You might also like
- Febrile SeizureDocument6 pagesFebrile SeizurepipimseptianaNo ratings yet
- Presentasi Jurnal Kejang DemamDocument21 pagesPresentasi Jurnal Kejang DemamSeptiana WahyuNo ratings yet
- Case Based Pediatrics For Medical Students and ResidentsDocument6 pagesCase Based Pediatrics For Medical Students and Residentssantosaerwin6591100% (1)
- tmpD6CD TMPDocument8 pagestmpD6CD TMPFrontiersNo ratings yet
- Febrile Seizures: Jithangi WanigasingheDocument5 pagesFebrile Seizures: Jithangi WanigasingheNadya ErlianieNo ratings yet
- Management of Febrile SeizuresDocument9 pagesManagement of Febrile SeizuresLi FaungNo ratings yet
- DMCN 14015Document10 pagesDMCN 14015Anida HasnaNo ratings yet
- 1 s2.0 S1875957210600198 MainDocument9 pages1 s2.0 S1875957210600198 MainTaddesse taddesse Taddesse taddesseNo ratings yet
- Clinical and Etiological Profile of Acute Febrile Encephalopathy in Eastern NepalDocument3 pagesClinical and Etiological Profile of Acute Febrile Encephalopathy in Eastern NepalNeha OberoiNo ratings yet
- Jurnal LisahaerDocument4 pagesJurnal LisahaerLissa AlhabsyiNo ratings yet
- Simple Versus Complex Febrile SeizureDocument18 pagesSimple Versus Complex Febrile SeizurePiet SeLoesindNo ratings yet
- Terapi S.EDocument5 pagesTerapi S.EnafamaulidinaNo ratings yet
- Apnea Emotiva Grave PDFDocument5 pagesApnea Emotiva Grave PDFfranckitaNo ratings yet
- Develop Med Child Neuro - 2018 - Sartori - First Ever Convulsive Seizures in Children Presenting To The EmergencyDocument10 pagesDevelop Med Child Neuro - 2018 - Sartori - First Ever Convulsive Seizures in Children Presenting To The EmergencyMarysol UlloaNo ratings yet
- Day 2a. Febrile Seizure Kuliah MHS 2012pdfDocument39 pagesDay 2a. Febrile Seizure Kuliah MHS 2012pdfNym Angga SantosaNo ratings yet
- Epilepsia - 2011 - Cendes - Vaccinations and Febrile SeizuresDocument3 pagesEpilepsia - 2011 - Cendes - Vaccinations and Febrile SeizurespuhumightNo ratings yet
- Ophthalmological Findings in Children With EncephalitisDocument8 pagesOphthalmological Findings in Children With EncephalitisSabila TasyakurNo ratings yet
- Technical Report: Treatment of The Child With Simple Febrile SeizuresDocument59 pagesTechnical Report: Treatment of The Child With Simple Febrile SeizuresCiara May SeringNo ratings yet
- Kejang Hiperglikemi PDFDocument10 pagesKejang Hiperglikemi PDFNishfullaili Nurun NisaNo ratings yet
- Santoso 2020Document10 pagesSantoso 2020Aldo VictoriaNo ratings yet
- Nfluenza-Associated Encephalitis Encephalopathy Identified by The Australian Childhood Encephalitis Study 2013-2015.Document6 pagesNfluenza-Associated Encephalitis Encephalopathy Identified by The Australian Childhood Encephalitis Study 2013-2015.zhoujNo ratings yet
- Epilepsia - 2005 - Knudsen - Febrile Seizures Treatment and PrognosisDocument8 pagesEpilepsia - 2005 - Knudsen - Febrile Seizures Treatment and PrognosisJanina MaligayaNo ratings yet
- BCMJ 53 Vol6 Febrile SeizuresDocument6 pagesBCMJ 53 Vol6 Febrile SeizuresdyyyaNo ratings yet
- Kejang 10Document6 pagesKejang 10nadya camelia pradasariNo ratings yet
- Epilepsia - 2023 - Gould - Are Brief Febrile Seizures Benign A Systematic Review and Narrative SynthesisDocument11 pagesEpilepsia - 2023 - Gould - Are Brief Febrile Seizures Benign A Systematic Review and Narrative Synthesis1400055hNo ratings yet
