You might also like
- DSM-IV Adult ADHD Symptom Checklist-Self Report Version # 6182Document1 pageDSM-IV Adult ADHD Symptom Checklist-Self Report Version # 6182Chris0% (1)
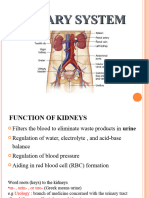
- Chapter 57 Introduction To The Urinary SystemDocument24 pagesChapter 57 Introduction To The Urinary SystemtikkimarshallNo ratings yet
- Urinary Tract Disorders, PowerpointDocument63 pagesUrinary Tract Disorders, Powerpointmutia mutia100% (4)
- Epilepsy (Gregory D. Cascino, Joseph I. Sirven Etc.)Document514 pagesEpilepsy (Gregory D. Cascino, Joseph I. Sirven Etc.)Georgiana Frunza100% (1)
- Metabolism of CarbohydratesDocument26 pagesMetabolism of CarbohydratesMM Qizill67% (3)
- Retina 2011 SyllabusDocument191 pagesRetina 2011 SyllabusAnyun NyunNo ratings yet
- Renal and Genitourinary ConditionsDocument139 pagesRenal and Genitourinary ConditionsjustinahorroNo ratings yet
- 5-The Urinary SystemDocument4 pages5-The Urinary SystemEma FröhlichováNo ratings yet
- Introduction To UrologyDocument48 pagesIntroduction To UrologyvaiyenNo ratings yet
- Two Kidneys: Extract Waste From The Blood and Balance Body FluidDocument5 pagesTwo Kidneys: Extract Waste From The Blood and Balance Body FluidDani PhilipNo ratings yet
- Urinary System (Complaints, Disorders, First Aid Measures)Document61 pagesUrinary System (Complaints, Disorders, First Aid Measures)David Badaru100% (1)
- Urinary CatheterizationDocument17 pagesUrinary CatheterizationLeofe CorregidorNo ratings yet
- HematuriaDocument86 pagesHematuriaMohamad Arif MustaphaNo ratings yet
- Urinary SystemDocument27 pagesUrinary Systemtareqhaddad123No ratings yet
- Obstructive Uropathy & Urinary Tract CalculiDocument55 pagesObstructive Uropathy & Urinary Tract CalculiNorFarah Fatin AnuarNo ratings yet
- Urinary System DisordersDocument14 pagesUrinary System DisordersGideon P. CasasNo ratings yet
- Urinary System and DisordersDocument22 pagesUrinary System and Disorders143bbNo ratings yet
- Storing A Urine SampleDocument8 pagesStoring A Urine SampleMarz DempseyNo ratings yet
- 3.modern ReviewDocument19 pages3.modern ReviewKrishnaNo ratings yet
- Introduction in UrologyDocument69 pagesIntroduction in UrologyKaram SaadNo ratings yet
- Urology: Schwartz's Principles of Surgery 11th EdDocument34 pagesUrology: Schwartz's Principles of Surgery 11th EdaddelinsNo ratings yet
- Ivp Intravenous PyelographyDocument16 pagesIvp Intravenous PyelographyLuisa ManaloNo ratings yet
- MED2 2022 (Autosaved)Document33 pagesMED2 2022 (Autosaved)Adakun SamuelNo ratings yet
- Physical Examination and Health Assessment: Genitourinary SystemDocument134 pagesPhysical Examination and Health Assessment: Genitourinary Systemmesfin DemiseNo ratings yet
- Urinary Disorders 2Document19 pagesUrinary Disorders 2ula mdiNo ratings yet
- Disorders of The Genitourinary SystemDocument100 pagesDisorders of The Genitourinary SystemMurti GutoNo ratings yet
- Urinary SystemDocument25 pagesUrinary Systembessan alfqeatNo ratings yet
- Sistemul RENALDocument108 pagesSistemul RENALAndrada OargăNo ratings yet
- Human Excretory SystemDocument51 pagesHuman Excretory SystemVinoj MnoNo ratings yet
- Urology For Medical Student Hora 19-12-2008Document77 pagesUrology For Medical Student Hora 19-12-2008Adriana SantosNo ratings yet
