You might also like
- 2014 Darrel Rees - How To Be An Illustrator PDFDocument168 pages2014 Darrel Rees - How To Be An Illustrator PDFdadcilifeNo ratings yet
- Case Study: International HRMDocument10 pagesCase Study: International HRMCornelius Kings 'Con'No ratings yet
- 00130478-202105000-00006 Serial Neurologic Assessment in Pediatrics (SNAP) : A New Tool For Bedside Neurologic Assessment of Critically Ill ChildrenDocument13 pages00130478-202105000-00006 Serial Neurologic Assessment in Pediatrics (SNAP) : A New Tool For Bedside Neurologic Assessment of Critically Ill ChildrenYo MeNo ratings yet
- Mythic Atropal - CR 40 Undead Quasi-DeityDocument1 pageMythic Atropal - CR 40 Undead Quasi-DeityDana HelmanNo ratings yet
- Organizational DevelopmentDocument12 pagesOrganizational DevelopmentShara Tumambing MA PsyNo ratings yet
- Noetzel and R.D. Sheth M. Shevell, S. Ashwal, D. Donley, J. Flint, M. Gingold, D. Hirtz, A. Majnemer, MDocument16 pagesNoetzel and R.D. Sheth M. Shevell, S. Ashwal, D. Donley, J. Flint, M. Gingold, D. Hirtz, A. Majnemer, MjoeunisaNo ratings yet
- A Pediatric FOUR Score Coma Scale: Interrater Reliability and Predictive ValidityDocument9 pagesA Pediatric FOUR Score Coma Scale: Interrater Reliability and Predictive ValidityrachmadyNo ratings yet
- 1377 FullDocument23 pages1377 FullPutri Wahyuni AllfazmyNo ratings yet
- She Vell 2003Document15 pagesShe Vell 2003Ivan VeriswanNo ratings yet
- Evaluation of The Child With Global Developmental DelayDocument14 pagesEvaluation of The Child With Global Developmental DelaylauramwoodyardNo ratings yet
- Schoenberg Et Al 2008 WISC IV Premorbid IntelligenceDocument8 pagesSchoenberg Et Al 2008 WISC IV Premorbid IntelligenceJoana Ponces de CarvalhoNo ratings yet
- Robinson 2014Document20 pagesRobinson 2014Laura PGNo ratings yet
- Neuropsychological Assessment in Children: Jornal de PediatriaDocument6 pagesNeuropsychological Assessment in Children: Jornal de PediatriaBenja MoranNo ratings yet
- Nih Mri StudyDocument18 pagesNih Mri StudyJudit ZCNo ratings yet
- The Design Organization Test: Further Demonstration of Reliability and Validity As A Brief Measure of Visuospatial AbilityDocument14 pagesThe Design Organization Test: Further Demonstration of Reliability and Validity As A Brief Measure of Visuospatial AbilitySamorNo ratings yet
- Methods of Neuropsychological Assessment EsDocument32 pagesMethods of Neuropsychological Assessment EsHermod26AnimeNo ratings yet
- Annett - Et - Al-2015-Pediatric - Blood - & - Cancer 2Document54 pagesAnnett - Et - Al-2015-Pediatric - Blood - & - Cancer 2KarolinaMaślakNo ratings yet
- Early, Accurate Diagnosis and Early Intervention in Cerebral PalsyDocument11 pagesEarly, Accurate Diagnosis and Early Intervention in Cerebral PalsyRoberto López MataNo ratings yet
- Neuropsychology Reports For Childhood Brain Tumor Survivors: Implementation of Recommendations at Home and SchoolDocument8 pagesNeuropsychology Reports For Childhood Brain Tumor Survivors: Implementation of Recommendations at Home and SchoolKamila PorębskaNo ratings yet
- Advances in pediatric clinical methodologyDocument9 pagesAdvances in pediatric clinical methodologyPopy LunaNo ratings yet
