You might also like
- Fetal-Placental DisordersFrom EverandFetal-Placental DisordersNicholas S. AssaliRating: 5 out of 5 stars5/5 (1)
- Aphallia Associate Fistula RectouretraDocument3 pagesAphallia Associate Fistula Rectouretraeni nadzhifahNo ratings yet
- Bhanchet 1977Document7 pagesBhanchet 1977zaki ahmadNo ratings yet
- Pathologic Quiz Case: Residents' PageDocument4 pagesPathologic Quiz Case: Residents' Pagejeka222No ratings yet
- Definitivo Taeniasis Girl 2017Document4 pagesDefinitivo Taeniasis Girl 2017Ray SelopNo ratings yet
- Paediatric Urology - Peno-Scrotal: Case 1 Case 2Document2 pagesPaediatric Urology - Peno-Scrotal: Case 1 Case 2HardiTariqHammaNo ratings yet
- Phimosis 5 PDFDocument4 pagesPhimosis 5 PDFNurul YaqinNo ratings yet
- Accessory Urethra, Accessory PhallusDocument7 pagesAccessory Urethra, Accessory PhallusGunduz AgaNo ratings yet
- Jurnal ParotitissDocument2 pagesJurnal ParotitissmarcelinaNo ratings yet
- Laryngomalacia and Swallowing Function in ChildrenDocument7 pagesLaryngomalacia and Swallowing Function in ChildrenmelaniaNo ratings yet
- Palmoplantar Keratoderma and Edentulous Status: Two Isolated Expressions of Papillon-Lefèvre SyndromeDocument4 pagesPalmoplantar Keratoderma and Edentulous Status: Two Isolated Expressions of Papillon-Lefèvre Syndromeseema sharmaNo ratings yet
- Paniculitis Nodular Esteril en PerrosDocument10 pagesPaniculitis Nodular Esteril en PerrosMoisés RodríguezNo ratings yet
- Acne Vulgaris: Clinical PracticeDocument18 pagesAcne Vulgaris: Clinical PracticeSonia Dwi Reina TumanggorNo ratings yet
- Cystic Endometrial Hyperplasia and Pyometra in Three Captive African Hunting Dogs (Lycaon Pictus)Document7 pagesCystic Endometrial Hyperplasia and Pyometra in Three Captive African Hunting Dogs (Lycaon Pictus)Intan Renita Yulianti DrumerNo ratings yet
- Autism and The Gastrointestinal Tract: ReferencesDocument3 pagesAutism and The Gastrointestinal Tract: References__aguNo ratings yet
- Pyloric Stenosis of Infancy - The Great Mystery UnravelsDocument1 pagePyloric Stenosis of Infancy - The Great Mystery UnravelsasclepiuspdfsNo ratings yet
- 61 Goepfert2004Document7 pages61 Goepfert2004angela_karenina_1No ratings yet
- 3 PBDocument4 pages3 PBSuh TeixeiraNo ratings yet
- Heymann2007 PDFDocument2 pagesHeymann2007 PDFNisa UcilNo ratings yet
- Reading Scholarly & Popular SourcesDocument3 pagesReading Scholarly & Popular SourcesNishat MamnoonNo ratings yet
- Stenosis PilorusDocument5 pagesStenosis PilorusNovita ApramadhaNo ratings yet
- Iron Overload and Hepatic Fibrosis in Response - JMDocument1 pageIron Overload and Hepatic Fibrosis in Response - JMBastomy EkaNo ratings yet
- Review of The Evidence On The Closure of Abdominal Wall DefectsDocument8 pagesReview of The Evidence On The Closure of Abdominal Wall DefectsLushaNo ratings yet
- PregnancyTumor GeneralDentistryDocument4 pagesPregnancyTumor GeneralDentistryNguyên TrầnNo ratings yet
- Differentiating Tonsil Cancer From Benign Tonsillar HypertrophyDocument2 pagesDifferentiating Tonsil Cancer From Benign Tonsillar HypertrophyrinamaulizaNo ratings yet
- A Diagnostic Flow Chart For Non-Immune HydropsDocument2 pagesA Diagnostic Flow Chart For Non-Immune HydropsIvan BejarNo ratings yet
- Fop Exams Categorized-2Document285 pagesFop Exams Categorized-2ani KumarNo ratings yet
- Pathologic and Physiologic PhimosisDocument7 pagesPathologic and Physiologic Phimosisdianita507No ratings yet
- Pott's Puffy Tumor in A 12-Year-Old Boy: ReferencesDocument4 pagesPott's Puffy Tumor in A 12-Year-Old Boy: ReferencesssmasterNo ratings yet