- TolitsDocument42 pagesTolitsAzela TuzonNo ratings yet
- Les 3Document19 pagesLes 3Dike Obiora-EzeNo ratings yet
- Clinical Examination of Genitourinary SystemDocument43 pagesClinical Examination of Genitourinary SystemKeamina .aNo ratings yet
- 161 - B3 Sesi 3 Asisten 2015Document74 pages161 - B3 Sesi 3 Asisten 2015Luthfi AnshoriNo ratings yet
- Evaluasi Fungsi Berkemih Dan Defikasi - LisaDocument37 pagesEvaluasi Fungsi Berkemih Dan Defikasi - LisaHeather BrownNo ratings yet
- Anatomy of The Urinary SystemDocument24 pagesAnatomy of The Urinary Systemgaylmm100% (2)
- Nursing Genito-Urinary SystemDocument109 pagesNursing Genito-Urinary SystemKenny Nadela100% (1)
- Bladder DiverticulaDocument23 pagesBladder DiverticulaJeanette CallejasNo ratings yet
- Alteration in Urinary System - ppt22222Document117 pagesAlteration in Urinary System - ppt22222yen1988No ratings yet
- 313 - Disorders of Renal and Urinary SystemsDocument8 pages313 - Disorders of Renal and Urinary SystemsChrissy Mendoza100% (2)
- Elimination NeedsDocument52 pagesElimination NeedsKhadija JaraNo ratings yet
- Kub Gyne Anemia PDFDocument117 pagesKub Gyne Anemia PDFWaterfall ShapelessNo ratings yet
- Gangguan Sistem Perkemihan: DR A. Yuda Handaya, SPB, Finacs, FmasDocument132 pagesGangguan Sistem Perkemihan: DR A. Yuda Handaya, SPB, Finacs, FmasRobby Wiranata WijayaNo ratings yet
- Urology Notes 1Document43 pagesUrology Notes 1Shazaan NadeemNo ratings yet
- Renal Urinary SystemDocument115 pagesRenal Urinary SystemBenjomar CalderonNo ratings yet
- Urine System 1Document11 pagesUrine System 1api-283243804No ratings yet
- Renal System (Output)Document30 pagesRenal System (Output)Tiffy SuarezNo ratings yet
- Presentation2 URINARYDocument16 pagesPresentation2 URINARYEunice HandigNo ratings yet
- Investigation JF The Urinary TractDocument139 pagesInvestigation JF The Urinary TractВладимир КурпаянидиNo ratings yet
- Obstructive Uropathy: Nitha. K 2 Year MSC NursingDocument67 pagesObstructive Uropathy: Nitha. K 2 Year MSC NursingNITHA KNo ratings yet
- Urinary Elimination: (Midterm)Document14 pagesUrinary Elimination: (Midterm)Mina RacadioNo ratings yet
- BLadder Outlet ObstructionDocument28 pagesBLadder Outlet ObstructionCodillia Cheong100% (1)
- GenitoUrinary Tract PresentationDocument60 pagesGenitoUrinary Tract PresentationJaezee RamosNo ratings yet
- Imaging of The Genitourinary TractDocument86 pagesImaging of The Genitourinary TractNor AinaNo ratings yet
- Urinary Symptoms and InvestigationsDocument16 pagesUrinary Symptoms and Investigationsمبدر حامدNo ratings yet
- Turbt 2Document80 pagesTurbt 2Windelyn GamaroNo ratings yet
- Inkontinensia UrinDocument24 pagesInkontinensia UrinBenny Wegah Nulis100% (9)
- Urinary System: TH RDDocument13 pagesUrinary System: TH RDdlneisha61No ratings yet
- Pelvic Anatomy Slides FINALDocument36 pagesPelvic Anatomy Slides FINALRajashekharNo ratings yet
- Imaging in Genitourinary System - 17 Agustus 2013 - by Robby HermawanDocument80 pagesImaging in Genitourinary System - 17 Agustus 2013 - by Robby HermawanFitria Dewi LestariNo ratings yet
- Clinical Case HomeworkDocument4 pagesClinical Case HomeworkIris BakerNo ratings yet
- Hematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesFrom EverandHematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesRating: 5 out of 5 stars5/5 (2)
- Resume 2Document2 pagesResume 2api-576574115No ratings yet
- Date Cues NSG Dx. Scientific Basis Goal of Care NSG Intervention Rationale Outcome Criteria EvaluationDocument3 pagesDate Cues NSG Dx. Scientific Basis Goal of Care NSG Intervention Rationale Outcome Criteria EvaluationWenalyn Grace Abella LlavanNo ratings yet
- AbortionDocument29 pagesAbortionMujeeb Choudhary100% (2)
- Addenbrooke Cognitive ExaminationDocument11 pagesAddenbrooke Cognitive ExaminationAshlin BaijuNo ratings yet
- Supplementary Materials Supplementary Table Complications Meddra Preferred Term, N (%) Working Ability Recovered N 122 Working Ability Not Recovered N 91Document9 pagesSupplementary Materials Supplementary Table Complications Meddra Preferred Term, N (%) Working Ability Recovered N 122 Working Ability Not Recovered N 91Perdana SihiteNo ratings yet
- Discoid MeniscusDocument22 pagesDiscoid Meniscusonehipsa0% (1)
- Hemorrhagic StrokeDocument30 pagesHemorrhagic StrokeAstrina SupandyNo ratings yet
- Acute Chronic GlomerulonephritisDocument37 pagesAcute Chronic GlomerulonephritisMadeline Jessica HuwaeNo ratings yet
- List of Medical AbbreviationsDocument16 pagesList of Medical AbbreviationsClaire Nimor VentulanNo ratings yet
- English Homework 4Document2 pagesEnglish Homework 4Teodora TanaseNo ratings yet
- Raynauds DiseaseDocument13 pagesRaynauds Diseaseapi-3718174100% (3)
- Training Manual PsychologistsDocument75 pagesTraining Manual PsychologistsNagarjuna KalimisettyNo ratings yet
- Ans. Xanthelasma Answer Peripheral CyanosisDocument2 pagesAns. Xanthelasma Answer Peripheral CyanosisJordan Abosama MamalumpongNo ratings yet
- J of Clinical Hypertension - 2021 - Ona - Executive Summary of The 2020 Clinical Practice Guidelines For The Management ofDocument14 pagesJ of Clinical Hypertension - 2021 - Ona - Executive Summary of The 2020 Clinical Practice Guidelines For The Management ofsefigi6746No ratings yet
- Robert Koch - Britannica Online EncyclopediaDocument2 pagesRobert Koch - Britannica Online EncyclopediakamilapufflerovaNo ratings yet
- PepDocument8 pagesPepUdayakrishnan P Kanhangad100% (1)
- Wound DebridementDocument21 pagesWound DebridementKrisna MuhammadNo ratings yet
- NP3 PreboardsDocument15 pagesNP3 PreboardsRamon Carlo Almiranez100% (2)
- General Principles of Periodontal SurgeryDocument33 pagesGeneral Principles of Periodontal SurgeryAnuj Singh PariharNo ratings yet
- Poster AbstractsDocument1 pagePoster Abstractsapi-295354451No ratings yet
- Chapter 3 3 1 First Line of DefenseDocument33 pagesChapter 3 3 1 First Line of Defenseapi-237856591No ratings yet
- Sindrome de ReyeDocument5 pagesSindrome de ReyecdsaludNo ratings yet
- Virocon 2021 FlyerDocument7 pagesVirocon 2021 FlyerAnand ChaubeyNo ratings yet
- Anemii HemoliticeDocument74 pagesAnemii HemoliticeCNo ratings yet
- Dengue JournalDocument4 pagesDengue JournalRohitKumarNo ratings yet
- APPENDIX P SAMPLE Discharge Instructions Following Delivery With Diagnosed PreeclampsiaDocument1 pageAPPENDIX P SAMPLE Discharge Instructions Following Delivery With Diagnosed PreeclampsiaglyadpadNo ratings yet