You might also like
- Clostridium Difficile: Its Role in Intestinal DiseaseFrom EverandClostridium Difficile: Its Role in Intestinal DiseaseRial D. RolfeRating: 3.5 out of 5 stars3.5/5 (32)
- PLE Practice Exam Day 4Document7 pagesPLE Practice Exam Day 4Sanielle Karla Garcia LorenzoNo ratings yet
- Complications of Labor and DeliveryDocument5 pagesComplications of Labor and DeliveryJill Hill100% (1)
- Obstetrics: Positive, But Upon Workup There Is No Pregnancy. It's D/T Cross Reaction To HCGDocument6 pagesObstetrics: Positive, But Upon Workup There Is No Pregnancy. It's D/T Cross Reaction To HCGPencenk AzznewNo ratings yet
- Obstetrics 2.01 AbortionDocument10 pagesObstetrics 2.01 AbortionJyl Yan SelasorNo ratings yet
- Complications of Labor and DeliveryDocument5 pagesComplications of Labor and DeliveryLovelyn Joy Abubo CortezNo ratings yet
- اسئله نسائيه مدققه-2 740795Document42 pagesاسئله نسائيه مدققه-2 740795Ashraf AlbhlaNo ratings yet
- Ectopic PregnancyDocument6 pagesEctopic PregnancyChristine Evan HoNo ratings yet
- Board Exam OB GYNDocument7 pagesBoard Exam OB GYNMitch C.No ratings yet
- (Documen T Title) : (Document Subtitle)Document24 pages(Documen T Title) : (Document Subtitle)Gebretsadik GebregergisNo ratings yet
- Maternal Test Questions 2Document7 pagesMaternal Test Questions 2dhodejun lizhaldeNo ratings yet
- 05.1 Obstructed Labor and Problems of The PassengerDocument16 pages05.1 Obstructed Labor and Problems of The PassengerJAN CAMILLE LENONNo ratings yet
- Book CBSE-Class-12-Biology-Reproductive-Health-Practice-QuestionsDocument9 pagesBook CBSE-Class-12-Biology-Reproductive-Health-Practice-QuestionsVikramNo ratings yet
- Scribd OB 4Document5 pagesScribd OB 4Ralph Tama Mangacop BenitoNo ratings yet
- 2024 Ob MaterialsDocument11 pages2024 Ob MaterialsJoshelle AndradeNo ratings yet
- Obs FitnessDocument6 pagesObs FitnessSchiganger MayalaNo ratings yet
- Hemorrhage in PregnancyDocument119 pagesHemorrhage in PregnancyTrina CabilitasanNo ratings yet
- MCQs-Bank Obestetrics-Dr-Ahmed-Walid - Proffesor of Obs & Gyn - Benha Faculty of MedicineDocument140 pagesMCQs-Bank Obestetrics-Dr-Ahmed-Walid - Proffesor of Obs & Gyn - Benha Faculty of MedicineAhmed AnwarNo ratings yet
- 02 First Trimester ConditionsDocument12 pages02 First Trimester ConditionsJAN CAMILLE LENONNo ratings yet
- Chapter 11-13 MATERNALDocument17 pagesChapter 11-13 MATERNALKaryll RomeroNo ratings yet
- MCN MT1 RefresherDocument7 pagesMCN MT1 RefresherRogerQuxNo ratings yet
- OB FC Nov 2021 NLEDocument9 pagesOB FC Nov 2021 NLEAlyssa SaibiNo ratings yet
- Self Assessment QuestionsDocument3 pagesSelf Assessment QuestionskhongjacmunNo ratings yet
- Panduan Lengkap NikahDocument5 pagesPanduan Lengkap NikahKitty YuffieNo ratings yet
- Prractice TestDocument23 pagesPrractice TestRoscelie KhoNo ratings yet
- MCN 2Document8 pagesMCN 2Nicole Dela TorreNo ratings yet
- اسئله نسائيه)Document47 pagesاسئله نسائيه)ملك عيسىNo ratings yet
- OB-GYN Board Exam QuestionsDocument11 pagesOB-GYN Board Exam QuestionsJo Anne94% (17)
- Sample MCQ QuestionsDocument11 pagesSample MCQ QuestionsPreeti Chouhan100% (1)
- Obg MCQS PDFDocument11 pagesObg MCQS PDFPreeti ChouhanNo ratings yet
- AbortionDocument32 pagesAbortionmani_mandeep262519100% (1)
- Revision Set 2Document12 pagesRevision Set 2Effa Emily100% (1)
- 04-05 - LEC Intrapartal Care and The Labor PhenomenonDocument29 pages04-05 - LEC Intrapartal Care and The Labor PhenomenonJAN CAMILLE LENONNo ratings yet
- B4Y5G3 O - G - With AnswersDocument6 pagesB4Y5G3 O - G - With AnswersZeke EdgeNo ratings yet
- Early Obstetric HemorrhageDocument23 pagesEarly Obstetric HemorrhageDianne GalangNo ratings yet
