Volume 9, Issue 2, February – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
A Giant Obstructing Prostatic Urethral Calculi –
A Rare Case Report
1 2
Usha Topalkatti Arun Rathi
Internal Medicine, Spartan Health Science University MBBS, MS MCH Genitourinary Surgery ,
School of Medicine, Vieux Fort, Saint Lucia Chalmeda Anand Rao Institute of Medical Sciences,
Hyderabad, India
3 4
Adeeb Afsar. Param Kadam
Mediciti Institute of Medical Sciences, Hyderabad, India MIMER Medical College , Maharashtra, India
Abstract:- Giant obstructing prostatic urethral calculi Patient was treated by suprapubic transvesical
are a rare but significant entity within the spectrum of cystolithotomy(fig 4) and bladder neck incision was given to
lower urinary tract lithiasis. Representing a minute retrieve the giant prostatic urethral calculi.
fraction of urinary stone disease cases, these calculi pose
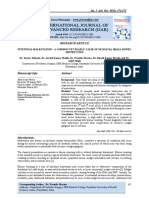
unique diagnostic and management challenges. This X-ray KUB(fig 1) and NCCT KUB( fig 2)
comprehensive review synthesizes existing literature to
provide insights into the epidemiology, etiology, clinical Ncct Kub revealed B/L Renal calculi with
presentation, diagnostic modalities, and treatment hydroureteronephrosis,Two vesical calculi of size 2.5cm, A
options for giant obstructing prostatic urethral calculi. large prostatic Urethral Calculus of size 5 x 3.3 cm and
We explore the bimodal age distribution of incidence, cystitis
highlighting peaks in early childhood and the fourth
decade of life, and delve into potential etiological factors Cystoscopy (fig 3) finding was suggestive of a giant
including migration from the bladder or upper urinary obstructing prostatic urethral calculi in dilated prostatic
tracts and de novo formation. Clinical manifestations urethra.
vary, ranging from acute lower urinary tract symptoms
to more insidious presentations associated with
anatomical abnormalities. Diagnostic strategies,
encompassing imaging modalities and laboratory tests,
are crucial for accurate assessment and management
planning. Treatment approaches, such as endoscopic
lithotripsy, open surgical procedures, and shock wave
lithotripsy, are discussed in detail, along with their
respective success rates and complications. Through a
thorough examination of the current source , this case
report aims to enhance understanding and facilitate
optimal management strategies for giant obstructing
prostatic urethral calculi. Fig 1 - vesical calculi and prostatic urethral calculi
Keywords:- Giant Urethral Calculi, Management Strategies
, Lower Urinary Tract Lithiasis, Prostatic Urethral Calculi.
I. INTRODUCTION
A 74 yr old male came to the emergency department
with abdominal pain and lower urinary tract symptoms. On
physical examination presence of suprapubic fullness and
tenderness. X-ray Kub (Kidneys, ureter, bladder) revealed
vesical calculi and prostatic urethral calculi (fig 1). Non-
Contrast Computerized Tomography Scan of the kidneys,
ureter, and bladder (NCCT kub). (fig 2) revealed Bilateral
(B/L) renal calculi with bilateral hydroureteronephrosis, two
vesical calculi each 2.5cm and a large Prostatic urethral
calculus of size 5 x 3.3cm. Urine examination was Fig 2- B/L renal calculi with bilateral
suggestive of Urinary tract infection (UTI). Cystoscopy(fig hydroureteronephrosis ,vesical calculi, giant prostatic
3) revealed completely obstructing giant prostatic urethral urethral calculi
calculi.
IJISRT24FEB346 www.ijisrt.com 842
Volume 9, Issue 2, February – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
onset symptoms. Diagnosis frequently involves the
identification of urinary tract infections at the time of
presentation [3]. For stones situated in the posterior urethra,
they can be displaced back into the bladder for subsequent
fragmentation through methods like electro hydraulic or
laser lithotripsy, with reported success rates ranging from
66% to 86%. If fragmentation within the bladder proves
unsuccessful, open cystolithotomy may be necessary.