- Febrile Seizures: Definition and ClassificationDocument3 pagesFebrile Seizures: Definition and ClassificationArmin AbasNo ratings yet
- Evaluasi Anak Dengan Kejang DemamDocument4 pagesEvaluasi Anak Dengan Kejang DemamdavidNo ratings yet
- Neonatal Seizure Mechanisms and Management UpdateDocument20 pagesNeonatal Seizure Mechanisms and Management UpdateJuan Martín Velasco CárdenasNo ratings yet
- 586.1 Febrile Seizures Mohamad A. MikatiDocument5 pages586.1 Febrile Seizures Mohamad A. MikatiDewida 'dewet' MaulidatuNo ratings yet
- Drugs in Context Volume 7 Issue 2018 (Doi 10.7573 - Dic.212536) Leung, Alexander KC Hon, Kam Lun Leung, Theresa NH - Febrile Seizures - An OverviewDocument12 pagesDrugs in Context Volume 7 Issue 2018 (Doi 10.7573 - Dic.212536) Leung, Alexander KC Hon, Kam Lun Leung, Theresa NH - Febrile Seizures - An OverviewAlwin Ardiansyah PulunganNo ratings yet
- Ejhs2503 0251Document6 pagesEjhs2503 0251Kiti AstutiNo ratings yet
- Atypical SspeDocument2 pagesAtypical Sspenisa_neyshaaljufriNo ratings yet
- 944 ArticleDocument8 pages944 ArticleAbang BoyyNo ratings yet
- Incidence and Risk Factors For Seizures in Central Nervous System Infections in ChildhoodDocument6 pagesIncidence and Risk Factors For Seizures in Central Nervous System Infections in ChildhoodLiani Toniaço BellesNo ratings yet
- Case Vignette. EpilepsyDocument8 pagesCase Vignette. EpilepsyAizel ManiagoNo ratings yet
- Neonatal Hipoxic IsquemicDocument21 pagesNeonatal Hipoxic IsquemicMariela Nadir Guerreros De VelasquezNo ratings yet
- The burden of pediatric status epilepticusDocument27 pagesThe burden of pediatric status epilepticusErick DjuandaNo ratings yet
- An Epidemiologic Study of 389 Children With EpilepDocument6 pagesAn Epidemiologic Study of 389 Children With Epilepbilal hadiNo ratings yet
- Riyan Agus FaisalDocument7 pagesRiyan Agus FaisalRiyan AgusNo ratings yet
- Link Between Seizures and Type 1 Diabetes ExploredDocument10 pagesLink Between Seizures and Type 1 Diabetes ExploredAbigail PheiliaNo ratings yet
- A Cohort Study To Assess The New WHO Japanese Encephalitis Surveillance StandardsDocument9 pagesA Cohort Study To Assess The New WHO Japanese Encephalitis Surveillance StandardsarmankoassracunNo ratings yet
- Epilepsy - Definition, Classification, Pathophysiology, and EpidemiologyDocument7 pagesEpilepsy - Definition, Classification, Pathophysiology, and EpidemiologyMartín FleiNo ratings yet
- Guideline Summary NGC-9469: RecommendationsDocument6 pagesGuideline Summary NGC-9469: RecommendationsIbrahim MachmudNo ratings yet
- Increased Number of Febrile Seizures in Very Preterm ChildrenDocument8 pagesIncreased Number of Febrile Seizures in Very Preterm ChildrenFarin MauliaNo ratings yet
- Epidemiology of Pediatric Acute Encephalitis/Encephalopathy in JapanDocument7 pagesEpidemiology of Pediatric Acute Encephalitis/Encephalopathy in Japaneko andryNo ratings yet
- Laporan Kasus Tonsilofaringitis AkutDocument8 pagesLaporan Kasus Tonsilofaringitis AkutAvhindAvhindNo ratings yet
- Epilepsy in Children with Cerebral PalsyDocument6 pagesEpilepsy in Children with Cerebral PalsyTiara Renita LestariNo ratings yet
- 472 1466 1 PB - 2Document6 pages472 1466 1 PB - 2Nazlia LarashitaNo ratings yet
- Febrile SeizureDocument16 pagesFebrile SeizureRashed Shatnawi100% (1)
- Relationships Between Serum Electrolytes and Febrile SeizureDocument4 pagesRelationships Between Serum Electrolytes and Febrile SeizureLedira Dara IsmiNo ratings yet