- Short Quiz in Science 7 Describe The Process of FertilizationDocument1 pageShort Quiz in Science 7 Describe The Process of FertilizationLINDSY MAE SULA-SULANo ratings yet
- Prepared By: Niko T. ManaliliDocument3 pagesPrepared By: Niko T. Manaliliiko552000No ratings yet
- Obstetrics Test 1Document3 pagesObstetrics Test 1Errold Joseph LahaganNo ratings yet
- Mid 104 ReqDocument3 pagesMid 104 ReqErika Mae RevadiloNo ratings yet
- Ob Prelim Evaluation 1St Semester 2015 1 of 2: Mec ElinoDocument9 pagesOb Prelim Evaluation 1St Semester 2015 1 of 2: Mec ElinoagilNo ratings yet
- Bonus: Here's Your Perfect By: Jamie MILLERDocument47 pagesBonus: Here's Your Perfect By: Jamie MILLERJack KayatNo ratings yet
- Dwnload Full Introduction To Maternity Pediatric Nursing 6th Edition Leifer Solutions Manual PDFDocument36 pagesDwnload Full Introduction To Maternity Pediatric Nursing 6th Edition Leifer Solutions Manual PDFgreeningquinovic25yn2100% (12)
- Full Download Introduction To Maternity Pediatric Nursing 6th Edition Leifer Solutions ManualDocument36 pagesFull Download Introduction To Maternity Pediatric Nursing 6th Edition Leifer Solutions Manualrakicrodwanb100% (28)
- ExamsDocument14 pagesExamssharon chuaNo ratings yet
- Care of Mother, Child, Family and Population Group At-Risk or With Problems By: Leani G. BongayonDocument5 pagesCare of Mother, Child, Family and Population Group At-Risk or With Problems By: Leani G. BongayonChrizelle Esperanzate FlorentinoNo ratings yet
- MCN Make Shift TestDocument9 pagesMCN Make Shift TestmaxynezolayvarNo ratings yet
- Maternal Notes Part IDocument21 pagesMaternal Notes Part Iabbycruz012No ratings yet
- Sexuality Today 11th Edition Kelly Test BankDocument15 pagesSexuality Today 11th Edition Kelly Test Banksamanthasimonnatjrwefky100% (12)
- Post Test DR LevelDocument4 pagesPost Test DR Levelbaraderoayyah41No ratings yet
- Maternal and Child Health Nursing MCQ 9Document22 pagesMaternal and Child Health Nursing MCQ 9shanika67% (6)
- 2ND Quarter 2023 Answer KeyDocument19 pages2ND Quarter 2023 Answer KeyKlarish Ann IgnacioNo ratings yet
- 2022 Ob2 s1t15 Preterm Labor and BirthDocument12 pages2022 Ob2 s1t15 Preterm Labor and BirthmedicoNo ratings yet
- Legal Med 2.03 Birth, Abortion, InfanticideDocument5 pagesLegal Med 2.03 Birth, Abortion, InfanticideKristine FabellonNo ratings yet
- MCN20220 Reviewer 20Document33 pagesMCN20220 Reviewer 20Krizelle MesinaNo ratings yet
- Rec!!!Document10 pagesRec!!!collinsmagNo ratings yet
- Sexuality Today 11th Edition Kelly Test BankDocument15 pagesSexuality Today 11th Edition Kelly Test Bankteresa100% (23)
- IBQs & MCQsDocument58 pagesIBQs & MCQsskNo ratings yet
- MID101 Final ExaminationDocument10 pagesMID101 Final ExaminationAldrin Riel BoyanoNo ratings yet
- MCN ReviewerDocument3 pagesMCN ReviewerJunghoon YangParkNo ratings yet
- Hypersensitivity ReactionDocument1 pageHypersensitivity ReactionSanielle Karla Garcia LorenzoNo ratings yet
- Diabetes Mellitus Type 2Document1 pageDiabetes Mellitus Type 2Sanielle Karla Garcia LorenzoNo ratings yet
- Rad 1.05a Case Reports-1Document7 pagesRad 1.05a Case Reports-1Sanielle Karla Garcia LorenzoNo ratings yet
- General Instructions To Examinees Professional Regulation CommissionDocument1 pageGeneral Instructions To Examinees Professional Regulation CommissionSanielle Karla Garcia LorenzoNo ratings yet
- ClinPath-10.2 - Urine and Other Body FluidsDocument4 pagesClinPath-10.2 - Urine and Other Body FluidsSanielle Karla Garcia LorenzoNo ratings yet
- Starbucks Cheat SheetDocument4 pagesStarbucks Cheat SheetSanielle Karla Garcia LorenzoNo ratings yet
