You might also like
- 2018 Update On OsteoporosisDocument16 pages2018 Update On OsteoporosisManel PopescuNo ratings yet
- Osteoporosis in Elderly MenDocument5 pagesOsteoporosis in Elderly MenFathia RachmatinaNo ratings yet
- Osteoporosis: How To Treat Osteoporosis: How To Prevent Osteoporosis: Along With Nutrition, Diet And Exercise For OsteoporosisFrom EverandOsteoporosis: How To Treat Osteoporosis: How To Prevent Osteoporosis: Along With Nutrition, Diet And Exercise For OsteoporosisNo ratings yet
- osteoprosis.pdfDocument6 pagesosteoprosis.pdfsaeed hasan saeedNo ratings yet
- Osteoporosis GTDocument15 pagesOsteoporosis GTZelalem AbrhamNo ratings yet
- Osteoporosis: Screening, Prevention, and ManagementDocument20 pagesOsteoporosis: Screening, Prevention, and ManagementBernardo RomeroNo ratings yet
- Pharmacists Lead Osteoporosis TreatmentDocument15 pagesPharmacists Lead Osteoporosis TreatmentJudith GraalNo ratings yet
- BMUS Chpt5 OsteoporosisDocument25 pagesBMUS Chpt5 OsteoporosisDaniel ChristoNo ratings yet
- Regaining Ground in Osteoporosis: Pharmacists Leading The ChargeDocument15 pagesRegaining Ground in Osteoporosis: Pharmacists Leading The ChargeJudith GraalNo ratings yet
- Group 5 OsteoporosisDocument17 pagesGroup 5 OsteoporosisFranchezka BeltranNo ratings yet
- Osteoporosis: Prepared By: Md. Giash Uddin Lecturer, Dept. of Pharmacy University of ChittagongDocument30 pagesOsteoporosis: Prepared By: Md. Giash Uddin Lecturer, Dept. of Pharmacy University of Chittagongsamiul bashirNo ratings yet
- Mpu3313 - v2 Mohamad Shafik Bin Supaat 821022145381001Document12 pagesMpu3313 - v2 Mohamad Shafik Bin Supaat 821022145381001محمد شافق ابنو شافعتNo ratings yet
- Orthopedic May 2013Document11 pagesOrthopedic May 2013javi222222No ratings yet
- Osteoporosis: The Increasing Role of The Orthopaedist: ClassificationDocument10 pagesOsteoporosis: The Increasing Role of The Orthopaedist: ClassificationMila RevalinaNo ratings yet
- What Is Osteoporosis?: Osteoposis Is A Disease ofDocument48 pagesWhat Is Osteoporosis?: Osteoposis Is A Disease ofTaruna GargNo ratings yet
- Osteoporosis PaperDocument7 pagesOsteoporosis Paperapi-558387899No ratings yet
- OsteoporosisDocument1 pageOsteoporosisaa4518379No ratings yet
- Osteo RXDocument27 pagesOsteo RXHarun NasutionNo ratings yet
- Mayo Clinic Guide to Preventing & Treating Osteoporosis: Keeping Your Bones Healthy and Strong to Reduce Your Risk of FractureFrom EverandMayo Clinic Guide to Preventing & Treating Osteoporosis: Keeping Your Bones Healthy and Strong to Reduce Your Risk of FractureRating: 2 out of 5 stars2/5 (1)
- Blok 16 Endocrinology of OsteoporosisDocument14 pagesBlok 16 Endocrinology of OsteoporosisHasty WahyuniNo ratings yet
- Paget Disease of Bone, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandPaget Disease of Bone, A Simple Guide to the Condition, Treatment and Related DiseasesNo ratings yet
- Patogenesis Osteoporosis VDocument15 pagesPatogenesis Osteoporosis Vaji pangestuNo ratings yet
- Patogenesis Osteoporosis V PDFDocument15 pagesPatogenesis Osteoporosis V PDFaji pangestuNo ratings yet
- Osteoporosis Case ReportDocument21 pagesOsteoporosis Case ReportJewenson SalvadorNo ratings yet
- Diet and Men 'S Sexual Health: Rates of Male Sexual DysfunctionsDocument15 pagesDiet and Men 'S Sexual Health: Rates of Male Sexual DysfunctionsHoa VânNo ratings yet
- Malnutrition in the ElderlyFrom EverandMalnutrition in the ElderlyW.O. SeilerNo ratings yet
