You might also like
- SEP Sepsis Kills: Paediatric Blood Culture GuidelineDocument3 pagesSEP Sepsis Kills: Paediatric Blood Culture GuidelineEliana LopezNo ratings yet
- Adult Blood Culture Guideline Updated Sept2016Document3 pagesAdult Blood Culture Guideline Updated Sept2016Dima GheorgheNo ratings yet
- Blood Cultures in Newborns and Children: Optimising An Everyday TestDocument5 pagesBlood Cultures in Newborns and Children: Optimising An Everyday TestŜâifJämêêlNo ratings yet
- Review On Blood Culture: Anup R Warrier, Mathew ThomasDocument3 pagesReview On Blood Culture: Anup R Warrier, Mathew Thomaspurnima4uonlyNo ratings yet
- Pracactical Session of CVS ModuleDocument18 pagesPracactical Session of CVS Modulehatem newishyNo ratings yet
- Blood Culture Collection Policy Highlights Best PracticesDocument12 pagesBlood Culture Collection Policy Highlights Best Practicesyousrazeidan1979No ratings yet
- Role of Specimen CollectionDocument72 pagesRole of Specimen Collectiontummalapalli venkateswara rao100% (4)
- J. Clin. Microbiol. 2011 Weinstein S26 9Document4 pagesJ. Clin. Microbiol. 2011 Weinstein S26 9Prakarsa Adi Daya NusantaraNo ratings yet
- Celebrating 70 Years of the Hungarian Society of Laboratory MedicineDocument9 pagesCelebrating 70 Years of the Hungarian Society of Laboratory MedicineRiski Nur RamadhaniNo ratings yet
- Bacteremia - Blood Cultures and Other Diagnostic Tools - UpToDateDocument14 pagesBacteremia - Blood Cultures and Other Diagnostic Tools - UpToDateMarcelo Saavedra MontoyaNo ratings yet
- Blood Culture Test ExplainedDocument22 pagesBlood Culture Test ExplainedpawchanNo ratings yet
- Diagnosis of Fungemia in Immunosuppressed Patients Using Blood Culture TechniquesDocument25 pagesDiagnosis of Fungemia in Immunosuppressed Patients Using Blood Culture Techniquesማላያላም ማላያላምNo ratings yet
- Yield of Blood Cultures in Children Presenting With Febrile Illness in A Tertiary Care HospitalDocument5 pagesYield of Blood Cultures in Children Presenting With Febrile Illness in A Tertiary Care Hospitalfaraz.mirza1No ratings yet
- Instruction For Collection of Microbiology PDFDocument8 pagesInstruction For Collection of Microbiology PDFAbu KaramNo ratings yet
- Specimen Collection in Infectious DiseasesDocument72 pagesSpecimen Collection in Infectious DiseasesFadi KhaizaranNo ratings yet
- Bacteremia - Blood Cultures and Other Diagnostic Tools - UpToDateDocument15 pagesBacteremia - Blood Cultures and Other Diagnostic Tools - UpToDateJota MartinezNo ratings yet
- Providing guidance on blood transfusions in resource-limited settingsDocument7 pagesProviding guidance on blood transfusions in resource-limited settingsHany ElbarougyNo ratings yet
- Sample CollectionDocument20 pagesSample Collectionmaan khanNo ratings yet
- Pediatric VenipunctureDocument7 pagesPediatric VenipunctureJulius FrondaNo ratings yet
- Blood Culture Collection ProcedureDocument2 pagesBlood Culture Collection ProcedureNestor PlasabasNo ratings yet
- 1Document6 pages1Thái Đàm VănNo ratings yet
- PL-Microbiology Specimen Collection Guidelines (2020.07.22)Document14 pagesPL-Microbiology Specimen Collection Guidelines (2020.07.22)Anonymous fgRHAEIMrHNo ratings yet