- Aplasia Cutis Congenital Type 6 A Rare Type-A Case Report: International Journal of Medical and Health ResearchDocument2 pagesAplasia Cutis Congenital Type 6 A Rare Type-A Case Report: International Journal of Medical and Health ResearchDr. Pedro Javier Cadena GonzálezNo ratings yet
- Acne VulgarisDocument10 pagesAcne Vulgarisbrilian jelitaNo ratings yet
- Acne InggrisDocument20 pagesAcne InggrisSonia Dwi Reina TumanggorNo ratings yet
- Are We Ready For A New Look at The Diagnosis of Premature Rupture of Membranes?Document6 pagesAre We Ready For A New Look at The Diagnosis of Premature Rupture of Membranes?stephaniedianNo ratings yet
- Martin 2017Document6 pagesMartin 2017Peregrine Albertus Ricco AzaliNo ratings yet
- 1 s2.0 S0738081X14002375 MainDocument13 pages1 s2.0 S0738081X14002375 Mainmarisa araujoNo ratings yet
- Prenatal Diagnosis of Congenital Epulis: Implications For DeliveryDocument3 pagesPrenatal Diagnosis of Congenital Epulis: Implications For DeliveryRiznasyarielia Nikmatun NafisahNo ratings yet
- A Study of Inguinal Hernia in ChildrenDocument5 pagesA Study of Inguinal Hernia in ChildrenrhmathidayatNo ratings yet
- Review Adolescent Endometriosis: An Update: Jessica Y. Shim MD, Marc R. Laufer MDDocument8 pagesReview Adolescent Endometriosis: An Update: Jessica Y. Shim MD, Marc R. Laufer MDIntan PermataNo ratings yet
- Plunging Ranula - Case Report EZADocument9 pagesPlunging Ranula - Case Report EZAreza kurniawanNo ratings yet
- Black UrineDocument2 pagesBlack Urinejoudi.jou95No ratings yet
- 1 s2.0 S0022522319430018 MainDocument13 pages1 s2.0 S0022522319430018 Mainnanda advocateNo ratings yet
- 292-Article Text-1640-1-10-20190515Document8 pages292-Article Text-1640-1-10-20190515Liset Edreira Cutipa SallucaNo ratings yet
- Benign Lesions of PinnaDocument4 pagesBenign Lesions of Pinnamanoj kumarNo ratings yet
- Incidence of Bronchiolitis Associated HospitalizatDocument2 pagesIncidence of Bronchiolitis Associated HospitalizatBastomy EkaNo ratings yet
- Journal of Pediatric Surgery CASE REPORTSDocument4 pagesJournal of Pediatric Surgery CASE REPORTSwidyaNo ratings yet
- Cute Appendicitis in Children: Emergency Department Diagnosis and ManagementDocument13 pagesCute Appendicitis in Children: Emergency Department Diagnosis and ManagementMusyawarah MelalaNo ratings yet
- Ross2007 Abs AjogDocument2 pagesRoss2007 Abs AjogAbdillah FauziNo ratings yet
- Retracted: Ileal-Lymphoid-Nodular Hyperplasia, Non-Specific Colitis, and Pervasive Developmental Disorder in ChildrenDocument5 pagesRetracted: Ileal-Lymphoid-Nodular Hyperplasia, Non-Specific Colitis, and Pervasive Developmental Disorder in Children__aguNo ratings yet
- Preuritic Urticarial Papule and Plaque of PregnancyDocument5 pagesPreuritic Urticarial Papule and Plaque of PregnancyNoraNo ratings yet
- Ileal-Lymphoid-Nodular Hyperplasia, Non-Specific Colitis, and Pervasive Developmental Disorder in ChildrenDocument11 pagesIleal-Lymphoid-Nodular Hyperplasia, Non-Specific Colitis, and Pervasive Developmental Disorder in ChildrenEmmanuelLeidiNo ratings yet
- Non-Immune Fetal Hydrops: Are We Doing The Appropriate Tests Each Time?Document3 pagesNon-Immune Fetal Hydrops: Are We Doing The Appropriate Tests Each Time?dian_067No ratings yet
- Glandula Salivar HeterotopicaDocument2 pagesGlandula Salivar HeterotopicaJuan Esteban RamirezNo ratings yet
- 10 1016@j Jpurol 2017 11 019Document23 pages10 1016@j Jpurol 2017 11 019Cuidados Enfermagem DomicílioNo ratings yet
- Condylomata Acuminata in Children: Abstract: We Describe A Study On 38 Children From 1 To 11 Years of AgeDocument3 pagesCondylomata Acuminata in Children: Abstract: We Describe A Study On 38 Children From 1 To 11 Years of AgeJoe DoeNo ratings yet
