You might also like
- Form No. 10iDocument2 pagesForm No. 10iTempuserNo ratings yet
- Form No 10Document2 pagesForm No 10javedmonis07No ratings yet
- DMF Ceftriaxone Sodium USPDocument94 pagesDMF Ceftriaxone Sodium USPArebuNo ratings yet
- Module 2Document36 pagesModule 2Mariela Lopez huamanNo ratings yet
- RecieptDocument1 pageRecieptGihanNo ratings yet
- TaxExemptionCertificate73079CC DN 357172Document1 pageTaxExemptionCertificate73079CC DN 357172Asif EbrahimNo ratings yet
- UPAY - Donation ReceiptDocument1 pageUPAY - Donation Receiptprescongoa.ikigaiNo ratings yet
- 1q2010type2activetext (DMF Sources)Document460 pages1q2010type2activetext (DMF Sources)thakkar_dhNo ratings yet
- Donation - Nov 2023 - 80GDocument1 pageDonation - Nov 2023 - 80Grohit.kedareNo ratings yet
- Credila Loan Application Form WeDocument2 pagesCredila Loan Application Form WeAditya MahoreNo ratings yet
- Appointment RecieptDocument3 pagesAppointment Recieptsiva5256No ratings yet
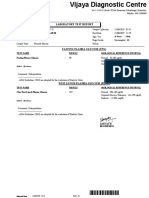
- Test Description Value(s) Unit(s) Reference Range: Pt/InrDocument2 pagesTest Description Value(s) Unit(s) Reference Range: Pt/InrSuhas KapseNo ratings yet
- Dengue: Subjective FindingsDocument5 pagesDengue: Subjective FindingsRaghu VenkatNo ratings yet
- LTA Declaration Form Period Ended 31.dec.2013Document1 pageLTA Declaration Form Period Ended 31.dec.2013Paymaster ServicesNo ratings yet
- Molecular Analysis For Qualitative Detection of Sars-Cov-2.: Negative Negative Negative PassDocument4 pagesMolecular Analysis For Qualitative Detection of Sars-Cov-2.: Negative Negative Negative PassmeezNo ratings yet
- 06 May 2017 221509117EF8XS16XAnnexure-Prefeasibilityreport PDFDocument109 pages06 May 2017 221509117EF8XS16XAnnexure-Prefeasibilityreport PDFjyothiNo ratings yet
- Lab Report NewDocument3 pagesLab Report Newhacebe2685No ratings yet
- Module 2Document114 pagesModule 2Ram YadavNo ratings yet
- Laboratory Test Report: Test Name Result Sars-Cov-2 (RDRP Gene)Document5 pagesLaboratory Test Report: Test Name Result Sars-Cov-2 (RDRP Gene)Imran AhmedNo ratings yet
- Drug Master FileDocument21 pagesDrug Master FileAbhijit kanavajeNo ratings yet
- Lucknow Mumbai: Sqvwyc CompleteDocument6 pagesLucknow Mumbai: Sqvwyc Completepawan guptaNo ratings yet
- Adamjee In-Patient Claim Reimbursement FormDocument2 pagesAdamjee In-Patient Claim Reimbursement Formhashamqazi100% (1)
- HHeparin API Manufacturers - Suppliers - Drug Master Files (DMF) - CEPDocument33 pagesHHeparin API Manufacturers - Suppliers - Drug Master Files (DMF) - CEPShahid HasanNo ratings yet
- Haematology Test Result Unit Biological Ref. Interval Prothrombin TimeDocument6 pagesHaematology Test Result Unit Biological Ref. Interval Prothrombin TimeNidhi RakeshNo ratings yet
- SanctionDocument6 pagesSanctionKriti GoodNo ratings yet
- Opdbills 4950545655505348Document1 pageOpdbills 4950545655505348Koshindar GaurNo ratings yet
- CT Scan Chest: Radiology Imaging DepartmentDocument1 pageCT Scan Chest: Radiology Imaging DepartmentDrehsan MemonNo ratings yet
- Error Codes On Biometric Attendance System (BAS)Document2 pagesError Codes On Biometric Attendance System (BAS)Naren Jamadar100% (1)
- PrescriptionDocument2 pagesPrescriptionMercy AngelinNo ratings yet
- DMLT CertificateDocument2 pagesDMLT CertificateZeeshan Ansari50% (2)
- Ambulance BillDocument4 pagesAmbulance Billanon-953784No ratings yet
- JWALADocument2 pagesJWALAVaid Navdeep Singh100% (1)
- Medical CertificateDocument5 pagesMedical CertificatePrasanna VenkatNo ratings yet
- RT PCR Test ReportDocument2 pagesRT PCR Test ReportMoumita MandalNo ratings yet
- Flight TicketDocument1 pageFlight TicketControl Advertising SolutionsNo ratings yet