Although shock wave lithotripsy after displacement into the
bladder has been attempted, success rates have been
reported at only 60% [4].
Fig 3 - completely obstructing giant prostatic urethral calculi
REFERENCES
[1]. Aegukkatajit S. Reduction of urinary stone in children
from north-eastern Thailand. J Med Assoc Thai
1999;82:1230–3.
[2]. Kamal BA, Anikwe RM, Darawani H, et al. Urethral
calculi: presentation and management. BJU Int
2004;93:549–52.
[3]. Shanmugam TV, Dhanapal V, Rajaraman T, et al.
Giant urethral calculi. Hosp Med 2000;61:582.
[4]. El-Sharif AE, Prasad K. Treatment of urethral stones
by retrograde manipulation and extracorporeal shock
wave lithotripsy. Br J Urol 1995;76: 761–4.
Fig 4 -suprapubic transvesical cystolithotomy
Fig 5- calculi
II. DISCUSSION
Urethral calculi represent a rare occurrence within
lower urinary tract lithiasis, constituting merely (0.3%) of
all instances of urinary stone disease in endemic areas [1].
These calculi typically manifest with a bimodal age
distribution, with peak occurrences observed in early
childhood and the fourth decade of life. They can originate
from migration from the bladder or upper urinary tracts or
form spontaneously, often in conjunction with anatomical
anomalies like strictures or diverticula, or from deposition
on a foreign body. Research indicates that only a small
proportion (2%) of patients with migratory urethral calculi
also have concurrent bladder stones, while a larger fraction
(18%) exhibit coexisting upper urinary tract calculus
disease[2]. Symptoms vary depending on the calculus type;
migratory calculi often precipitate acute lower urinary tract
symptoms, such as stranguria, urinary retention, gross
hematuria, and dysuria, while de novo urethral calculi and
those situated in diverticula may present with more gradual
IJISRT24FEB346 www.ijisrt.com 843
You might also like
- URL in A Case of AdultNeglected Case of Bladder ExstrophyDocument2 pagesURL in A Case of AdultNeglected Case of Bladder ExstrophyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Surgical Management of Urolithiasis in Dog Along With Peritoneal Dialysis: 12 CasesDocument10 pagesSurgical Management of Urolithiasis in Dog Along With Peritoneal Dialysis: 12 CasesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Rajiv Gandhi University of Health Sciences: Proforma For Registration of Subject For DissertationDocument25 pagesRajiv Gandhi University of Health Sciences: Proforma For Registration of Subject For DissertationShivu ShivukumarNo ratings yet
- Diagnosis of Urethral Stricture On Dynamic Voiding Transvaginal Sonourethrography: A Case ReportDocument4 pagesDiagnosis of Urethral Stricture On Dynamic Voiding Transvaginal Sonourethrography: A Case ReportSri PertiwiNo ratings yet
- Articles: BackgroundDocument8 pagesArticles: Backgroundapi-62836649No ratings yet
- International Journal of Surgery Case ReportsDocument6 pagesInternational Journal of Surgery Case ReportsErikNo ratings yet
- Dual Loop Reconstruction After Pancreaticoduodenectomy For A Previous Roux-En-Y Biliodigestive Anastomosis A Case ReportDocument2 pagesDual Loop Reconstruction After Pancreaticoduodenectomy For A Previous Roux-En-Y Biliodigestive Anastomosis A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Scholars Journal of Medical Case Reports: ISSN 2347-6559 (Online) ISSN 2347-9507 (Print)Document2 pagesScholars Journal of Medical Case Reports: ISSN 2347-6559 (Online) ISSN 2347-9507 (Print)galihmuchlishermawanNo ratings yet
- Anest Caudal UsgDocument3 pagesAnest Caudal UsgEva Garcia MartinezNo ratings yet
- Glandular Cystitis - A Rare Benign Condition Presenting As A Pseudo-Tumor of The BladderDocument3 pagesGlandular Cystitis - A Rare Benign Condition Presenting As A Pseudo-Tumor of The BladderRahmamagerNo ratings yet