- Hepatic Osteodystrophy MechanismDocument14 pagesHepatic Osteodystrophy MechanismM.miracleNo ratings yet
- OsteopeniaDocument9 pagesOsteopeniaMohamed EssallaaNo ratings yet
- Protocolo Clínico e Diretrizes Terapêuticas para Osteoporose no BrasilDocument22 pagesProtocolo Clínico e Diretrizes Terapêuticas para Osteoporose no BrasilDaniNo ratings yet
- Screening For Osteoporosis: Clinical PracticeDocument8 pagesScreening For Osteoporosis: Clinical PracticeGayuh PrastyaNo ratings yet
- Drug Induced OsteoporosisDocument22 pagesDrug Induced OsteoporosisGabriel JoséNo ratings yet
- Osteoporosis: Prevention and ManagementDocument36 pagesOsteoporosis: Prevention and Managementsara M.H.No ratings yet
- Osteoporosis Risk and Treatment ReviewDocument10 pagesOsteoporosis Risk and Treatment ReviewSandra Arely Rodriguez EscobarNo ratings yet
- Osteoporosis: Signs and SymptomsDocument9 pagesOsteoporosis: Signs and SymptomschelseachoirNo ratings yet
- Musculo-Skeletal Disorders - GoutDocument14 pagesMusculo-Skeletal Disorders - GoutKyle J. NortonNo ratings yet
- Life Extension Magazine: The 10 Most Important Blood TestsDocument6 pagesLife Extension Magazine: The 10 Most Important Blood TestsJaffer AftabNo ratings yet
- OsteoporosisDocument6 pagesOsteoporosiskingNo ratings yet
- OsteoporosisDocument6 pagesOsteoporosiskingNo ratings yet
- OsteoporosisDocument6 pagesOsteoporosiskingNo ratings yet
- OsteoporosisDocument6 pagesOsteoporosiskingNo ratings yet
- Osteoarthritis - (Arthrose in Europe) how to Prevent and Treat This Disease AccordinglyFrom EverandOsteoarthritis - (Arthrose in Europe) how to Prevent and Treat This Disease AccordinglyNo ratings yet
- Common Medications That Increase Calcium Loss and Promote Risk of OsteoporosisDocument1 pageCommon Medications That Increase Calcium Loss and Promote Risk of OsteoporosisAnonymous 4j7k1q9HNo ratings yet
- Novartis Osteoporosis Slide KitDocument42 pagesNovartis Osteoporosis Slide KitShravanti SatyanandNo ratings yet
- American Medical Women's Association Position Paper On OsteoporosisDocument7 pagesAmerican Medical Women's Association Position Paper On OsteoporosisVincent NandoNo ratings yet
- OsteoporosisDocument43 pagesOsteoporosisMuna Hassan Mustafa100% (1)
- Treatment of Low Bone Density or Osteoporosis To Prevent Fractures in Men and Women: A Clinical Practice Guideline Update From The American College of PhysiciansDocument28 pagesTreatment of Low Bone Density or Osteoporosis To Prevent Fractures in Men and Women: A Clinical Practice Guideline Update From The American College of PhysiciansRoberto López MataNo ratings yet
- Health and Wellness Promotion For Older AdultsDocument29 pagesHealth and Wellness Promotion For Older AdultsShimmering MoonNo ratings yet
- Piis2050052117300744 PDFDocument15 pagesPiis2050052117300744 PDFRichu UhcirNo ratings yet
- OsteoporosisDocument12 pagesOsteoporosisMahnoor ShahNo ratings yet
- Men OsteoporosisDocument5 pagesMen Osteoporosisapi-309082881No ratings yet
- Osteoporosis and OsteopeniaDocument29 pagesOsteoporosis and OsteopeniaShruti Maroo - RathiNo ratings yet
- 23andme Printable Report Aug 2013 RevisionDocument24 pages23andme Printable Report Aug 2013 RevisionLucien Engelen100% (1)
- OsteoporosisDocument12 pagesOsteoporosisAzharul Islam ArjuNo ratings yet
- Web AssignmentDocument1 pageWeb AssignmentJA BerzabalNo ratings yet
- OsteoporosisDocument6 pagesOsteoporosisabdulghaffarsp8No ratings yet
- Osteoporosis PDFDocument4 pagesOsteoporosis PDFmawarNo ratings yet