- TEST(s) Normal UNIT(s)Document1 pageTEST(s) Normal UNIT(s)Ahad Siddique100% (1)
- All India Institute of Medical Sciences (Aiims) : Laboratory Observation ReportDocument2 pagesAll India Institute of Medical Sciences (Aiims) : Laboratory Observation ReportPiyush TripathiNo ratings yet
- Government of Andhrapradesh Identity Card For Person With DisabilityDocument1 pageGovernment of Andhrapradesh Identity Card For Person With DisabilitykalavaguntasachivalayamNo ratings yet
- Man Ishta MtaDocument2 pagesMan Ishta MtaDhairya TamtaNo ratings yet
- Diagnostic Report: Patient Name: Gopal Mondal GOPAM301119980 0002UF026577Document2 pagesDiagnostic Report: Patient Name: Gopal Mondal GOPAM301119980 0002UF026577world one AR BABUNo ratings yet
- CMC Vellore AccomodationDocument7 pagesCMC Vellore Accomodationhelpbgp0% (1)
- Star Health and Allied Insurance Company Limited Tariff Statement - Mini SOC (FINALISED)Document1 pageStar Health and Allied Insurance Company Limited Tariff Statement - Mini SOC (FINALISED)Sanket Sahare100% (1)
- Radiology Report-R5016547Document4 pagesRadiology Report-R5016547Rajeev SNo ratings yet
- DR Kedia Covering Letter PNDTDocument2 pagesDR Kedia Covering Letter PNDTAlok KediaNo ratings yet
- Z3rk4o00mfhmkk5mwrjowdDocument2 pagesZ3rk4o00mfhmkk5mwrjowdVarun GognaNo ratings yet
- Surname AGE Hospital CODE:0000585 HOSPITAL NO.9013115 Given Name SEX Ward / Room Fmw3Document2 pagesSurname AGE Hospital CODE:0000585 HOSPITAL NO.9013115 Given Name SEX Ward / Room Fmw3Gerald AndersonNo ratings yet
- Hospital Document Tariff Statement (Mini SOC)Document1 pageHospital Document Tariff Statement (Mini SOC)Deepak KaushikNo ratings yet
- Form of Essentiality Certificate B PDFDocument2 pagesForm of Essentiality Certificate B PDFAnji KaringuNo ratings yet
- Star Health and Allied Insurance Co. LTD: Hospital Empanelment Request FormDocument2 pagesStar Health and Allied Insurance Co. LTD: Hospital Empanelment Request FormDeepak Kaushik0% (1)
- S14 - FPSC Rakesh Marg J-3, Pushpanjali Complex, Nehru Nagar Rakesh Marg, Ghaziabad-Utp, IndDocument2 pagesS14 - FPSC Rakesh Marg J-3, Pushpanjali Complex, Nehru Nagar Rakesh Marg, Ghaziabad-Utp, Indvijay rastogiNo ratings yet
- 22/03/2023 Millat Nursing Home 23/03/2023 14:11:47 15:29:25 22/03/2023 15:29:25Document2 pages22/03/2023 Millat Nursing Home 23/03/2023 14:11:47 15:29:25 22/03/2023 15:29:25Sony YadavNo ratings yet
- Patient 15-c20721 Bcr-Abl Quali ReportDocument4 pagesPatient 15-c20721 Bcr-Abl Quali ReportNishant Kumar GuptaNo ratings yet
- Total QAR8.00: Thanks For Riding, GeorgeDocument3 pagesTotal QAR8.00: Thanks For Riding, GeorgegeorgeNo ratings yet
- WRUV7926Document3 pagesWRUV7926rajashekarcse533No ratings yet
- 19 Dec 2022Document1 page19 Dec 2022Yogesh ArasuNo ratings yet
- S P VashistDocument27 pagesS P VashistGhissu GangNo ratings yet
- Department of Molecular Biology. Covid 19 RTPCR With Home Collection Test Name Result Unit Bio. Ref. Range MethodDocument2 pagesDepartment of Molecular Biology. Covid 19 RTPCR With Home Collection Test Name Result Unit Bio. Ref. Range Methodmaneesh babuNo ratings yet
- Age/Sex: 20/m: Covid-19 RT PCRDocument2 pagesAge/Sex: 20/m: Covid-19 RT PCRRoamer MalluNo ratings yet
- Consent Form Aadhaar Seeding in EnglishDocument1 pageConsent Form Aadhaar Seeding in EnglishPranab Prajapati0% (1)
- IT Section 80DDBDocument3 pagesIT Section 80DDBnm.namitamishraNo ratings yet
- Provisional Interest Certificate - 56465233 - 221527539Document1 pageProvisional Interest Certificate - 56465233 - 221527539dinesh makwanaNo ratings yet
- Form XDocument1 pageForm Xdinesh makwanaNo ratings yet