- Early, Accurate Diagnosis of Cerebral PalsyDocument11 pagesEarly, Accurate Diagnosis of Cerebral PalsyAndrea PederziniNo ratings yet
- Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy Advances in Diagnosis and TreatmentDocument11 pagesEarly, Accurate Diagnosis and Early Intervention in Cerebral Palsy Advances in Diagnosis and TreatmentMiguel Angel Rodriguez MartinezNo ratings yet
- Improving The Identification of Neonatal Web VideoDocument3 pagesImproving The Identification of Neonatal Web VideoBelén AracelyNo ratings yet
- UC San Francisco Previously Published Works: TitleDocument12 pagesUC San Francisco Previously Published Works: TitleMajito BNo ratings yet
- Jamapediatrics Novak 2017 RV 170003Document11 pagesJamapediatrics Novak 2017 RV 170003Evelyn HerreraNo ratings yet
- RetrieveDocument26 pagesRetrievemarta_gasparNo ratings yet
- Validation of The NIH Toolbox Cognitive Battery in Intellectual DisabilityDocument13 pagesValidation of The NIH Toolbox Cognitive Battery in Intellectual DisabilityRaul Morales VillegasNo ratings yet
- 1999 Mirsky Model Attention ADHDDocument9 pages1999 Mirsky Model Attention ADHDEduardo CastilloNo ratings yet
- Topics in Magnetic Resonance Imaging - Neuroimaging of The Child With Developmental DelayDocument18 pagesTopics in Magnetic Resonance Imaging - Neuroimaging of The Child With Developmental DelayJemima ChanNo ratings yet
- UC San Francisco Previously Published WorksDocument10 pagesUC San Francisco Previously Published WorksTessa CruzNo ratings yet
- Neuroimagenes en Preterminos y Rendimiento EscolarDocument15 pagesNeuroimagenes en Preterminos y Rendimiento EscolarAlejandroVeraVargasNo ratings yet
- Hammersmith NeonatalDocument3 pagesHammersmith Neonataljulianamd87No ratings yet
- Posterior Fossa Metaanalysis 2016 Part 2Document24 pagesPosterior Fossa Metaanalysis 2016 Part 2SahasraNo ratings yet
- Attention Process TrainingDocument22 pagesAttention Process TrainingLara Perez MurciaNo ratings yet
- INCLEN Diagnostic Tool For Epilepsy (INDT-EPI) For Primary Care Physicians: Development and ValidationDocument5 pagesINCLEN Diagnostic Tool For Epilepsy (INDT-EPI) For Primary Care Physicians: Development and ValidationAulya ArchuletaNo ratings yet
- Denver Developmental Screening Test - ValidityDocument7 pagesDenver Developmental Screening Test - Validitymodaberi1988No ratings yet
- Arizona Cognitive Test For DownDocument16 pagesArizona Cognitive Test For DownadriricaldeNo ratings yet
- 1 s2.0 S0890856709609552 MainDocument9 pages1 s2.0 S0890856709609552 Main서혜주No ratings yet
- Effects of A Neurodevelopmental Treatment Based.3Document13 pagesEffects of A Neurodevelopmental Treatment Based.3ivairmatiasNo ratings yet
- Clinical Tools Used in Young Infants Born Very Preterm To Predict Motor and Cognitive Delay (Not Cerebral Palsy) : A Systematic ReviewDocument9 pagesClinical Tools Used in Young Infants Born Very Preterm To Predict Motor and Cognitive Delay (Not Cerebral Palsy) : A Systematic ReviewAna paula CamargoNo ratings yet
- Assessment of Neurodisability and Malnutrition in Children in AfricaDocument8 pagesAssessment of Neurodisability and Malnutrition in Children in AfricaM.g. AlomiaNo ratings yet
- Asq3 PDFDocument6 pagesAsq3 PDFjanakaNo ratings yet
- Peds 2012-0900IDocument19 pagesPeds 2012-0900IAsma Ayad GhaziNo ratings yet