- AUR in ChildrenDocument1 pageAUR in ChildrenStaporn KasemsripitakNo ratings yet
- Case ReportDocument6 pagesCase ReportGladishNo ratings yet
- 10 1016@j Ajog 2019 07 010 PDFDocument13 pages10 1016@j Ajog 2019 07 010 PDFDaniel GamarraNo ratings yet
- Pathologic and Physiologic PhimosisDocument4 pagesPathologic and Physiologic PhimosisJuwita PratiwiNo ratings yet
- Case Reports Esophageal Foreign Body in NeonatesDocument3 pagesCase Reports Esophageal Foreign Body in NeonatesmuhammadpanggihpangestuNo ratings yet
- Hypersensitivity ReactionDocument1 pageHypersensitivity ReactionSanielle Karla Garcia LorenzoNo ratings yet
- Diabetes Mellitus Type 2Document1 pageDiabetes Mellitus Type 2Sanielle Karla Garcia LorenzoNo ratings yet
- Karl Avillo - MicrobiologyDocument16 pagesKarl Avillo - MicrobiologySanielle Karla Garcia LorenzoNo ratings yet
- PX Niedo Aniolina JI Bonilla Jenelyn U.Document8 pagesPX Niedo Aniolina JI Bonilla Jenelyn U.Sanielle Karla Garcia LorenzoNo ratings yet
- Rad 1.05a Case Reports-1Document7 pagesRad 1.05a Case Reports-1Sanielle Karla Garcia LorenzoNo ratings yet
- Starbucks Cheat SheetDocument4 pagesStarbucks Cheat SheetSanielle Karla Garcia LorenzoNo ratings yet
- AbrasionDocument1 pageAbrasionSanielle Karla Garcia LorenzoNo ratings yet
- ClinPath-10.2 - Urine and Other Body FluidsDocument4 pagesClinPath-10.2 - Urine and Other Body FluidsSanielle Karla Garcia LorenzoNo ratings yet
- General Instructions To Examinees Professional Regulation CommissionDocument1 pageGeneral Instructions To Examinees Professional Regulation CommissionSanielle Karla Garcia LorenzoNo ratings yet
- Karl Avillo - Legal MedicineDocument17 pagesKarl Avillo - Legal MedicineSanielle Karla Garcia Lorenzo100% (1)
- Prev Med Mar 2022Document8 pagesPrev Med Mar 2022Sanielle Karla Garcia LorenzoNo ratings yet
- ANATOMY VERSUS, CLINICAL CORRELATIONS AND MUST KNOWS by LonelybitterDocument18 pagesANATOMY VERSUS, CLINICAL CORRELATIONS AND MUST KNOWS by LonelybitterSanielle Karla Garcia LorenzoNo ratings yet
- FEU Gyne Ratio Finals COMPLETE 1Document36 pagesFEU Gyne Ratio Finals COMPLETE 1Sanielle Karla Garcia LorenzoNo ratings yet
- Down The StretchDocument2 pagesDown The StretchSanielle Karla Garcia LorenzoNo ratings yet
- Internal Medicine Mar 2022Document8 pagesInternal Medicine Mar 2022Sanielle Karla Garcia LorenzoNo ratings yet
- FCM SE 1 - MergedDocument111 pagesFCM SE 1 - MergedSanielle Karla Garcia LorenzoNo ratings yet
- PLE Practice Exam Day 2Document7 pagesPLE Practice Exam Day 2Sanielle Karla Garcia LorenzoNo ratings yet
- PLE Practice Exam Day 3Document10 pagesPLE Practice Exam Day 3Sanielle Karla Garcia LorenzoNo ratings yet
- PLE Practice Exam Day 1Document8 pagesPLE Practice Exam Day 1Sanielle Karla Garcia LorenzoNo ratings yet
- 2019 ENNS Dissemination - Vitamin ADocument48 pages2019 ENNS Dissemination - Vitamin ASanielle Karla Garcia LorenzoNo ratings yet
- PLE Practice Exam Day 4Document7 pagesPLE Practice Exam Day 4Sanielle Karla Garcia LorenzoNo ratings yet
- Anatomy Pearls: Jimffel A. Tejada, PTRP, MDDocument13 pagesAnatomy Pearls: Jimffel A. Tejada, PTRP, MDSanielle Karla Garcia Lorenzo100% (1)
- Day 4 WK 2Document8 pagesDay 4 WK 2Sanielle Karla Garcia LorenzoNo ratings yet
- PH - 7.28 Pco2 - 28Mmhg Hco3 - 14Meqs/L: Metabolic Acidosis, Partially CompensatedDocument27 pagesPH - 7.28 Pco2 - 28Mmhg Hco3 - 14Meqs/L: Metabolic Acidosis, Partially CompensatedSanielle Karla Garcia LorenzoNo ratings yet
- Day 3 WK 2Document9 pagesDay 3 WK 2Sanielle Karla Garcia LorenzoNo ratings yet