- Discarding The Initial Aliquot of Blood Does Not Reduce Contamination Rates in Intravenous-Catheter-Drawn Blood CulturesDocument2 pagesDiscarding The Initial Aliquot of Blood Does Not Reduce Contamination Rates in Intravenous-Catheter-Drawn Blood CulturesKay HanNo ratings yet
- Blood Specimen Collection: Blood Cultures - Ce: AlertDocument21 pagesBlood Specimen Collection: Blood Cultures - Ce: AlertJuilta AstiwiNo ratings yet
- Specimen Collection 2Document70 pagesSpecimen Collection 2Sakura Di Musim Semi100% (1)
- Relevance of Routine Use of The Anaerobic Blood Culture BottleDocument5 pagesRelevance of Routine Use of The Anaerobic Blood Culture BottleSambit DashNo ratings yet
- Frequency of Thrombocytopenia in Neonatal Sepsis: Dr. Nadia GulDocument9 pagesFrequency of Thrombocytopenia in Neonatal Sepsis: Dr. Nadia GulNaeem NawazNo ratings yet
- Revisiting Blood CulturingDocument2 pagesRevisiting Blood Culturingtummalapalli venkateswara raoNo ratings yet
- Sepsis in The Newborn - Latest NewsDocument13 pagesSepsis in The Newborn - Latest NewsBrunaNo ratings yet
- 2022 Blood Culture Booklet Provided by BiomerieuxDocument19 pages2022 Blood Culture Booklet Provided by BiomerieuxAndy SetiawanNo ratings yet
- Laboratory Diagnosis of Bloodstream Infections: Mm. CajucomDocument23 pagesLaboratory Diagnosis of Bloodstream Infections: Mm. CajucomMarc CajucomNo ratings yet
- Blood CultureDocument38 pagesBlood CultureGlucose DRglucoseNo ratings yet
- 2 C PDFDocument14 pages2 C PDFAvisena AzisNo ratings yet
- Ciz 971Document6 pagesCiz 971Software InvestigaciónNo ratings yet
- Specimen Collection and ProcessingDocument18 pagesSpecimen Collection and ProcessingShopee PremiumismeNo ratings yet
- Guide to Neonatal Sepsis ScreeningDocument8 pagesGuide to Neonatal Sepsis ScreeningraniaulfahNo ratings yet
- Blood Culture: A Key Investigation FORDocument19 pagesBlood Culture: A Key Investigation FORJordan Alvarez Toro100% (1)
- Policies and Procedures of Laboratory Services in Each AreaDocument10 pagesPolicies and Procedures of Laboratory Services in Each AreaDarren CarinoNo ratings yet
- Predictors of Positive Blood Culture and Deaths Among Neonates With Suspected Neonatal Sepsis in A Tertiary Hospital, Mwanza-TanzaniaDocument9 pagesPredictors of Positive Blood Culture and Deaths Among Neonates With Suspected Neonatal Sepsis in A Tertiary Hospital, Mwanza-Tanzaniafasya azzahraNo ratings yet
- Pediatric Blood TransfusionDocument10 pagesPediatric Blood TransfusionELISION OFFICIALNo ratings yet
- 194 265 1 SMDocument5 pages194 265 1 SMAdkhiatul MuslihatinNo ratings yet
- Specimen Collection MicrobiologyDocument25 pagesSpecimen Collection MicrobiologyHartiniNo ratings yet
- Mycology SOP 2nd Ed 2019Document144 pagesMycology SOP 2nd Ed 2019Deepak Muralidhara NadigNo ratings yet
- Clinical MicrobiologyDocument91 pagesClinical MicrobiologyDr. Jayesh Patidar67% (3)
- Is The VolumeDocument5 pagesIs The VolumePaola NapoliNo ratings yet
- Lab TechniquesDocument5 pagesLab TechniquesElvisNo ratings yet
- Blood BankDocument22 pagesBlood BankArshNo ratings yet
- Assignment in Module 8 and 9 - AZURDocument3 pagesAssignment in Module 8 and 9 - AZURCARL AXEL AZURNo ratings yet