- R56 - Febrile SeizuresDocument28 pagesR56 - Febrile SeizuresradverNo ratings yet
- Pathogenesis of Opsoclonus MyoclonusDocument2 pagesPathogenesis of Opsoclonus MyoclonusIRENA GENINo ratings yet
- Sodium Channelopathy and Post-Pertussis SeizuresDocument2 pagesSodium Channelopathy and Post-Pertussis Seizuresworsham87No ratings yet
- Faktor Resiko Kejang PDFDocument10 pagesFaktor Resiko Kejang PDFHamtaroHedwigNo ratings yet
- Review Article: Etiology and Risk Factors of Febrile Seizure - An UpdateDocument10 pagesReview Article: Etiology and Risk Factors of Febrile Seizure - An UpdateResty Rahmiliah RahimNo ratings yet
- Ramaraj, Rajdurai Group 6 Md3 B2 PediaDocument19 pagesRamaraj, Rajdurai Group 6 Md3 B2 PediaRaj DuraiNo ratings yet
- Current Concepts On Epilepsy Management in Tuberous SclerosisDocument10 pagesCurrent Concepts On Epilepsy Management in Tuberous Sclerosiselmon patadunganNo ratings yet
- Recognition and Management of Febrile Convulsion in ChildrenDocument8 pagesRecognition and Management of Febrile Convulsion in ChildrenPutu WirasatyaNo ratings yet
- Journal Of: Clinical, Epidemiological and Laboratory Characteristics of Patients With Febrile ConvulsionDocument4 pagesJournal Of: Clinical, Epidemiological and Laboratory Characteristics of Patients With Febrile ConvulsioncuteNo ratings yet
- Distribution of Cooling To Avionics PDFDocument76 pagesDistribution of Cooling To Avionics PDFpuhumightNo ratings yet
- Titanium and Its Alloys: Metallurgy, Heat Treatment and Alloy CharacteristicsDocument13 pagesTitanium and Its Alloys: Metallurgy, Heat Treatment and Alloy CharacteristicsBruna GomesNo ratings yet
- MJIRI v19n4p319 enDocument4 pagesMJIRI v19n4p319 enpuhumightNo ratings yet
- Preterm Human Milk Composition A Systematic Literature ReviewDocument13 pagesPreterm Human Milk Composition A Systematic Literature ReviewpuhumightNo ratings yet
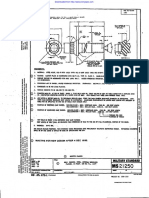
- MILITARY BOLT SPECIFICATIONDocument3 pagesMILITARY BOLT SPECIFICATIONRubén Darío Becerra GalindoNo ratings yet
- Foolishness Without Consequence? From Physical To Virtual Modeling in The History of Military Aircraft Development at SaabDocument19 pagesFoolishness Without Consequence? From Physical To Virtual Modeling in The History of Military Aircraft Development at SaabpuhumightNo ratings yet
- Decision Support System For Fault Isolation of JAS 39 Gripen PDFDocument71 pagesDecision Support System For Fault Isolation of JAS 39 Gripen PDFpuhumightNo ratings yet
- Diagnosis of The Air Distribution System of The JAS39 Gripen Environmental Control SystemDocument59 pagesDiagnosis of The Air Distribution System of The JAS39 Gripen Environmental Control SystempuhumightNo ratings yet
- Epilepsia - 2011 - Cendes - Vaccinations and Febrile SeizuresDocument3 pagesEpilepsia - 2011 - Cendes - Vaccinations and Febrile SeizurespuhumightNo ratings yet
- Development of Integrated Functional Monitoring and Warnings System For Saab 39 GripenDocument7 pagesDevelopment of Integrated Functional Monitoring and Warnings System For Saab 39 GripenpuhumightNo ratings yet
- 211799Document12 pages211799puhumightNo ratings yet
- Diagnosis On A Principle PDFDocument69 pagesDiagnosis On A Principle PDFpuhumightNo ratings yet