- Investigation of Global Developmental Delay: Evidence Based GuidelinesDocument5 pagesInvestigation of Global Developmental Delay: Evidence Based GuidelinesFirah Triple'sNo ratings yet
- Assessing Alzheimer's with cognitive testsDocument14 pagesAssessing Alzheimer's with cognitive testsLanna RegoNo ratings yet
- Dise Expert Consensus-Aao-2021Document14 pagesDise Expert Consensus-Aao-2021Alejandra Oliveros VargasNo ratings yet
- Fonseca Et Al. (2010) How To Increase Academic Performance in Children With Oppositional Defiant Disorder. An Implicit Theory EffectDocument4 pagesFonseca Et Al. (2010) How To Increase Academic Performance in Children With Oppositional Defiant Disorder. An Implicit Theory EffectAnonymous 86yt2cxMNo ratings yet
- Bosanquet Etal DMCN 2013Document9 pagesBosanquet Etal DMCN 2013ramopavelNo ratings yet
- Evaluation of The Child With Global Developmental DelayDocument14 pagesEvaluation of The Child With Global Developmental DelayplaincircleNo ratings yet
- 10.7556 Jaoa.1992.92.6.729Document16 pages10.7556 Jaoa.1992.92.6.729consueloamado.medNo ratings yet
- Dhawan 2016Document6 pagesDhawan 2016lilisNo ratings yet
- Evidencias VojtaDocument9 pagesEvidencias VojtaRommel AndresNo ratings yet
- Morgan 2013Document14 pagesMorgan 2013NéstorNo ratings yet
- Medical Decision Making Among Adolescents With Neonatal Brachial Plexus Palsy and Their Families: A Qualitative StudyDocument8 pagesMedical Decision Making Among Adolescents With Neonatal Brachial Plexus Palsy and Their Families: A Qualitative StudyPaoloLansangNo ratings yet
- Moeschler2014 PDFDocument18 pagesMoeschler2014 PDFFernando WijayaNo ratings yet
- Comparative Analysis of The WISC-IV in A Clinical Setting - ADHD vs. non-ADHDDocument7 pagesComparative Analysis of The WISC-IV in A Clinical Setting - ADHD vs. non-ADHDKarel GuevaraNo ratings yet
- Lippincott Williams & Wilkins: Info/about/policies/terms - JSPDocument14 pagesLippincott Williams & Wilkins: Info/about/policies/terms - JSPThayla Amorim SantinoNo ratings yet
- Growth and Health in Children With Moderate-to-Severe Cerebral PalsyDocument11 pagesGrowth and Health in Children With Moderate-to-Severe Cerebral PalsyNudyan BetharinaNo ratings yet
- Child Adoles Ment Health - 2010 - Holmes - The Diagnostic Utility of Executive Function Assessments in The Identification PDFDocument7 pagesChild Adoles Ment Health - 2010 - Holmes - The Diagnostic Utility of Executive Function Assessments in The Identification PDFJúlia JanoviczNo ratings yet
- Cognition Assessment Using The NIH Toolbox: "Nfsjdbo"Dbefnzpg/Fvspmphz6Obvuipsj (FesfqspevdujpopguijtbsujdmfjtqspijcjufeDocument12 pagesCognition Assessment Using The NIH Toolbox: "Nfsjdbo"Dbefnzpg/Fvspmphz6Obvuipsj (FesfqspevdujpopguijtbsujdmfjtqspijcjufeDenisse HuéramoNo ratings yet
- Care Pathways Early Diagnosis PrintDocument5 pagesCare Pathways Early Diagnosis PrintiannikkiNo ratings yet
- Neuropsychological and HOQ scores in childhood hydrocephalusDocument6 pagesNeuropsychological and HOQ scores in childhood hydrocephalusAnnisa HasnaNo ratings yet
- Neonatal Seizures: Current Management and Future ChallengesFrom EverandNeonatal Seizures: Current Management and Future ChallengesLakshmi NagarajanRating: 4 out of 5 stars4/5 (2)