- Etiology of Neonatal Sepsis in Five Urban Hospitals in The PhilippinesDocument11 pagesEtiology of Neonatal Sepsis in Five Urban Hospitals in The PhilippinesAlexandra Duque-DavidNo ratings yet
- PMLS Lec 5 7 FinalsDocument13 pagesPMLS Lec 5 7 FinalsEthel JerricaNo ratings yet
- Cord Blood BankingDocument5 pagesCord Blood BankingRavi KantNo ratings yet
- Specimen Collection - MicrobiologyDocument14 pagesSpecimen Collection - MicrobiologyRahmiati LaoNo ratings yet
- Blood Culture Contamination: Single-Sample StrategyDocument8 pagesBlood Culture Contamination: Single-Sample StrategyArthur YanezNo ratings yet
- Booklet Blood Culture 2018Document19 pagesBooklet Blood Culture 2018Karmass JallalNo ratings yet
- Collection of Blood From DonorsDocument7 pagesCollection of Blood From DonorsBernardoHernandezNo ratings yet
- SepsisDocument9 pagesSepsisArief FidiantoNo ratings yet
- Diagnosing Viral Infections Lab TechniquesDocument18 pagesDiagnosing Viral Infections Lab TechniquesDragon Gie30No ratings yet
- Accurate and Fast Diagnostic Algorithm For Febrile UTIDocument7 pagesAccurate and Fast Diagnostic Algorithm For Febrile UTIManusama HasanNo ratings yet
- Unit 1 - 1.2 Techniques Oriented Examination of Specimens-Blood, CSF, Body Fluids, Pus and Aspirates, Throat Swab, StoolDocument47 pagesUnit 1 - 1.2 Techniques Oriented Examination of Specimens-Blood, CSF, Body Fluids, Pus and Aspirates, Throat Swab, StoolProvince Public Health Laboratory JanakpurNo ratings yet
- Adhesive DressingDocument10 pagesAdhesive DressingFatma ElzaytNo ratings yet
- APSNA PFIS GastrostomyTubeDocument4 pagesAPSNA PFIS GastrostomyTubeFatma ElzaytNo ratings yet
- Additional 14 and 5Document4 pagesAdditional 14 and 5Fatma ElzaytNo ratings yet
- Pediatric Nursing Knowledge & Skills ChecklistDocument4 pagesPediatric Nursing Knowledge & Skills Checklistnorthweststaffing67% (3)
- Emrpub 2012 en 1362 PDFDocument82 pagesEmrpub 2012 en 1362 PDFachysfNo ratings yet
- Pediatric Patient Safety and Quality Improvement by Karen Frush Steven E. KrugDocument334 pagesPediatric Patient Safety and Quality Improvement by Karen Frush Steven E. KrugFatma ElzaytNo ratings yet
- Randomized Trial of Alcohol Triple Dye For Umbilical Cord CareDocument5 pagesRandomized Trial of Alcohol Triple Dye For Umbilical Cord CareFatma ElzaytNo ratings yet
- Updates To Neonatal, Pediatric Resuscitation Guidelines Based On New EvidenceDocument3 pagesUpdates To Neonatal, Pediatric Resuscitation Guidelines Based On New EvidenceFatma ElzaytNo ratings yet
- Global Patient Safety Action Plan 2021-2030Document108 pagesGlobal Patient Safety Action Plan 2021-2030Leia MendesNo ratings yet
- Two Methods of Cord Care in High-Risk Newborns: Their Effects On Hydration, Temperature, PH, and Floras of The Cord AreaDocument12 pagesTwo Methods of Cord Care in High-Risk Newborns: Their Effects On Hydration, Temperature, PH, and Floras of The Cord AreaFatma ElzaytNo ratings yet
- National Paediatric Early Warning Score Chart TrainingDocument10 pagesNational Paediatric Early Warning Score Chart TrainingFatma ElzaytNo ratings yet