- Data - Investment Proofs - 2022-23Document15 pagesData - Investment Proofs - 2022-23dinesh makwanaNo ratings yet
- Mehul ParmarDocument2 pagesMehul Parmardinesh makwanaNo ratings yet
- NRS 2109 Revised Pharma Syllabus AY 2020 2021Document48 pagesNRS 2109 Revised Pharma Syllabus AY 2020 2021Julianne Kyla MercadoNo ratings yet
- Toaz - Info LLB Notes Mumbai University Law Amp Medicine Confidentiality PRDocument3 pagesToaz - Info LLB Notes Mumbai University Law Amp Medicine Confidentiality PRVandana BhatNo ratings yet
- PHINMA University of Pangasinan College of Health Sciences Nursing Care PlanDocument2 pagesPHINMA University of Pangasinan College of Health Sciences Nursing Care PlanJoeriel MontemayorNo ratings yet
- Diagnostic Ultrasound System T3300 Operating Instructions en v1.894Document146 pagesDiagnostic Ultrasound System T3300 Operating Instructions en v1.894Harold James BoyrasNo ratings yet
- Somanabolic+Muscle+Maximizer+PDF+ +eBook+Free+Download+Kyle+LeonDocument34 pagesSomanabolic+Muscle+Maximizer+PDF+ +eBook+Free+Download+Kyle+LeonAaron BarclayNo ratings yet
- 2014 BJM MeowsDocument7 pages2014 BJM MeowshendraNo ratings yet
- HSE Management Standards Indicator ToolDocument3 pagesHSE Management Standards Indicator ToolOllie EvansNo ratings yet
- Community Medicine Osce ReviewersDocument2 pagesCommunity Medicine Osce ReviewersJoy FucananNo ratings yet
- Non Insti FinalDocument7 pagesNon Insti FinalJames BoundNo ratings yet
- Eye Infection and Blepharitis by MHSNDocument18 pagesEye Infection and Blepharitis by MHSNMhsn0% (1)
- 1 PDFDocument359 pages1 PDFHira PujariNo ratings yet
- DAY 1 Work Immersion JournalDocument2 pagesDAY 1 Work Immersion JournalJerome Rex SantosNo ratings yet
- Books by Robie H. HarrisDocument2 pagesBooks by Robie H. HarrisCandlewick PressNo ratings yet
- Atlas of Clinical Ophthalmology 2nd Edition (2013)Document506 pagesAtlas of Clinical Ophthalmology 2nd Edition (2013)bogdasus75% (4)
- Inguinal Hernias in Adults Epidemiological Clinical and Therapeutic AspectsDocument24 pagesInguinal Hernias in Adults Epidemiological Clinical and Therapeutic AspectsmutmainnahNo ratings yet
- Jurnal Penelitian KBDocument6 pagesJurnal Penelitian KBMaya Ulfah apriliyaNo ratings yet
- 10 1016@j Childyouth 2019 104649Document39 pages10 1016@j Childyouth 2019 104649Vanessa AydinanNo ratings yet
- Physiology Behind Contraceptive MethodsDocument26 pagesPhysiology Behind Contraceptive Methodsnirilib100% (2)
- SynlanDocument3 pagesSynlanAreli AltamiranoNo ratings yet
- KI Health 75th FinalDocument127 pagesKI Health 75th FinalChandrimaChatterjeeNo ratings yet
- Cardiology BookDocument401 pagesCardiology BookOana100% (5)
- Miscellaneous Gi DrugsDocument7 pagesMiscellaneous Gi DrugsJanelle BondadNo ratings yet
- Brine Shrimp Lethality AssayDocument5 pagesBrine Shrimp Lethality AssayEnzo TimbolNo ratings yet
- Assignment 3: Final Project - Comprehensive Literature ReviewDocument18 pagesAssignment 3: Final Project - Comprehensive Literature ReviewJay JalaliNo ratings yet
- Jurnal 4Document2 pagesJurnal 4PDPPSNS2M1022 Nur Liyana Syamimi Binti Mohd AzmanNo ratings yet
- The Juiceman's Power of Juicing PDF by Jay KordichDocument292 pagesThe Juiceman's Power of Juicing PDF by Jay Kordichpdf ebook free download95% (19)
- Covid Treatment PresentationDocument36 pagesCovid Treatment PresentationSr. Section Engineer Coaching Depot-ValsadNo ratings yet
- Table 1 Clinical Handover Solutions Matrix Sept 2014Document1 pageTable 1 Clinical Handover Solutions Matrix Sept 2014Dewi Ratna SariNo ratings yet
- Tahun 2022 - Stok Fix BHP..Document28 pagesTahun 2022 - Stok Fix BHP..Hanaya beauty0% (1)
- DM Health Teaching PlanDocument5 pagesDM Health Teaching PlancamilatanNo ratings yet