- Intestinal Malrotation - A Common Yet Deadly Cause of Neonatal Small Bowel ObstructionDocument4 pagesIntestinal Malrotation - A Common Yet Deadly Cause of Neonatal Small Bowel ObstructionIJAR JOURNALNo ratings yet
- Bladder Decompression For Chronic Urinary Retention May Lead To Upper Tract BleedingDocument3 pagesBladder Decompression For Chronic Urinary Retention May Lead To Upper Tract BleedingRara Aulia IINo ratings yet
- International Ayurvedic Medical Journal: Case Report ISSN: 2320 5091 Impact Factor: 4.018Document5 pagesInternational Ayurvedic Medical Journal: Case Report ISSN: 2320 5091 Impact Factor: 4.018Sonu JangraNo ratings yet
- Stricture Urethra in Children: An Indian Perspective: Original ArticleDocument6 pagesStricture Urethra in Children: An Indian Perspective: Original ArticleLilis Endah SulistiyawatiNo ratings yet
- Pi Is 2468448120302800Document2 pagesPi Is 2468448120302800Shivaraj S ANo ratings yet
- Dusting Versus Basketing During UreterosDocument5 pagesDusting Versus Basketing During UreterosCarlos Esteban Gutiérrez CastrejonNo ratings yet
- El Khoury2018Document3 pagesEl Khoury2018peroksidaseNo ratings yet
- A Case Report of Ancient Presacral SchwannomaDocument4 pagesA Case Report of Ancient Presacral SchwannomaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Treatment of Giant Prostatic Urethral Stone W 2024 International Journal ofDocument5 pagesTreatment of Giant Prostatic Urethral Stone W 2024 International Journal ofRonald QuezadaNo ratings yet
- Cong Cyst Pancreas DR Nitin JainDocument5 pagesCong Cyst Pancreas DR Nitin JainMohsin SaeedNo ratings yet
- Management of Urethral Stricture by UttarabastiDocument4 pagesManagement of Urethral Stricture by Uttarabastimurshid AhmedNo ratings yet
- Parameatal Cyst :A Case ReportDocument3 pagesParameatal Cyst :A Case ReportDr.ankit AnandNo ratings yet
- Factors Contributing To SMALL INTESTINE Suture Line Disruption PDFDocument117 pagesFactors Contributing To SMALL INTESTINE Suture Line Disruption PDFDumitru RadulescuNo ratings yet
- Diagnosis and Surgical Management of Prostatic Abscess in A DogDocument4 pagesDiagnosis and Surgical Management of Prostatic Abscess in A DogPutri Nadia ReskiNo ratings yet
- Cats With Circumcaval UretersDocument8 pagesCats With Circumcaval UretersDaniel CapuchoNo ratings yet
- Advancements in Upper Gastrointestinal Endoscopic Therapy: A Comprehensive ReviewDocument12 pagesAdvancements in Upper Gastrointestinal Endoscopic Therapy: A Comprehensive ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Extracorporeal Shock Wave Lithotripsy and Endoscopic Ureteral Stent Placement in An Asian Small-Clawed Otter (Aonyx Cinerea) With NephrolithiasisDocument6 pagesExtracorporeal Shock Wave Lithotripsy and Endoscopic Ureteral Stent Placement in An Asian Small-Clawed Otter (Aonyx Cinerea) With NephrolithiasisツコロクムワNo ratings yet
- 2017 Cecal Dilatationand Distentionandits Managementinacowand Kankayam BullockDocument4 pages2017 Cecal Dilatationand Distentionandits Managementinacowand Kankayam BullockDrAmit KajalaNo ratings yet
- A Prospective Observational Study On Scola For Ventral Hernia With Diastasis Recti - Our Experience at A Tertiary Care HospitalDocument4 pagesA Prospective Observational Study On Scola For Ventral Hernia With Diastasis Recti - Our Experience at A Tertiary Care HospitalInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Infected Meckels Diverticulum Masquerading As Spontaneous Rupture of Umbilical Granuloma - A Case Report in One Month Old InfantDocument4 pagesInfected Meckels Diverticulum Masquerading As Spontaneous Rupture of Umbilical Granuloma - A Case Report in One Month Old InfantIJAR JOURNALNo ratings yet