- AbrasionDocument1 pageAbrasionSanielle Karla Garcia LorenzoNo ratings yet
- PX Niedo Aniolina JI Bonilla Jenelyn U.Document8 pagesPX Niedo Aniolina JI Bonilla Jenelyn U.Sanielle Karla Garcia LorenzoNo ratings yet
- PIIS0022347616311714Document2 pagesPIIS0022347616311714Sanielle Karla Garcia LorenzoNo ratings yet
- Karl Avillo - MicrobiologyDocument16 pagesKarl Avillo - MicrobiologySanielle Karla Garcia LorenzoNo ratings yet
- FEU Gyne Ratio Finals COMPLETE 1Document36 pagesFEU Gyne Ratio Finals COMPLETE 1Sanielle Karla Garcia LorenzoNo ratings yet
- Down The StretchDocument2 pagesDown The StretchSanielle Karla Garcia LorenzoNo ratings yet
- Internal Medicine Mar 2022Document8 pagesInternal Medicine Mar 2022Sanielle Karla Garcia LorenzoNo ratings yet
- Prev Med Mar 2022Document8 pagesPrev Med Mar 2022Sanielle Karla Garcia LorenzoNo ratings yet
- Karl Avillo - Legal MedicineDocument17 pagesKarl Avillo - Legal MedicineSanielle Karla Garcia Lorenzo100% (1)
- ANATOMY VERSUS, CLINICAL CORRELATIONS AND MUST KNOWS by LonelybitterDocument18 pagesANATOMY VERSUS, CLINICAL CORRELATIONS AND MUST KNOWS by LonelybitterSanielle Karla Garcia LorenzoNo ratings yet
- PLE Practice Exam Day 3Document10 pagesPLE Practice Exam Day 3Sanielle Karla Garcia LorenzoNo ratings yet
- PLE Practice Exam Day 2Document7 pagesPLE Practice Exam Day 2Sanielle Karla Garcia LorenzoNo ratings yet
- PLE Practice Exam Day 1Document8 pagesPLE Practice Exam Day 1Sanielle Karla Garcia LorenzoNo ratings yet
- FCM SE 1 - MergedDocument111 pagesFCM SE 1 - MergedSanielle Karla Garcia LorenzoNo ratings yet
- 2019 ENNS Dissemination - Vitamin ADocument48 pages2019 ENNS Dissemination - Vitamin ASanielle Karla Garcia LorenzoNo ratings yet
- Day 1 Ple Practice Exam Week 2: BiochemistryDocument8 pagesDay 1 Ple Practice Exam Week 2: BiochemistrySanielle Karla Garcia LorenzoNo ratings yet
- Anatomy Pearls: Jimffel A. Tejada, PTRP, MDDocument13 pagesAnatomy Pearls: Jimffel A. Tejada, PTRP, MDSanielle Karla Garcia Lorenzo100% (1)
- Day 3 WK 2Document9 pagesDay 3 WK 2Sanielle Karla Garcia LorenzoNo ratings yet
- PH - 7.28 Pco2 - 28Mmhg Hco3 - 14Meqs/L: Metabolic Acidosis, Partially CompensatedDocument27 pagesPH - 7.28 Pco2 - 28Mmhg Hco3 - 14Meqs/L: Metabolic Acidosis, Partially CompensatedSanielle Karla Garcia LorenzoNo ratings yet
- PLE Crammer TypeDocument3 pagesPLE Crammer TypeSanielle Karla Garcia Lorenzo100% (1)
- Day 2 WK 2Document8 pagesDay 2 WK 2Sanielle Karla Garcia LorenzoNo ratings yet
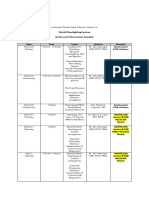
- Hybrid Moonlighting Seminar ScheduleDocument2 pagesHybrid Moonlighting Seminar ScheduleSanielle Karla Garcia LorenzoNo ratings yet
- Herpetic StomatitisDocument21 pagesHerpetic StomatitisZulfahmi RizkiNo ratings yet
- InPatient Claim Form - Jubilee Life InsuranceDocument2 pagesInPatient Claim Form - Jubilee Life InsuranceAhmad Zubair40% (5)
- Riverside County Teachers Union Letter To The Riverside County Office of EducationDocument2 pagesRiverside County Teachers Union Letter To The Riverside County Office of EducationBeau YarbroughNo ratings yet
- Undangan Seminar Internasional 2021-DikonversiDocument4 pagesUndangan Seminar Internasional 2021-DikonversiJandi PermadiNo ratings yet
- NutrientsDocument13 pagesNutrientsUnknown ScoutNo ratings yet
- Ectopic Pregnancy For Med Students ExplainedDocument2 pagesEctopic Pregnancy For Med Students Explainedmartin magdenoskiNo ratings yet
- DLR Verification IMEDDocument2 pagesDLR Verification IMEDEvan MorshadNo ratings yet
- Med Surg BkatDocument8 pagesMed Surg BkatLucilia Nunes0% (1)
- 2022 Summer Research Internship ProgramDocument2 pages2022 Summer Research Internship ProgramNicole SwenartonNo ratings yet