- Moog AG M-346 Brochure Mar15Document4 pagesMoog AG M-346 Brochure Mar15puhumightNo ratings yet
- IAI - LAVI Fighter Evolution: Ovadia Harari Memorial LectureDocument1 pageIAI - LAVI Fighter Evolution: Ovadia Harari Memorial LecturepuhumightNo ratings yet
- M-346 Advanced Trainer's Early Test Flights Achieve MilestonesDocument12 pagesM-346 Advanced Trainer's Early Test Flights Achieve MilestonespuhumightNo ratings yet
- New Configurations For The Windshield and The Canopy For A Two-Seater Trainer Military AircraftDocument8 pagesNew Configurations For The Windshield and The Canopy For A Two-Seater Trainer Military AircraftpuhumightNo ratings yet
- Aeroelastic Test and ValidationDocument21 pagesAeroelastic Test and ValidationpuhumightNo ratings yet
- M-346 Flight Test ProgrammeDocument10 pagesM-346 Flight Test ProgrammecoralonsoNo ratings yet
- Concept Definition: A Historical Perspective: (Based On A-10 Systems Engineering Case Study)Document22 pagesConcept Definition: A Historical Perspective: (Based On A-10 Systems Engineering Case Study)puhumightNo ratings yet
- T-6A Texan II Systems Engineering Case StudyDocument88 pagesT-6A Texan II Systems Engineering Case StudypuhumightNo ratings yet
- Aermacchi M-346FA The Fighter AttackDocument12 pagesAermacchi M-346FA The Fighter AttackpuhumightNo ratings yet
- Aircraft Active Flutter Suppression: State of The Art and Technology Maturation NeedsDocument41 pagesAircraft Active Flutter Suppression: State of The Art and Technology Maturation NeedspuhumightNo ratings yet
- Eads (Dasa) At-2000 MakoDocument8 pagesEads (Dasa) At-2000 MakopuhumightNo ratings yet
- Active content manual physics chapter measurementsDocument57 pagesActive content manual physics chapter measurementspuhumightNo ratings yet
- Active content manual physics chapter measurementsDocument57 pagesActive content manual physics chapter measurementspuhumightNo ratings yet
- F-22A Lightweight Gun System Comparison: NDIA Gun and Missile Systems Conference & ExhibitionDocument17 pagesF-22A Lightweight Gun System Comparison: NDIA Gun and Missile Systems Conference & ExhibitionpuhumightNo ratings yet
- Air Force Institute of Technology: Improving The Upt Student Follow-On Assignment Selection ProcessDocument91 pagesAir Force Institute of Technology: Improving The Upt Student Follow-On Assignment Selection ProcesspuhumightNo ratings yet
- ftft-OIO-ifc?: An Investigation of F/A-l 8 AMAD Gearbox Driveshaft VibrationDocument101 pagesftft-OIO-ifc?: An Investigation of F/A-l 8 AMAD Gearbox Driveshaft VibrationpuhumightNo ratings yet
- Aerodynamic Model Tests of Exhaust Augmentors for F/A-18 EngineDocument29 pagesAerodynamic Model Tests of Exhaust Augmentors for F/A-18 EnginepuhumightNo ratings yet
- Quiz Sistemas de AeronavesDocument23 pagesQuiz Sistemas de AeronavesAllain CelyNo ratings yet
- Race Solutiuon AllenDocument22 pagesRace Solutiuon AllenGjgcdNo ratings yet
- Our Lady of La Porteria Academy Senior High School Department Module in Trends, Networks, and Critical Thinking in The 21 Century Culture 12Document7 pagesOur Lady of La Porteria Academy Senior High School Department Module in Trends, Networks, and Critical Thinking in The 21 Century Culture 12Gab ReyesNo ratings yet
- Neuro Motor Readiness Pl2011Document94 pagesNeuro Motor Readiness Pl2011mohitnet1327100% (3)