- Abses Adalah 1332 5211 1 PBDocument5 pagesAbses Adalah 1332 5211 1 PBSayhelloTVNo ratings yet
- Adenocarcinoma Article 2021Document7 pagesAdenocarcinoma Article 2021Bapai MallikNo ratings yet
- Kodikara 2020Document3 pagesKodikara 2020Budi do Re miNo ratings yet
- Cystolithotomy Case Study From CJC-BSNDocument41 pagesCystolithotomy Case Study From CJC-BSNNil GyiNo ratings yet
- Mechanisms, Mitigation, and Management of Urinary Toxicity From Prostate RadiotherapyDocument10 pagesMechanisms, Mitigation, and Management of Urinary Toxicity From Prostate RadiotherapyZuriNo ratings yet
- Vesical Imaging Reporting and Data System (VI-RADS)Document2 pagesVesical Imaging Reporting and Data System (VI-RADS)medicoscantareiraNo ratings yet
- Case 1 Case 2: Bladder Outlet ObstructionDocument2 pagesCase 1 Case 2: Bladder Outlet ObstructionHardiTariqHamma100% (1)
- 1 s2.0 S1879522615003929 MainDocument4 pages1 s2.0 S1879522615003929 MainsagaNo ratings yet
- The Abcs of Voiding Cystourethrography: Pictorial EssayDocument18 pagesThe Abcs of Voiding Cystourethrography: Pictorial EssayDaniel Mamani CruzNo ratings yet
- Alexandria Journal of Medicine: Rehab Abdel Rahman El BakryDocument5 pagesAlexandria Journal of Medicine: Rehab Abdel Rahman El BakrySatrio Budi WicaksonoNo ratings yet
- Uti 11 30Document6 pagesUti 11 30Luis Ferdinand Dacera-Gabronino Gamponia-NonanNo ratings yet
- Uti 11 30 PDFDocument6 pagesUti 11 30 PDFLuis Ferdinand Dacera-Gabronino Gamponia-NonanNo ratings yet
- ANewalgorith JPUReprintDocument9 pagesANewalgorith JPUReprintAdam DarmawanNo ratings yet
- Journal of Pediatric Surgery: Shabnam Sabetkish, Nastaran Sabetkish, Abdol-Mohammad KajbafzadehDocument7 pagesJournal of Pediatric Surgery: Shabnam Sabetkish, Nastaran Sabetkish, Abdol-Mohammad KajbafzadehAmatystNo ratings yet
- Intervention Technologies at Treatment of Iatrogenic Strictures of Extrahepatic Bile DuctsDocument6 pagesIntervention Technologies at Treatment of Iatrogenic Strictures of Extrahepatic Bile DuctsCentral Asian StudiesNo ratings yet
- Large Renal Calculus Hidinga Renal Tumor Type Squamous Cell Carcinoma About A Rare Case and Review of LiteratureDocument5 pagesLarge Renal Calculus Hidinga Renal Tumor Type Squamous Cell Carcinoma About A Rare Case and Review of LiteratureIJAR JOURNALNo ratings yet
- Crim Urology2013-932529Document3 pagesCrim Urology2013-932529TheQueensafa90No ratings yet
- Jugular Vascular Access Port ImplantatioDocument6 pagesJugular Vascular Access Port ImplantatioputuNo ratings yet
- Congenital Anomalies of Kidney and Ureter 2161 0940 1000190Document10 pagesCongenital Anomalies of Kidney and Ureter 2161 0940 1000190Indra JayaNo ratings yet
- Practical Approach To Linear Endoscopic Ultrasound Examination of The Rectum and Anal CanalDocument10 pagesPractical Approach To Linear Endoscopic Ultrasound Examination of The Rectum and Anal CanalERICSON ARCANANo ratings yet
- The Characteristic Ultrasound Features of Specific Types of Ovarian Pathology (Review)Document15 pagesThe Characteristic Ultrasound Features of Specific Types of Ovarian Pathology (Review)Sam K. AikinsNo ratings yet
- 32CVIR300ABSEDocument8 pages32CVIR300ABSEResidencia Cirugia GeneralNo ratings yet
- Possibilities of Computed Tomography and Magnetic Resonance Urography As Modern Techniques in The Diagnosis of Volumetric Ureteral ProcessesDocument6 pagesPossibilities of Computed Tomography and Magnetic Resonance Urography As Modern Techniques in The Diagnosis of Volumetric Ureteral ProcessesCentral Asian StudiesNo ratings yet
- SC 20141Document3 pagesSC 20141RelviGuzmanApazaNo ratings yet
- Uterine RuptureDocument3 pagesUterine RuptureAndreaAlexandraNo ratings yet