- 1 - First Lecture - Introduction & DataDocument6 pages1 - First Lecture - Introduction & DataFatma ElzaytNo ratings yet
- Neonates: Clinical Syndromes and Cardinal Fea-Tures of Infectious Diseases: Approach To Diagnosis and Initial ManagementDocument7 pagesNeonates: Clinical Syndromes and Cardinal Fea-Tures of Infectious Diseases: Approach To Diagnosis and Initial ManagementFatma ElzaytNo ratings yet
- Ubbilical Hernia Science DirectDocument14 pagesUbbilical Hernia Science DirectFatma ElzaytNo ratings yet
- Delayed Versus Immediate Cord Clamping in Preterm Infants: Original ArticleDocument11 pagesDelayed Versus Immediate Cord Clamping in Preterm Infants: Original ArticleFatma ElzaytNo ratings yet
- Borntoosoon Chapter5Document18 pagesBorntoosoon Chapter5Datulna Benito Mamaluba Jr.No ratings yet
- Chamnanvanakij, 2005Document6 pagesChamnanvanakij, 2005Fatma ElzaytNo ratings yet
- Bile Esculin Test MicroDocument2 pagesBile Esculin Test MicroFatma ElzaytNo ratings yet
- Factores Umbilical Cord InfectionDocument15 pagesFactores Umbilical Cord InfectionFatma ElzaytNo ratings yet
- Science Direct Cord CareDocument7 pagesScience Direct Cord CareFatma ElzaytNo ratings yet
- Umbilical Cord Care After The First Day From Birth: A Case Control Study in A Northeastern Italian HospitalDocument7 pagesUmbilical Cord Care After The First Day From Birth: A Case Control Study in A Northeastern Italian HospitalFatma ElzaytNo ratings yet
- Egypt 2014 Demographic and Health SurveyDocument463 pagesEgypt 2014 Demographic and Health SurveyFatma ElzaytNo ratings yet
- 2 Ref IntroductionDocument6 pages2 Ref IntroductionFatma ElzaytNo ratings yet
- Original Research Article: ISSN: 2230-9926Document7 pagesOriginal Research Article: ISSN: 2230-9926Fatma ElzaytNo ratings yet
- Lyngdoh 2018Document6 pagesLyngdoh 2018Fatma ElzaytNo ratings yet
- WHO Guidelines For Newborn CareDocument26 pagesWHO Guidelines For Newborn CareMamoni MaityNo ratings yet
- Nonate in Nicu Scince DirectDocument7 pagesNonate in Nicu Scince DirectFatma ElzaytNo ratings yet
- GentianaDocument7 pagesGentianaFatma ElzaytNo ratings yet
- New Born Skin Care GuidlineDocument1 pageNew Born Skin Care GuidlineFatma ElzaytNo ratings yet
- Ozdamire 2017organismesDocument7 pagesOzdamire 2017organismesFatma ElzaytNo ratings yet
- Bitterness Compounds in Coffee Brew Measured by Analytical Instruments and Taste Sensing SystemDocument34 pagesBitterness Compounds in Coffee Brew Measured by Analytical Instruments and Taste Sensing SystemSolisNo ratings yet
- Chapter 17Document48 pagesChapter 17MahmoudKhedrNo ratings yet
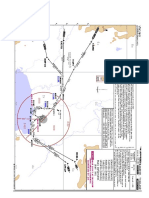
- VTBS 20-3DDocument1 pageVTBS 20-3Dwong keen faivNo ratings yet
- Man and Mystery Vol 13 - Monsters and Cryptids (Rev06)Document139 pagesMan and Mystery Vol 13 - Monsters and Cryptids (Rev06)Pablo Jr AgsaludNo ratings yet
- Power Grid Corporation of India Limited Construction ManagementDocument8 pagesPower Grid Corporation of India Limited Construction ManagementRahul RanjanNo ratings yet
- Seismic Design Coefficients and Factors TableDocument3 pagesSeismic Design Coefficients and Factors TableJonathan ColeNo ratings yet