- Retroperitoneal Appendicitis: A Surgical Dilemma: Euroasian Journal of Hepato-Gastroenterology January 2013Document3 pagesRetroperitoneal Appendicitis: A Surgical Dilemma: Euroasian Journal of Hepato-Gastroenterology January 2013putraNo ratings yet
- Answer: Nama: Indriyani NIM: 1702014Document3 pagesAnswer: Nama: Indriyani NIM: 1702014Ayu SamudraNo ratings yet
- List of Hospitals Gujarat PDFDocument11 pagesList of Hospitals Gujarat PDFVijay ChaudharyNo ratings yet
- Case For Acute GastroenteritisDocument26 pagesCase For Acute GastroenteritisSheana TmplNo ratings yet
- Iqvia Covid 19 Eu4 and Uk NewsletterDocument82 pagesIqvia Covid 19 Eu4 and Uk NewsletterKaushal BhattNo ratings yet
- Biology Investigatory ProjectDocument14 pagesBiology Investigatory Projectdesaipiyush1234No ratings yet
- 2016 Emergency and Trauma Radiology - A Teaching File Opt VXDocument415 pages2016 Emergency and Trauma Radiology - A Teaching File Opt VXRe S100% (5)
- Isfm HipertiroidismoDocument17 pagesIsfm HipertiroidismoMaria Rodriguez RodrguezNo ratings yet
- FINAL CervicalCA7BDocument6 pagesFINAL CervicalCA7BRommel OliverasNo ratings yet
- Resident - Handbook - January 2016 - Final PDFDocument205 pagesResident - Handbook - January 2016 - Final PDFAliAlissa85No ratings yet
- Nursing Philosophy UpdatedDocument9 pagesNursing Philosophy Updatedapi-581236671No ratings yet
- Gingivectomy SeminarDocument64 pagesGingivectomy SeminarKrishan GuliaNo ratings yet
- Form 2 - Patient Conduction Form FrontDocument2 pagesForm 2 - Patient Conduction Form FrontMdrrmo Pamplona Camarines SurNo ratings yet
- Amyotrophic Lateral Sclerosis (ALS)Document19 pagesAmyotrophic Lateral Sclerosis (ALS)adilabasi100% (1)
- Tugas Bahasa InggrisDocument3 pagesTugas Bahasa InggrisWendylina BuikNo ratings yet
- New Flow Pasien Igd 11 November 2023 RinaDocument7 pagesNew Flow Pasien Igd 11 November 2023 RinasayaseorangdokterNo ratings yet
- PED Concept MapDocument1 pagePED Concept MapSamantha Smith PetiniotNo ratings yet
- Correction Factor PET PDFDocument6 pagesCorrection Factor PET PDFAnonymous NKvozome5No ratings yet
- tm6260 51 99-2 September2008Document43 pagestm6260 51 99-2 September2008anil nsNo ratings yet
- Nima CVDocument3 pagesNima CVNivya Susan SabuNo ratings yet
- Andre FE (2008) - Vaccination Greatly Reduces Disease, Disability, Death and Inequity Worldwide PDFDocument7 pagesAndre FE (2008) - Vaccination Greatly Reduces Disease, Disability, Death and Inequity Worldwide PDFHoa NắngNo ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (4)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (39)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (5)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (83)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeRating: 4.5 out of 5 stars4.5/5 (3)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (44)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (267)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- I Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionFrom EverandI Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionNo ratings yet
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- The Fun Habit: How the Pursuit of Joy and Wonder Can Change Your LifeFrom EverandThe Fun Habit: How the Pursuit of Joy and Wonder Can Change Your LifeRating: 4.5 out of 5 stars4.5/5 (19)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)
- The Story of Philosophy: The Lives and Opinions of the Greater PhilosophersFrom EverandThe Story of Philosophy: The Lives and Opinions of the Greater PhilosophersNo ratings yet