- Pediatric Neuropsychiatry: A Case-Based ApproachFrom EverandPediatric Neuropsychiatry: A Case-Based ApproachAaron J. HauptmanNo ratings yet
- Acad Emerg Med 2007 p1114Document6 pagesAcad Emerg Med 2007 p1114Handris SupriadiNo ratings yet
- Modern Pathol 2006 p75Document8 pagesModern Pathol 2006 p75Handris SupriadiNo ratings yet
- Ad HTT 027 034 May18 07Document7 pagesAd HTT 027 034 May18 07Handris SupriadiNo ratings yet
- RetinaDocument58 pagesRetinaMegan ShanzuNo ratings yet
- Aafp PDFDocument8 pagesAafp PDFAnonymous umFOIQIMBANo ratings yet
- Microbiol Mol Biol Rev 2000 p461Document28 pagesMicrobiol Mol Biol Rev 2000 p461Handris SupriadiNo ratings yet
- Production and Contamination of Pasteurized Beverages Packed in Sealed Plastic Containers in Thailand and Potential Preventive MeasuresDocument9 pagesProduction and Contamination of Pasteurized Beverages Packed in Sealed Plastic Containers in Thailand and Potential Preventive MeasuresHandris SupriadiNo ratings yet
- Blood SpatterDocument79 pagesBlood SpatterHandris SupriadiNo ratings yet
- Ad HTT 027 034 May18 07Document7 pagesAd HTT 027 034 May18 07Handris SupriadiNo ratings yet
- Int Congress Series 2006 p834Document3 pagesInt Congress Series 2006 p834Handris SupriadiNo ratings yet
- Bpa 1Document1 pageBpa 1Handris SupriadiNo ratings yet
- BPA LGDocument1 pageBPA LGHandris SupriadiNo ratings yet
- J Substance Abuse Treat 2008 p215Document9 pagesJ Substance Abuse Treat 2008 p215Handris SupriadiNo ratings yet
- 2 Phisical ExaminationDocument76 pages2 Phisical ExaminationArdisa Permata PutriNo ratings yet
- Am Fam Physician 2005 p1353Document6 pagesAm Fam Physician 2005 p1353Handris SupriadiNo ratings yet
- Postgrad Med J 2004 p654Document7 pagesPostgrad Med J 2004 p654Handris SupriadiNo ratings yet
- Daun SirihDocument9 pagesDaun SirihAjid Hanif PurwantoNo ratings yet
- Arch Dis Child 2001 PF79Document4 pagesArch Dis Child 2001 PF79Handris SupriadiNo ratings yet
- Methadone Guidelines EnglishDocument64 pagesMethadone Guidelines EnglishHandris SupriadiNo ratings yet
- Can J Med 2003 p90Document8 pagesCan J Med 2003 p90Handris SupriadiNo ratings yet
- Cell Death Differentiation 2001 p1131Document3 pagesCell Death Differentiation 2001 p1131Handris SupriadiNo ratings yet
- 1628 6995 3 PBDocument20 pages1628 6995 3 PBRio Riahman SitepuNo ratings yet
- Cell Death Differentiation 2001 p1131Document3 pagesCell Death Differentiation 2001 p1131Handris SupriadiNo ratings yet
- Paranoid Schizophrenia: What You Should KnowDocument50 pagesParanoid Schizophrenia: What You Should KnowHandris SupriadiNo ratings yet
- Am J Public Health 1999 p662Document4 pagesAm J Public Health 1999 p662Handris SupriadiNo ratings yet
- Antimicrob Agents Chemother 2007 p110Document9 pagesAntimicrob Agents Chemother 2007 p110Handris SupriadiNo ratings yet
- Eur J Personality 1997 p101Document32 pagesEur J Personality 1997 p101Handris SupriadiNo ratings yet
- Am Fam Physician 2005 p1353Document6 pagesAm Fam Physician 2005 p1353Handris SupriadiNo ratings yet
- Artigo 13 - DM GestacionalDocument8 pagesArtigo 13 - DM GestacionalfahlevyNo ratings yet
- J Fam Therapy 1981 p21Document10 pagesJ Fam Therapy 1981 p21Handris SupriadiNo ratings yet
- Management Accounting ResearchDocument3 pagesManagement Accounting Researchali asgharNo ratings yet