- KSB ETN GM 80-200 - DomasDocument6 pagesKSB ETN GM 80-200 - Domasmuttawali arsyi han bugisNo ratings yet
- DTP - Digital Transformer ProtectionDocument13 pagesDTP - Digital Transformer ProtectionHBNBILNo ratings yet
- The Task of 5-Axis Milling PDFDocument4 pagesThe Task of 5-Axis Milling PDFManikanda PrabhucNo ratings yet
- Syngo MR E11 OncoDocument64 pagesSyngo MR E11 OncoLuís GuerraNo ratings yet
- Namma Kalvi 12th Maths Book Back 1 Mark Questions em 216251Document29 pagesNamma Kalvi 12th Maths Book Back 1 Mark Questions em 21625111B CHARAN ANANDNo ratings yet
- Mischel2004 - Toward An Integrative Science of The PersonDocument24 pagesMischel2004 - Toward An Integrative Science of The PersonTibor GalacziNo ratings yet
- The Emerald Tablets of Thoth Toth The Atlantean - Table 05Document5 pagesThe Emerald Tablets of Thoth Toth The Atlantean - Table 05Georgiana BealcuNo ratings yet
- Persian Polymath Physician Al-Rāzī's Life and WorksDocument10 pagesPersian Polymath Physician Al-Rāzī's Life and WorksAnonymous 29PN6AZTNo ratings yet
- NCE - Lesson 61 (A)Document8 pagesNCE - Lesson 61 (A)Zahir Pacasum-OmarNo ratings yet
- The Efficient Way To Prevent Water Carryover and Keep Your Indoor Air HealthierDocument1 pageThe Efficient Way To Prevent Water Carryover and Keep Your Indoor Air HealthierAzrinshah Abu BakarNo ratings yet
- Acute Pain - Mastectomy - Breast CADocument2 pagesAcute Pain - Mastectomy - Breast CAAngie MandeoyaNo ratings yet
- II PUC PHYSICS - Previously Appeared Questions and Answers For 2021 Exam by MANJUNATH BDocument52 pagesII PUC PHYSICS - Previously Appeared Questions and Answers For 2021 Exam by MANJUNATH BVishal Ramesh100% (1)
- IndictmentDocument2 pagesIndictmentCBS Austin WebteamNo ratings yet
- Literature ReviewDocument2 pagesLiterature ReviewFaith Arpon AbogandaNo ratings yet
- I PU Assignment 2023-24 For WorkshopDocument12 pagesI PU Assignment 2023-24 For Workshopfaruff111100% (1)
- Gujarat Technological University: W.E.F. AY 2018-19Document4 pagesGujarat Technological University: W.E.F. AY 2018-19Premal PatelNo ratings yet
- Incremental and Newton Methods Lab ReportDocument10 pagesIncremental and Newton Methods Lab ReportAbde RrahimNo ratings yet
- Sunningdale School Notes Summer 2022Document12 pagesSunningdale School Notes Summer 2022sunningdaleschoolNo ratings yet
- Fiat Type 199 Punto Evo 3 PDFDocument9 pagesFiat Type 199 Punto Evo 3 PDFGestione SportivaNo ratings yet
- DIESEL PARTS OF AMERICA DPA-240 USER'S MANUALDocument54 pagesDIESEL PARTS OF AMERICA DPA-240 USER'S MANUALEdinson Ariel Chavarro QuinteroNo ratings yet
- Phases of Clinical Trials: OverlapDocument3 pagesPhases of Clinical Trials: OverlapMohammed El-GezeiryNo ratings yet
- Modeling Endocrine Control of The Pituitary-Ovarian Axis: Androgenic Influence and Chaotic DynamicsDocument22 pagesModeling Endocrine Control of The Pituitary-Ovarian Axis: Androgenic Influence and Chaotic DynamicsKerin ArdyNo ratings yet
- Build A Borz Practical Scrap Metal Small Arms Vol9Document23 pagesBuild A Borz Practical Scrap Metal Small Arms Vol9Gia Linh Văn100% (2)
- Home Automation Chapter 1Document7 pagesHome Automation Chapter 1Nishant Sawant100% (1)