- The Forgotten Stentolith A Rare Case ReportDocument3 pagesThe Forgotten Stentolith A Rare Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 44 Danfulani EtalDocument3 pages44 Danfulani EtaleditorijmrhsNo ratings yet
- 1 s2.0 S1930043321006816 MainDocument5 pages1 s2.0 S1930043321006816 MainFatimah AssagafNo ratings yet
- Urinary Bladder Diverticulum and Its Association With Malignancy: An Anatomical Study On CadaversDocument3 pagesUrinary Bladder Diverticulum and Its Association With Malignancy: An Anatomical Study On CadaversIrma Suriani DarwisNo ratings yet
- Sustainable Energy Consumption Analysis through Data Driven InsightsDocument16 pagesSustainable Energy Consumption Analysis through Data Driven InsightsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Vertical Farming System Based on IoTDocument6 pagesVertical Farming System Based on IoTInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Entrepreneurial Creative Thinking and Venture Performance: Reviewing the Influence of Psychomotor Education on the Profitability of Small and Medium Scale Firms in Port Harcourt MetropolisDocument10 pagesEntrepreneurial Creative Thinking and Venture Performance: Reviewing the Influence of Psychomotor Education on the Profitability of Small and Medium Scale Firms in Port Harcourt MetropolisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Influence of Principals’ Promotion of Professional Development of Teachers on Learners’ Academic Performance in Kenya Certificate of Secondary Education in Kisii County, KenyaDocument13 pagesInfluence of Principals’ Promotion of Professional Development of Teachers on Learners’ Academic Performance in Kenya Certificate of Secondary Education in Kisii County, KenyaInternational Journal of Innovative Science and Research Technology100% (1)
- Ambulance Booking SystemDocument7 pagesAmbulance Booking SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Utilization of Waste Heat Emitted by the KilnDocument2 pagesUtilization of Waste Heat Emitted by the KilnInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Digital Finance-Fintech and it’s Impact on Financial Inclusion in IndiaDocument10 pagesDigital Finance-Fintech and it’s Impact on Financial Inclusion in IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Detection and Counting of Fake Currency & Genuine Currency Using Image ProcessingDocument6 pagesDetection and Counting of Fake Currency & Genuine Currency Using Image ProcessingInternational Journal of Innovative Science and Research Technology100% (9)
- An Overview of Lung CancerDocument6 pagesAn Overview of Lung CancerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Osho Dynamic Meditation; Improved Stress Reduction in Farmer Determine by using Serum Cortisol and EEG (A Qualitative Study Review)Document8 pagesOsho Dynamic Meditation; Improved Stress Reduction in Farmer Determine by using Serum Cortisol and EEG (A Qualitative Study Review)International Journal of Innovative Science and Research TechnologyNo ratings yet
- An Efficient Cloud-Powered Bidding MarketplaceDocument5 pagesAn Efficient Cloud-Powered Bidding MarketplaceInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Designing Cost-Effective SMS based Irrigation System using GSM ModuleDocument8 pagesDesigning Cost-Effective SMS based Irrigation System using GSM ModuleInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Impact of Stress and Emotional Reactions due to the Covid-19 Pandemic in IndiaDocument6 pagesImpact of Stress and Emotional Reactions due to the Covid-19 Pandemic in IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Effect of Solid Waste Management on Socio-Economic Development of Urban Area: A Case of Kicukiro DistrictDocument13 pagesEffect of Solid Waste Management on Socio-Economic Development of Urban Area: A Case of