You might also like
- 7 Steps To Discovering Your Personal Values - Scott Jeffrey PDFDocument9 pages7 Steps To Discovering Your Personal Values - Scott Jeffrey PDFtraketeoNo ratings yet
- Perio-Ortho Symbiosis: A Review Article: Dr. Apeksha Ghai and Dr. Mayur KaushikDocument3 pagesPerio-Ortho Symbiosis: A Review Article: Dr. Apeksha Ghai and Dr. Mayur Kaushikmohammad naufalNo ratings yet
- SplintingDocument40 pagesSplintingrupaliNo ratings yet
- Ortho Perio NewDocument5 pagesOrtho Perio NewNingombam Robinson SinghNo ratings yet
- I Love You But I M Not in Love With YouDocument31 pagesI Love You But I M Not in Love With YouRaluca CotetiuNo ratings yet
- Mariyam Zehra PG 1St Year Department of OrthodonticsDocument101 pagesMariyam Zehra PG 1St Year Department of OrthodonticsMariyam67% (3)
- NSAIDS in Dentistry It's Principles in PracticeDocument6 pagesNSAIDS in Dentistry It's Principles in PracticeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Yasmeen Sitxfa002Document35 pagesYasmeen Sitxfa002ranu jain100% (1)
- Minor Periodontal Surgery in OrthoDocument6 pagesMinor Periodontal Surgery in OrthoJuanCarlosViverosCórdovaNo ratings yet
- Manuscript BodyDocument11 pagesManuscript BodyKatherine TerronesNo ratings yet
- Pdflib Plop: PDF Linearization, Optimization, Protection Page Inserted by Evaluation VersionDocument10 pagesPdflib Plop: PDF Linearization, Optimization, Protection Page Inserted by Evaluation VersionHARITHA H.PNo ratings yet
- Pdflib Plop: PDF Linearization, Optimization, Protection Page Inserted by Evaluation VersionDocument10 pagesPdflib Plop: PDF Linearization, Optimization, Protection Page Inserted by Evaluation VersionJoshua MartinNo ratings yet
- Pdflib Plop: PDF Linearization, Optimization, Protection Page Inserted by Evaluation VersionDocument10 pagesPdflib Plop: PDF Linearization, Optimization, Protection Page Inserted by Evaluation VersionMonojit DuttaNo ratings yet
- Krishnan 2006Document10 pagesKrishnan 2006Shatabdi A ChakravartyNo ratings yet
- Drugs in Orthodontics - A ReviewDocument7 pagesDrugs in Orthodontics - A ReviewRicha AhlawatNo ratings yet
- Drugs in Orthodontics: G.Shekar Subramanian Ist Year PGDocument69 pagesDrugs in Orthodontics: G.Shekar Subramanian Ist Year PGShekar SubramanianNo ratings yet
- NSAIDs in Orthodontic Tooth Movement, 2012Document4 pagesNSAIDs in Orthodontic Tooth Movement, 2012Tarif HamshoNo ratings yet
- Drug Therapy in OrthodonticsDocument4 pagesDrug Therapy in OrthodonticsRicha AhlawatNo ratings yet
- Effects of Drugs in Orthodontic Tooth Movement: A ReviewDocument6 pagesEffects of Drugs in Orthodontic Tooth Movement: A ReviewvprakshaindiaNo ratings yet
- 2019 Modulation - of - Various - Biomarkers - Under - The - EffectDocument6 pages2019 Modulation - of - Various - Biomarkers - Under - The - EffectricardoNo ratings yet
- The Potential Use of Pharmacological Agents To Modulate Orthodontic Tooth Movement (OTM)Document9 pagesThe Potential Use of Pharmacological Agents To Modulate Orthodontic Tooth Movement (OTM)vprakshaindiaNo ratings yet
- Drugs OrthodDocument9 pagesDrugs OrthoddrmeenugargNo ratings yet
- NSAID Side EffectDocument8 pagesNSAID Side EffectMohamed FaizalNo ratings yet
- The Use of Different Analgesics in Orthodontic Tooth Movements, Angle EgyptionDocument7 pagesThe Use of Different Analgesics in Orthodontic Tooth Movements, Angle EgyptionTarif HamshoNo ratings yet
- Methods of Accelerating Orthodontic Tooth MovementDocument10 pagesMethods of Accelerating Orthodontic Tooth MovementJuan AndradeNo ratings yet
- Drugs in Orthodontics - 1Document43 pagesDrugs in Orthodontics - 1Sushma Rayal SANo ratings yet
- Idt 2013 Jbs Bisphosphonates (J Suzuki)Document6 pagesIdt 2013 Jbs Bisphosphonates (J Suzuki)SanNo ratings yet
- Qi 32 5 Tyrovola 6Document7 pagesQi 32 5 Tyrovola 6Ortodoncia 1No ratings yet
- The Effects of Commonly Used Drugs On Orthodontic Tooth Movement: A Systematic ReviewDocument5 pagesThe Effects of Commonly Used Drugs On Orthodontic Tooth Movement: A Systematic ReviewvprakshaindiaNo ratings yet
- Systemic MedicationsDocument8 pagesSystemic MedicationsGonzalo Báez VNo ratings yet