- Day 1 Ple Practice Exam Week 2: BiochemistryDocument8 pagesDay 1 Ple Practice Exam Week 2: BiochemistrySanielle Karla Garcia LorenzoNo ratings yet
- PLE Crammer TypeDocument3 pagesPLE Crammer TypeSanielle Karla Garcia Lorenzo100% (1)
- Day 2 WK 2Document8 pagesDay 2 WK 2Sanielle Karla Garcia LorenzoNo ratings yet
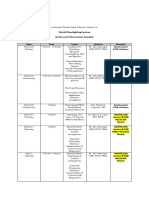
- Hybrid Moonlighting Seminar ScheduleDocument2 pagesHybrid Moonlighting Seminar ScheduleSanielle Karla Garcia LorenzoNo ratings yet
- ADocument21 pagesACarlene GomesNo ratings yet
- Technical Information ASSET DOC LOC 17687504Document23 pagesTechnical Information ASSET DOC LOC 17687504SuparnoNo ratings yet
- 2019 Iran PPRDocument10 pages2019 Iran PPRFareena FatimaNo ratings yet
- Aft MPM Cafs 01Document2 pagesAft MPM Cafs 01Forum PompieriiNo ratings yet
- 21 Lesson For 21st CenturyDocument16 pages21 Lesson For 21st CenturySamia GhafoorNo ratings yet
- Shiloh 2019Document24 pagesShiloh 2019Daniel Ojevwe100% (1)
- Arrangement of The Posterior TeethDocument6 pagesArrangement of The Posterior Teethsamiran vaidyaNo ratings yet
- Operation Husky Sicily 1943: Maj R L SimmonsDocument27 pagesOperation Husky Sicily 1943: Maj R L SimmonsStent21No ratings yet
- Module 3 TD 8 WEEK3Document8 pagesModule 3 TD 8 WEEK3meraaguilanNo ratings yet
- Worksheet 8: Language HandbookDocument2 pagesWorksheet 8: Language HandbookMrs BeyNo ratings yet
- Automatic Drainage Cleaning SystemDocument42 pagesAutomatic Drainage Cleaning SystemAnonymous j0aO95fg100% (2)
- Ansi Ies RP-8-21Document547 pagesAnsi Ies RP-8-21cristianbaileyeNo ratings yet
- EMD Tools1Document55 pagesEMD Tools1Vladimir ArsicNo ratings yet
- B1+ UNIT 3 Extra Grammar Practice RevisionDocument1 pageB1+ UNIT 3 Extra Grammar Practice RevisionRetox Borukov0% (2)
- Unit Homework Momentum Its Conservation Ans KeyDocument6 pagesUnit Homework Momentum Its Conservation Ans KeyKristyne Olicia100% (1)
- Biology AS ClassifiedDocument209 pagesBiology AS ClassifiedMaaz Rashid100% (2)
- TEGOPAC Bond251 012016Document2 pagesTEGOPAC Bond251 012016Pranshu JainNo ratings yet
- Dave Stevenson: DetailsDocument2 pagesDave Stevenson: DetailsPhethego Caprivian MokgaloNo ratings yet
- 0748640843Document273 pages0748640843Zia Ullah100% (1)
- Chapter 1Document21 pagesChapter 1sibi samsonNo ratings yet
- Escherichia Coli O157:H7 Issues and Ramifications: Executive SummaryDocument12 pagesEscherichia Coli O157:H7 Issues and Ramifications: Executive SummaryTinnysumardiNo ratings yet
- Abstract Book Leish World Congress 5Document1,116 pagesAbstract Book Leish World Congress 5libremdNo ratings yet
- TDS - Pidicryl 120V - UpdatedDocument1 pageTDS - Pidicryl 120V - Updatedhai nguyenNo ratings yet
- MOV S ManualDocument84 pagesMOV S ManualAbdulrahmanNo ratings yet
- Activity Sheet - Radioactive DecayDocument5 pagesActivity Sheet - Radioactive DecayAkshat jhaNo ratings yet
- Siemens MCB Price List Wef 15-10-2023Document60 pagesSiemens MCB Price List Wef 15-10-2023M/S.TEJEET ELECTRICAL & ENGG. CORP.No ratings yet
- Beacon Atlantic Short Spec R1 141118 NBDocument4 pagesBeacon Atlantic Short Spec R1 141118 NBRayodcNo ratings yet
- RS PRO Digital, Bench Power Supply, 217W, 3 Output, 0 32V 3 A, 5 ADocument5 pagesRS PRO Digital, Bench Power Supply, 217W, 3 Output, 0 32V 3 A, 5 AGuillaume FoubertNo ratings yet
- Master ILO Tools Templates - Desk TopDocument61 pagesMaster ILO Tools Templates - Desk TopVenkatesanNo ratings yet
- Cambridge International Advanced Subsidiary and Advanced LevelDocument12 pagesCambridge International Advanced Subsidiary and Advanced LevelTerTalks ChikweyaNo ratings yet