- Fundamentals of Cognitive Psychology 2nd Edition Kellogg Test BankDocument11 pagesFundamentals of Cognitive Psychology 2nd Edition Kellogg Test BankElizabethSteelenjzpk100% (13)
- Treatment and Prognosis of Febrile Seizures - UpToDateDocument14 pagesTreatment and Prognosis of Febrile Seizures - UpToDateDinointernosNo ratings yet
- Information Processing Model: Sensory Memory: Information Enters The Human Information Processing System Via TheDocument17 pagesInformation Processing Model: Sensory Memory: Information Enters The Human Information Processing System Via TheMuskan100% (1)
- Theories of Memories and ForgettingDocument38 pagesTheories of Memories and ForgettingjayhandarwinNo ratings yet
- Code Stroke & Hyperacute Stroke TreatmentDocument35 pagesCode Stroke & Hyperacute Stroke TreatmentSitti Fatwan NisakNo ratings yet
- Development of Rhombencephalon and MesencephalonDocument27 pagesDevelopment of Rhombencephalon and MesencephalonRafique AhmedNo ratings yet
- Trip Report For Technical Writing PDFDocument1 pageTrip Report For Technical Writing PDFapi-512290651No ratings yet
- Biopsychology 9th Edition Pinel Test BankDocument25 pagesBiopsychology 9th Edition Pinel Test BankCameronAllenmtwei100% (64)
- Intelligent Counselor:An Intelligent Advisory SystemDocument6 pagesIntelligent Counselor:An Intelligent Advisory SystemIJSTENo ratings yet
- Febrile Seizure (Kejang Demam)Document25 pagesFebrile Seizure (Kejang Demam)KertiasihwayanNo ratings yet
- Chart To Analyze The Articles Webquest 2: AuthorDocument4 pagesChart To Analyze The Articles Webquest 2: Authorkatherin TorresNo ratings yet
- Rehabilitation AmbulationDocument14 pagesRehabilitation AmbulationDeborah SalinasNo ratings yet
- Encephalitis and Brain Abscess Continuum 2021Document32 pagesEncephalitis and Brain Abscess Continuum 2021geraldine paternina aguas100% (1)
- Exam 1 Answer KeyDocument8 pagesExam 1 Answer KeySharon KimNo ratings yet
- Changes From Icd 10 To 11Document9 pagesChanges From Icd 10 To 11Daniel John ArboledaNo ratings yet
- Human Ear Anatomy and PhysiologyDocument29 pagesHuman Ear Anatomy and PhysiologyAnkit SubediNo ratings yet
- Melanocytes - MelaninDocument27 pagesMelanocytes - MelaninJanelleNo ratings yet
- Emotion Perception 2Document14 pagesEmotion Perception 2Juan Camilo Sánchez AriasNo ratings yet
- Taste Buds & Taste ReceptorsDocument6 pagesTaste Buds & Taste ReceptorsMissz WazeeNo ratings yet
- Electrical Neuroimaging Koenig Thomas HandoutDocument12 pagesElectrical Neuroimaging Koenig Thomas HandoutDyah AprilNo ratings yet
- Nerve Physiology LectureDocument9 pagesNerve Physiology LectureMavic Villanueva100% (1)
- Asked: Frequently Questions About Neuromuscular DentistryDocument6 pagesAsked: Frequently Questions About Neuromuscular DentistryAhmed HamzaNo ratings yet
- On The Similarity of Odor and Language Perception: Tyler S. LorigDocument8 pagesOn The Similarity of Odor and Language Perception: Tyler S. LorigMTPNo ratings yet
- Lab Manual Sensory CompleteDocument18 pagesLab Manual Sensory Completeshanafisah100% (2)
- Foundations of Machine Learning: Module 6: Neural NetworkDocument22 pagesFoundations of Machine Learning: Module 6: Neural NetworkNishant TiwariNo ratings yet
- Science 8 PDFDocument172 pagesScience 8 PDFaftab khanNo ratings yet
- Positional Cervical Cord Compression Fibromyalgia PaperDocument7 pagesPositional Cervical Cord Compression Fibromyalgia PaperValiant LordNo ratings yet