kidney Disease Questionnaire PDFDocument1 pageKidney Disease Questionnaire PDFSincerely ReynNo ratings yet
- Mps Application FormDocument4 pagesMps Application Form健康生活園Healthy Life GardenNo ratings yet
- Kidney Disease Questionnaire PDFDocument1 pageKidney Disease Questionnaire PDFSincerely ReynNo ratings yet
- Application Form For International Students: 宗教信仰 ReligionDocument3 pagesApplication Form For International Students: 宗教信仰 ReligionTRUST ZHOUNo ratings yet
- .. - State Common Entrance Test Cell, Government of Maharashtra - ..Document2 pages.. - State Common Entrance Test Cell, Government of Maharashtra - ..Sakshi suransNo ratings yet
- Direct Deposit Form: B e N o I T J A M e S KDocument1 pageDirect Deposit Form: B e N o I T J A M e S KKevin BenoitNo ratings yet
- Phillips Hmo Enrollee Subscription FormDocument2 pagesPhillips Hmo Enrollee Subscription FormJack EzehNo ratings yet
- Phillips Hmo Enrollee Subscription FormDocument2 pagesPhillips Hmo Enrollee Subscription FormOnyekachi JackNo ratings yet
- British Embassy Job Application Form: Please Type or PrintDocument5 pagesBritish Embassy Job Application Form: Please Type or PrintAndreea Ioana BerilaNo ratings yet
- ChildDocument16 pagesChildmorenamoldovan3No ratings yet
- AFL Loan Application V03052021 FilledDocument4 pagesAFL Loan Application V03052021 FilledSAnjaiNo ratings yet
- Declaration of Good Health Cum Membership Form: Life InsuranceDocument2 pagesDeclaration of Good Health Cum Membership Form: Life InsuranceAkshay JagdaleNo ratings yet
- State Pension (Contributory) : Application Form ForDocument20 pagesState Pension (Contributory) : Application Form ForYvonne ChiltonNo ratings yet
- State of Illinois COVID-19 Update Nov. 6Document9 pagesState of Illinois COVID-19 Update Nov. 6CrainsChicagoBusinessNo ratings yet
- 2324 SFE PFF2 FormDocument20 pages2324 SFE PFF2 FormMarioNo ratings yet
- Instructions To DefendantsDocument1 pageInstructions To DefendantsobsidNo ratings yet
- HDFC ERGO General Insurance Company Limited Claim FormDocument8 pagesHDFC ERGO General Insurance Company Limited Claim FormYash ChaudharyNo ratings yet
- WC Application 2023 - 230620Document3 pagesWC Application 2023 - 230620Mansi GandhiNo ratings yet
- New Employee Form - SriDocument2 pagesNew Employee Form - SriChintya KartiniNo ratings yet
- Yerleşim Yeri - İNGİLİZCEDocument5 pagesYerleşim Yeri - İNGİLİZCEErdinç KuşçuNo ratings yet
- Sdeexamapp PDFDocument2 pagesSdeexamapp PDFpriya_psalmsNo ratings yet
- MBBS FormDocument4 pagesMBBS FormUtkarsh SinghalNo ratings yet
- Aditya Birla - Form ADocument4 pagesAditya Birla - Form APrashant KarekarNo ratings yet
- 1.individual AML-CFT Client Form ADocument1 page1.individual AML-CFT Client Form AOmar AhsanNo ratings yet
- Newborn Application FormDocument2 pagesNewborn Application FormMicaela KrielNo ratings yet
- Afyaimara Medical Cover: Application FormDocument7 pagesAfyaimara Medical Cover: Application FormNicholas WambeteNo ratings yet
- Claimant Statement Form (Death Claims) : Customer Helpline No: 1860 266 7766Document3 pagesClaimant Statement Form (Death Claims) : Customer Helpline No: 1860 266 7766Tarun RustagiNo ratings yet
- IRAs, 401(k)s & Other Retirement Plans: Strategies for Taking Your Money OutFrom EverandIRAs, 401(k)s & Other Retirement Plans: Strategies for Taking Your Money OutRating: 4 out of 5 stars4/5 (18)
- Formal Description Techniques, IV: Proceedings of the IFIP TC6/WG6.1 Fourth International Conference on Formal Description Techniques for Distributed Systems and Communications Protocols, FORTE '91, Sydney, Australia, 19-22 November 1991From EverandFormal Description Techniques, IV: Proceedings of the IFIP TC6/WG6.1 Fourth International Conference on Formal Description Techniques for Distributed Systems and Communications Protocols, FORTE '91, Sydney, Australia, 19-22 November 1991K.R. ParkerNo ratings yet