- The Power of Courtesy: How Politeness Can Gain Respect, Inspire Kindness and Strengthen RelationshipsDocument3 pagesThe Power of Courtesy: How Politeness Can Gain Respect, Inspire Kindness and Strengthen Relationshipswardah farainNo ratings yet
- k-2 EngineeringDocument1 pagek-2 Engineeringapi-235408695No ratings yet
- What S in A Name Exploring Pansexuality OnlineDocument16 pagesWhat S in A Name Exploring Pansexuality OnlineBrendaNo ratings yet
- Curriculum Design Principles for Effective Teaching and LearningDocument5 pagesCurriculum Design Principles for Effective Teaching and LearningPatrick kenneth GacayanNo ratings yet
- Automated MPS and Item Analysis Workbook InstructionsDocument68 pagesAutomated MPS and Item Analysis Workbook Instructionscharlene albateraNo ratings yet
- Lukacs' Reification and the Proletariat's Class ConsciousnessDocument44 pagesLukacs' Reification and the Proletariat's Class ConsciousnessDaniel SchwartzNo ratings yet
- Understanding Cognitive BiasesDocument3 pagesUnderstanding Cognitive BiasesEd Gerard AquinoNo ratings yet
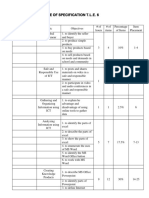
- Table of Specification T.L.E. 6Document3 pagesTable of Specification T.L.E. 6Autumn Thorn SebastianNo ratings yet
- 5 - Concluding Sentence - Lesson PracticeDocument3 pages5 - Concluding Sentence - Lesson Practiceismail mllNo ratings yet
- Research ProposalDocument5 pagesResearch ProposalLueween Acay CansinoNo ratings yet
- Programmed LearningDocument18 pagesProgrammed LearningRukhsana KhanNo ratings yet
- Rebuilding the Economic SystemDocument4 pagesRebuilding the Economic SystemMiodrag Mijatovic100% (1)
- CLC What Makes A High PotentialDocument20 pagesCLC What Makes A High PotentialxavierxandersNo ratings yet
- Maryane Jhudiel Tibar Hofileña: SkillsDocument2 pagesMaryane Jhudiel Tibar Hofileña: SkillsVirgie Hofileña FaustinoNo ratings yet
- Effects of Internet AddictionDocument14 pagesEffects of Internet AddictionHeraHeccateNo ratings yet
- 2012 - Job Profile - Field Service Engineer FSEDocument2 pages2012 - Job Profile - Field Service Engineer FSEskybmeNo ratings yet
- MY FINAL DEMO & For ApplicationDocument6 pagesMY FINAL DEMO & For ApplicationRica Mae AnciadoNo ratings yet
- Children's Use of Technology and Social MediaDocument5 pagesChildren's Use of Technology and Social MediaJunel SildoNo ratings yet
- BSD Outside Learning Permission FormDocument2 pagesBSD Outside Learning Permission FormihappyscribdNo ratings yet
- MRF ProjectDocument78 pagesMRF ProjectPrem Raj33% (3)
- The Trickster MythDocument39 pagesThe Trickster MythLJ100% (1)
- Inflectional MorphologyDocument37 pagesInflectional MorphologyFriadmo SaragihNo ratings yet
- Modern Japan culture and society seminar scheduleDocument1 pageModern Japan culture and society seminar scheduleIao MoaNo ratings yet
- BEE COUNTY - Beeville Isd - 2009 Texas School Survey of Drug and Alcohol UseDocument249 pagesBEE COUNTY - Beeville Isd - 2009 Texas School Survey of Drug and Alcohol Use2009 Texas School Survey of Drug and Alcohol UseNo ratings yet
- Learning Competency (Essential Competency) : English 9 Quarter 2 Week 6Document6 pagesLearning Competency (Essential Competency) : English 9 Quarter 2 Week 6Heidee BasasNo ratings yet