Kicukiro DistrictInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Computer Vision Gestures Recognition System Using Centralized Cloud ServerDocument9 pagesComputer Vision Gestures Recognition System Using Centralized Cloud ServerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Auto Tix: Automated Bus Ticket SolutionDocument5 pagesAuto Tix: Automated Bus Ticket SolutionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Examining the Benefits and Drawbacks of the Sand Dam Construction in Cadadley RiverbedDocument8 pagesExamining the Benefits and Drawbacks of the Sand Dam Construction in Cadadley RiverbedInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Industry That Capitalizes Off of Women's Insecurities?Document8 pagesAn Industry That Capitalizes Off of Women's Insecurities?International Journal of Innovative Science and Research TechnologyNo ratings yet
- Forensic Advantages and Disadvantages of Raman Spectroscopy Methods in Various Banknotes Analysis and The Observed Discordant ResultsDocument12 pagesForensic Advantages and Disadvantages of Raman Spectroscopy Methods in Various Banknotes Analysis and The Observed Discordant ResultsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Predictive Analytics for Motorcycle Theft Detection and RecoveryDocument5 pagesPredictive Analytics for Motorcycle Theft Detection and RecoveryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Comparative Evaluation of Action of RISA and Sodium Hypochlorite on the Surface Roughness of Heat Treated Single Files, Hyflex EDM and One Curve- An Atomic Force Microscopic StudyDocument5 pagesComparative Evaluation of Action of RISA and Sodium Hypochlorite on the Surface Roughness of Heat Treated Single Files, Hyflex EDM and One Curve- An Atomic Force Microscopic StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Study Assessing Viability of Installing 20kw Solar Power For The Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoDocument6 pagesStudy Assessing Viability of Installing 20kw Solar Power For The Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Unmasking Phishing Threats Through Cutting-Edge Machine LearningDocument8 pagesUnmasking Phishing Threats Through Cutting-Edge Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cyber Security Awareness and Educational Outcomes of Grade 4 LearnersDocument33 pagesCyber Security Awareness and Educational Outcomes of Grade 4 LearnersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Blockchain Based Decentralized ApplicationDocument7 pagesBlockchain Based Decentralized ApplicationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Smart Health Care SystemDocument8 pagesSmart Health Care SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Visual Water: An Integration of App and Web To Understand Chemical ElementsDocument5 pagesVisual Water: An Integration of App and Web To Understand Chemical ElementsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueDocument2 pagesParastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Factors Influencing The Use of Improved Maize Seed and Participation in The Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaDocument6 pagesFactors Influencing The Use of Improved Maize Seed and Participation in The Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Impact of Silver Nanoparticles Infused in Blood in A Stenosed Artery Under The Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in A Sten. Art. Under The Eff. of Mag. FieldDocument6 pagesImpact of Silver Nanoparticles Infused in Blood in A Stenosed Artery Under The Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in A Sten. Art. Under The Eff. of Mag. FieldInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fusco, La Insoportable Levedad de Los SeresDocument18 pagesFusco, La Insoportable Levedad de Los SeresAlby TAnNo ratings yet