- Content and Contextual Analysis of Primary SourcesDocument9 pagesContent and Contextual Analysis of Primary SourcesCielo Nicole De GuzmanNo ratings yet
- Hallticket OMATAAR029 19-04-2022Document2 pagesHallticket OMATAAR029 19-04-2022Muhammed SwalihNo ratings yet
- Basic Microeconomics Course OutlineDocument2 pagesBasic Microeconomics Course OutlineLorraine JNo ratings yet
- AT03 03 The Accountancy Profession PresentationDocument66 pagesAT03 03 The Accountancy Profession Presentationgutlaysophia06No ratings yet
- Dimas - Reciprocal Teaching Approach Topic MatrixDocument3 pagesDimas - Reciprocal Teaching Approach Topic MatrixMaricarDimasNo ratings yet
- Ib Business and Management CourseworkDocument7 pagesIb Business and Management Courseworkafazbsaxi100% (2)
- A Practical Guide in Writing Your Action Research: July 2012Document25 pagesA Practical Guide in Writing Your Action Research: July 2012Trang NguyenNo ratings yet
- Facilitate Learning Sessions: (Written Exam)Document8 pagesFacilitate Learning Sessions: (Written Exam)Precious Andoy-Megabon0% (1)
- Rrllb81 Tut 301 Tutorial WorkDocument48 pagesRrllb81 Tut 301 Tutorial Worktshepangtshepi001No ratings yet
- SVMCM (V3.0) : Renewal Application DetailsDocument2 pagesSVMCM (V3.0) : Renewal Application Detailspappu dasNo ratings yet
- Wjec Media Studies A Level Coursework Grade BoundariesDocument4 pagesWjec Media Studies A Level Coursework Grade Boundariespqdgddifg100% (1)
- GVR - ECCE Michigan Exam Practice - Test 1Document11 pagesGVR - ECCE Michigan Exam Practice - Test 1Miriam88% (8)
- STA630 Mid Term Past Papers Mega FileDocument19 pagesSTA630 Mid Term Past Papers Mega Fileadina riazNo ratings yet
- Clarification For Language AcqDocument3 pagesClarification For Language AcqROXANA QUISPE CUADROSNo ratings yet
- CEE Seminar Report TemplateDocument3 pagesCEE Seminar Report TemplateBitch CarrieNo ratings yet
- COC 1 and COC 2 ScriptDocument8 pagesCOC 1 and COC 2 ScriptIbarra Nicole VillegasNo ratings yet
- Tle8 SLM Q1M4Document31 pagesTle8 SLM Q1M4christian paulNo ratings yet
- Pastor PrinceDocument13 pagesPastor PrinceWidimongar W. JarqueNo ratings yet
- Manual Pdu 2017Document37 pagesManual Pdu 2017Chris SánchezNo ratings yet
- Financial Statement Analysis: Standard Course OutlineDocument6 pagesFinancial Statement Analysis: Standard Course OutlineMahmoud ZizoNo ratings yet
- NYU Tandon Financial EngineeringDocument1 pageNYU Tandon Financial EngineeringmmhjxxcearelkuoahqNo ratings yet
- POLYCET - 2020: Government of Andhra Pradesh Department of Technical EducationDocument64 pagesPOLYCET - 2020: Government of Andhra Pradesh Department of Technical EducationSai PavanNo ratings yet
- 241 - 430 - 4 - 3 - Mathematics (Basic)Document8 pages241 - 430 - 4 - 3 - Mathematics (Basic)Shikhar BijaniNo ratings yet
- What Next After 10th, Inter, DegreeDocument10 pagesWhat Next After 10th, Inter, DegreeBlue JaguarNo ratings yet
- Reviewer in MATHEMATICSDocument84 pagesReviewer in MATHEMATICSMarlyn TenorioNo ratings yet
- 2019 MYANMAR Student Mobility Facts and FiguresDocument2 pages2019 MYANMAR Student Mobility Facts and FiguresHikari ChanNo ratings yet
- ICICI CareersDocument2 pagesICICI CareersYuth Cricket Club ParariNo ratings yet
- Learning Delivery Modalities Course 2 (LDM2) For TeachersDocument94 pagesLearning Delivery Modalities Course 2 (LDM2) For TeachersJOSEFINA MAGADIANo ratings yet
- ED 209 - Assessment in Learning 2 Part I. Multiple ChoiceDocument4 pagesED 209 - Assessment in Learning 2 Part I. Multiple ChoiceLouise Ann Bersamin82% (22)
- Academic Background and Course Involvement As Predictors of Exam PerformanceDocument5 pagesAcademic Background and Course Involvement As Predictors of Exam PerformanceNguyễn Trần Bá ToànNo ratings yet