- Skeletal System Diseases and DisordersDocument32 pagesSkeletal System Diseases and DisordersPatrisha Georgia AmitenNo ratings yet
- Latihan Soal Bahasa InggrisDocument2 pagesLatihan Soal Bahasa Inggriscilacapbarat999No ratings yet
- SWINE Magazine Feb/Apr 2021Document30 pagesSWINE Magazine Feb/Apr 2021jem ruizNo ratings yet
- Catalogo Accesorios MINDRAYDocument64 pagesCatalogo Accesorios MINDRAYitalo100% (2)
- Vacuna Moderna Updated CDC September 11, 2023 Clinical Review - SPIKEVAXDocument156 pagesVacuna Moderna Updated CDC September 11, 2023 Clinical Review - SPIKEVAX9jz5dzj5gwNo ratings yet
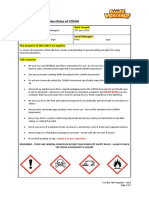
- 10 Golden COSHH RulesDocument2 pages10 Golden COSHH RulesKecskeméty BoriNo ratings yet
- Manpower Planning Hospital Ex 648Document3 pagesManpower Planning Hospital Ex 648supriyaverma1989No ratings yet
- CT1, CT2, CT5 and CT8 Study Plan UK Exams September 2013Document8 pagesCT1, CT2, CT5 and CT8 Study Plan UK Exams September 2013Mohamed ArafaNo ratings yet
- HerpesDocument2 pagesHerpesMaria Chacón CarbajalNo ratings yet
- Haryana Review MARCH 2017Document60 pagesHaryana Review MARCH 2017Neeraj YadavNo ratings yet
- LESSON PLAN FOR BASIC B.Sc. NURSING I YEAR PSYCHOLOGY SUBJECTDocument5 pagesLESSON PLAN FOR BASIC B.Sc. NURSING I YEAR PSYCHOLOGY SUBJECTVenkatesan AnnamalaiNo ratings yet
- Vial of BlissDocument2 pagesVial of BlissGuilherme De FariasNo ratings yet
- DCHDocument163 pagesDCHLuiza Radulescu100% (1)
- The End of Poverty - Jaffrey SachsDocument32 pagesThe End of Poverty - Jaffrey SachsPulkit GargNo ratings yet
- Notice 503943616Document2 pagesNotice 503943616abreu2021No ratings yet
- Chapter 2 General Conditions of ServiceDocument7 pagesChapter 2 General Conditions of ServiceAnand KrishnaNo ratings yet
- Comparison of The Recovery Rate of Otomycosis Using Betadine and Clotrimazole Topical TreatmentDocument6 pagesComparison of The Recovery Rate of Otomycosis Using Betadine and Clotrimazole Topical TreatmentHendra SusantoNo ratings yet
- Nur1 230 Fundamentals of Canadian NursingDocument1,666 pagesNur1 230 Fundamentals of Canadian NursingSamantha Lau100% (4)
- Massage techniques for relaxation and healingDocument1 pageMassage techniques for relaxation and healingALISA SAITANo ratings yet
- Chocolate and DepressionDocument15 pagesChocolate and DepressionAdriantopNo ratings yet
- Food Hygiene AssignmentDocument13 pagesFood Hygiene AssignmentSamjhana Neupane100% (1)
- Final MHA Thesis, Getachew L.Document62 pagesFinal MHA Thesis, Getachew L.Ochom Yar RiamNo ratings yet
- PhD Thesis AcknowledgementDocument3 pagesPhD Thesis AcknowledgementNeelamegam DevarasuNo ratings yet
- Brochogenic Cyst 2017.fullDocument5 pagesBrochogenic Cyst 2017.fullManok KumarNo ratings yet
- Solid Waste Management Policy Framework: Gaps and IssuesDocument20 pagesSolid Waste Management Policy Framework: Gaps and IssuesThe Outer Marker100% (5)
- BMCH Family Planning Policy Provides Universal AccessDocument2 pagesBMCH Family Planning Policy Provides Universal AccessShang Dimol100% (1)
- Cataingan East District SBFP ReportDocument24 pagesCataingan East District SBFP ReportCarlota TejeroNo ratings yet
- Summative 2 Form 2 November K2Document4 pagesSummative 2 Form 2 November K2Sha MinNo ratings yet
- Applied Kinesiology Collected Papers 2001-2006Document124 pagesApplied Kinesiology Collected Papers 2001-2006Huib Salomons80% (10)
- Forensic PathologyDocument3 pagesForensic PathologyjmosserNo ratings yet
- Antibody Conjugate ProtacDocument7 pagesAntibody Conjugate Protac김현수No ratings yet