- Dua Book 3a Teacher Version 1 Format BDocument60 pagesDua Book 3a Teacher Version 1 Format BHifz HaafizahNo ratings yet
- How To Pass The FSODocument5 pagesHow To Pass The FSODeutsch FrancaisNo ratings yet
- Mechanisms of Baclofen Action On Masticitv: MilanovDocument6 pagesMechanisms of Baclofen Action On Masticitv: MilanovNacho MicheloniNo ratings yet
- Amazing Grace (My Chains Are Gone)Document33 pagesAmazing Grace (My Chains Are Gone)kennethl_41No ratings yet
- 4th WeekDocument3 pages4th WeekMaricar Narag SalvaNo ratings yet
- Different Variables: Laiba Ijaz - Operational ResearchDocument26 pagesDifferent Variables: Laiba Ijaz - Operational ResearchLaiba MughalNo ratings yet
- Daily Lesson Log GAMABADocument4 pagesDaily Lesson Log GAMABAMarlyvic SuavilloNo ratings yet
- Week 4Document12 pagesWeek 4Norhidayah RahmanNo ratings yet
- Spectrum 3rd ESODocument23 pagesSpectrum 3rd ESOIsalor30% (1)
- Modal Verb CanDocument15 pagesModal Verb CanChoco MartiniNo ratings yet
- Success Through Excess: How Property and Casualty Insurers Are Boosting Profits by Entering The Excess and Surplus MarketDocument32 pagesSuccess Through Excess: How Property and Casualty Insurers Are Boosting Profits by Entering The Excess and Surplus MarketNauman NoorNo ratings yet
- 1 To 4 Overview and Technical AnalysisDocument21 pages1 To 4 Overview and Technical AnalysisnomanNo ratings yet
- Andrew Steele v. United States, 362 F.2d 536, 10th Cir. (1966)Document3 pagesAndrew Steele v. United States, 362 F.2d 536, 10th Cir. (1966)Scribd Government DocsNo ratings yet
- AlzheimerDocument8 pagesAlzheimerKrizhia MacayaonNo ratings yet
- The Merchant of Venice and Jew of Malta InternetDocument34 pagesThe Merchant of Venice and Jew of Malta InternetKashif WaqasNo ratings yet
- Human Right Mahatma Gandhi University BBA CBCS 5-1Document19 pagesHuman Right Mahatma Gandhi University BBA CBCS 5-1Rajesh MgNo ratings yet
- IOS Module NotesDocument99 pagesIOS Module NotesShivani ChoudharyNo ratings yet
- Development of A Reliability Based Design Framework For Transmission Line Structure FoundationsDocument9 pagesDevelopment of A Reliability Based Design Framework For Transmission Line Structure FoundationsNitesh JainNo ratings yet
- People vs. QuiachonDocument7 pagesPeople vs. QuiachonJonimar Coloma QueroNo ratings yet
- EMTDocument127 pagesEMTharryyasirNo ratings yet
- Case Presentation: DR - Prathibha.M.ChachadiDocument28 pagesCase Presentation: DR - Prathibha.M.ChachadiPrathibha M ChachadiNo ratings yet
- Rugby Union Rugby Is A Team Game That .. (Play) in Britain Since The Middle of The 19Document2 pagesRugby Union Rugby Is A Team Game That .. (Play) in Britain Since The Middle of The 19Châu Phạm Thùy GiangNo ratings yet
- Cinosi EDocument2 pagesCinosi ESalwa KamiliaNo ratings yet
- Tlac 3.0 PDFDocument26 pagesTlac 3.0 PDFFook Ngo83% (6)
- Mageo - Jeannette Marie - 2006 - Figurative Dreams Analysis and U.S Traveling IdentitiesDocument33 pagesMageo - Jeannette Marie - 2006 - Figurative Dreams Analysis and U.S Traveling IdentitiesOscar Plens BravoNo ratings yet
- Metropolitan Bank and Trust Company vs. Tobias GR No. 177780 January 25 2012Document6 pagesMetropolitan Bank and Trust Company vs. Tobias GR No. 177780 January 25 2012Ian Jasper R. ManglicmotNo ratings yet
- English Kumarbharati July 2019 STD 10th English Medium SSC Maharashtra State Board Question PaperDocument8 pagesEnglish Kumarbharati July 2019 STD 10th English Medium SSC Maharashtra State Board Question PaperSIDDHESH WADEKARNo ratings yet
- Shear ForceDocument14 pagesShear ForceQayyum Uzear Usin100% (1)
- DevotionDocument34 pagesDevotionmelchor anacionNo ratings yet