- Asprin Salicylate Therapy Decreases Bone Resorption by InhiDocument3 pagesAsprin Salicylate Therapy Decreases Bone Resorption by InhiAyesha AyyazNo ratings yet
- Effects of Physical Stimulation in The Field of Oral HealthDocument17 pagesEffects of Physical Stimulation in The Field of Oral HealthsovalaxNo ratings yet
- 1150JPIS - Jpis 50 68Document6 pages1150JPIS - Jpis 50 68Louis HutahaeanNo ratings yet
- 1 s2.0 S094096021830089X MainDocument8 pages1 s2.0 S094096021830089X MainDANTE DELEGUERYNo ratings yet
- BifosfonatosyortodonciaDocument8 pagesBifosfonatosyortodonciavivigaitanNo ratings yet
- Accelerated OrthodonticsDocument95 pagesAccelerated Orthodonticsobula reddyNo ratings yet
- Medication and Orthodontic Tooth MovementDocument6 pagesMedication and Orthodontic Tooth MovementJuan Andres CastilloNo ratings yet
- Tooth Socket HealingDocument16 pagesTooth Socket HealingluisNo ratings yet
- Articol Acidul ZoledronicDocument13 pagesArticol Acidul ZoledronicAndreea GorbanescuNo ratings yet
- Catch It Right - A Case Report On Occlusal SplintDocument6 pagesCatch It Right - A Case Report On Occlusal SplintSkAliHassanNo ratings yet
- Ortho-Perio Synergy - A Review: Crimson PublishersDocument8 pagesOrtho-Perio Synergy - A Review: Crimson PublishersJoshua Diaz QuiquijanaNo ratings yet
- Teriparatide - The Future Ofhost Modulation Andperiodontal Regeneration? A Short ReviewDocument3 pagesTeriparatide - The Future Ofhost Modulation Andperiodontal Regeneration? A Short ReviewIJAR JOURNALNo ratings yet
- Seminar Canine Impaction: Dr. Shubham Sharan Post-Graduate Student Department of Orthodontics &dentofacialorthopaedicsDocument24 pagesSeminar Canine Impaction: Dr. Shubham Sharan Post-Graduate Student Department of Orthodontics &dentofacialorthopaedicsDayal SharanNo ratings yet
- Endodontic Orthodontic Relationships A Review of Integrated Treatment PlanningDocument18 pagesEndodontic Orthodontic Relationships A Review of Integrated Treatment PlanningAlfonso SernaNo ratings yet
- Systemic Diseases and Medications InfluenceDocument20 pagesSystemic Diseases and Medications InfluencealinagaxiolaariasNo ratings yet
- Article - 1459954778 2Document7 pagesArticle - 1459954778 2SOLEHANo ratings yet
- Management of Medically Compromised Prosthodontic PatientsDocument8 pagesManagement of Medically Compromised Prosthodontic PatientsIJAR JOURNALNo ratings yet
- SRMJResDentSci64261-1568441 042124Document4 pagesSRMJResDentSci64261-1568441 042124Dha Dina SevofrationNo ratings yet
- Accelerated OrthodonticsDocument1 pageAccelerated OrthodonticsAllen SharonNo ratings yet
- En Do Don Tic Orthodontic Relationship Are View of Treatment Planning ChangesDocument18 pagesEn Do Don Tic Orthodontic Relationship Are View of Treatment Planning ChangesSatpal SandhuNo ratings yet
- Accelerated OrthodonticsDocument7 pagesAccelerated OrthodonticsSneha JoshiNo ratings yet
- Regional Acceleratory Phenomenon A ReviewDocument4 pagesRegional Acceleratory Phenomenon A ReviewChzNo ratings yet
- Root Resorption in Maxillary & Mandiblar Anterior Segment During Active Orthodontic Treatment - A CBCT StudyDocument18 pagesRoot Resorption in Maxillary & Mandiblar Anterior Segment During Active Orthodontic Treatment - A CBCT StudyImpact JournalsNo ratings yet
- Orthodontic Considerations in The Evaluation and Treatment of Dentofacial DeformitiesDocument36 pagesOrthodontic Considerations in The Evaluation and Treatment of Dentofacial DeformitiesLaura Naiez NaiezNo ratings yet
- The Open Dentistry Journal: Methodologies in Orthodontic Pain Management: A ReviewDocument6 pagesThe Open Dentistry Journal: Methodologies in Orthodontic Pain Management: A Reviewnevin santhoshNo ratings yet
- The Action of Corticosteroids On Orthodontic Tooth MovementDocument25 pagesThe Action of Corticosteroids On Orthodontic Tooth MovementDhanusha ReddyNo ratings yet
- Effect of Splinting On Periodontal Health - A ReviewDocument4 pagesEffect of Splinting On Periodontal Health - A ReviewSweetz Viena ParamitaNo ratings yet
- MuhlemanDocument3 pagesMuhlemanAristya SidhartaNo ratings yet
- Ortho-Perio Relation: A Review: Deepthi PK, Arun Kumar P, Esther Nalini H, Renuka DeviDocument5 pagesOrtho-Perio Relation: A Review: Deepthi PK, Arun Kumar P, Esther Nalini H, Renuka DeviNeelash KrishnaNo ratings yet
- Orthodontic Tooth Movement After Inhibition of Cyclooxygenase-2Document5 pagesOrthodontic Tooth Movement After Inhibition of Cyclooxygenase-2Laís C. PoletoNo ratings yet
- Asds 07 1679Document4 pagesAsds 07 1679Abdulla Al-keklyNo ratings yet
- Root Resorption Abuabara 2007Document4 pagesRoot Resorption Abuabara 2007Aly OsmanNo ratings yet
- Literature Review of Quantitative StudiesDocument5 pagesLiterature Review of Quantitative Studiesd0vidihujam3100% (1)
- Kinjal AttachedDocument1 pageKinjal AttachedNilay JethavaNo ratings yet
- Writing Vstep Scan 1Document24 pagesWriting Vstep Scan 1NgaNo ratings yet
- NZ Physiotherapy Code of Ethics Final 0Document6 pagesNZ Physiotherapy Code of Ethics Final 0Pintilie MihaelaNo ratings yet
- Environmental Controls in Operating Theatres: S. Dharan and D. PittetDocument6 pagesEnvironmental Controls in Operating Theatres: S. Dharan and D. PittetDinda FSNo ratings yet
- Ingles Compresion LectoraDocument6 pagesIngles Compresion LectoraAlvaro Josue HernandezNo ratings yet
- Pbs Register of SponsorsDocument1,727 pagesPbs Register of SponsorsZaili KastamNo ratings yet
- Literature Review On Electronic Health RecordsDocument6 pagesLiterature Review On Electronic Health Recordsea2167ra100% (1)
- Daftar Obat Untuk Formularium KlinikDocument42 pagesDaftar Obat Untuk Formularium KlinikRianda LeeNo ratings yet
- Department of Education: Directions: Choose The Letter of The Correct AnswerDocument2 pagesDepartment of Education: Directions: Choose The Letter of The Correct AnswerMelitado WengNo ratings yet
- The Ladli Scheme in India ReportDocument26 pagesThe Ladli Scheme in India ReportManoj BhalaniNo ratings yet
- Digi T Vigilance TestDocument6 pagesDigi T Vigilance TestJillianne FrancoNo ratings yet
- EntDocument11 pagesEntkhuzaima9No ratings yet
- Full Length Research Article: ISSN: 2230-9926Document5 pagesFull Length Research Article: ISSN: 2230-9926Nisarg SutharNo ratings yet
- Tratament Diuretic in Insuficienta CardiacaDocument19 pagesTratament Diuretic in Insuficienta CardiacaOlga HMNo ratings yet
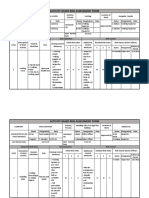
- Activity-Based Risk Assessment Form: Wearing InspectorDocument3 pagesActivity-Based Risk Assessment Form: Wearing InspectorSherly MagatNo ratings yet
- Case Study APFDocument64 pagesCase Study APFJayselle ArvieNo ratings yet
- Modele Anglais - Convention Coordonnateur - Version 20220409Document36 pagesModele Anglais - Convention Coordonnateur - Version 20220409SchmoutNo ratings yet
- From Sanity To Not Guilty by Reason of Insanity .The Legal FrameworkDocument18 pagesFrom Sanity To Not Guilty by Reason of Insanity .The Legal FrameworkPrecious OzigiNo ratings yet
- 12 - DEMONSTRATION INSTRUCTION FOR THE TRAINEE AND THE TRAINER Rev01Document2 pages12 - DEMONSTRATION INSTRUCTION FOR THE TRAINEE AND THE TRAINER Rev01Crisostomo MateoNo ratings yet
- NFPA 1700 - TrainingMaterialsDocument41 pagesNFPA 1700 - TrainingMaterialsGiovanni PalmieriNo ratings yet
- Angelina Hull Student - Heritagehs - Argumentative Essay - Student Name - Class Period - Spring 19 - H English 1Document5 pagesAngelina Hull Student - Heritagehs - Argumentative Essay - Student Name - Class Period - Spring 19 - H English 1api-461590822No ratings yet
- Tips On NURSING LICENSURE EXAM PDFDocument4 pagesTips On NURSING LICENSURE EXAM PDFCrystal Ann Monsale TadiamonNo ratings yet
- Reflection Paper MULANAYDocument2 pagesReflection Paper MULANAYRob40% (5)
- Paaralang Sekundarya NG Lucban Integrated School: Research CapsuleDocument10 pagesPaaralang Sekundarya NG Lucban Integrated School: Research CapsuleJohn Lester M. Dela CruzNo ratings yet
- (Comprehensive Geriatric Assessment) Experiencia Com Idosos de Colombia E BrasilDocument27 pages(Comprehensive Geriatric Assessment) Experiencia Com Idosos de Colombia E BrasilBrisa NarvaezNo ratings yet
- Say No To PlasticDocument28 pagesSay No To Plasticpavithra nirmalaNo ratings yet