You might also like
- Assessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsFrom EverandAssessment of Pain Management in Anaesthesia Practice among Nurse AnaesthetistsNo ratings yet
- 2024 Clinical Relevance of Resistance Training in Women With FibromyalgiaDocument16 pages2024 Clinical Relevance of Resistance Training in Women With FibromyalgiaLina M GarciaNo ratings yet
- Whodas Measurement Properties For Women With DysmenorrheaDocument8 pagesWhodas Measurement Properties For Women With Dysmenorrheahanna.oravecz1No ratings yet
- WHODAS Measurement Properties For Women With Dysmenorrhea: Research Open AccessDocument7 pagesWHODAS Measurement Properties For Women With Dysmenorrhea: Research Open Accessokky ocktavNo ratings yet
- 1 s2.0 S2214139116300026 Main PDFDocument8 pages1 s2.0 S2214139116300026 Main PDFAnonymous T4IxYOoBBGNo ratings yet
- Comparison of Numerical and Verbal Rating ScalesDocument8 pagesComparison of Numerical and Verbal Rating ScalesplsssssNo ratings yet
- The Effect of DismenorhoeDocument18 pagesThe Effect of DismenorhoeNarmin FaisalNo ratings yet
- Develomnent of The Wisconsin Brief Pain Question&ire To Assess Pain in Cancer and Other DiseasesDocument14 pagesDevelomnent of The Wisconsin Brief Pain Question&ire To Assess Pain in Cancer and Other DiseasesParisa SattarNo ratings yet
- Ong 139 391Document9 pagesOng 139 391abdi syahputraNo ratings yet
- Studies Were Also Assessed For Bias Using The Cochrane CriteriaDocument12 pagesStudies Were Also Assessed For Bias Using The Cochrane CriteriaAndrio GultomNo ratings yet
- 5 A Systematic Review of The Pain Scales in AdultsDocument12 pages5 A Systematic Review of The Pain Scales in AdultsKepompong KupukupuNo ratings yet
- Skala NyeriDocument20 pagesSkala NyeripuspaNo ratings yet
- Prospective Association Between Dysmenorrhea and CDocument13 pagesProspective Association Between Dysmenorrhea and CSandra PahlmNo ratings yet
- Effects of Matched vs. Unmatched Physical Therapy Interventions On Pain or Disability in Patients With Neck Pain A Systematic Review and Meta-AnalysDocument21 pagesEffects of Matched vs. Unmatched Physical Therapy Interventions On Pain or Disability in Patients With Neck Pain A Systematic Review and Meta-AnalyshrzicajosipNo ratings yet
- Patients' Perception of Acute and Chronic Pain and Their Satisfaction With Care at The General Hospital DoualaDocument8 pagesPatients' Perception of Acute and Chronic Pain and Their Satisfaction With Care at The General Hospital DoualaEditor IJTSRDNo ratings yet
- Nop2 8 2345Document9 pagesNop2 8 2345api-600421611No ratings yet
- 1 s2.0 S1836955319300918 Main PDFDocument7 pages1 s2.0 S1836955319300918 Main PDFJuliano BritoNo ratings yet
- Literature Review DysmenorrheaDocument9 pagesLiterature Review Dysmenorrheaafmzkbuvlmmhqq100% (1)
- Study Literatur: Pengkajian Luka Kaki DiabetesDocument15 pagesStudy Literatur: Pengkajian Luka Kaki DiabetesoctaviamayvikaNo ratings yet
- Academic Emergency Medicine - 2022 - Broder - Guidelines For Reasonable and Appropriate Care in The Emergency Department 2Document36 pagesAcademic Emergency Medicine - 2022 - Broder - Guidelines For Reasonable and Appropriate Care in The Emergency Department 2Dr. Ricardo NegreteNo ratings yet
- Karcioglu 2018Document8 pagesKarcioglu 2018Liana HarnumNo ratings yet
- Comparing Visual-Analog and Numeric Scales For Assessing Menstrual PainDocument4 pagesComparing Visual-Analog and Numeric Scales For Assessing Menstrual PainMelissaNo ratings yet
- AINEsDocument13 pagesAINEsSebastian NamikazeNo ratings yet
- Control of Endometriosis-Associated Pain With Etonogestrel-Releasing Contraceptive Implant and 52mg Levonogestrel ReleaDocument8 pagesControl of Endometriosis-Associated Pain With Etonogestrel-Releasing Contraceptive Implant and 52mg Levonogestrel ReleaYudhistira AdhiNo ratings yet
- European Journal of Pain - 2019 - Aggarwal - The Effectiveness of Self Management Interventions in Adults With ChronicDocument17 pagesEuropean Journal of Pain - 2019 - Aggarwal - The Effectiveness of Self Management Interventions in Adults With ChronicNatalie JaraNo ratings yet
- A Simple Method For Clinical Implications of Pain Comprehensive Geriatric AssessmentDocument6 pagesA Simple Method For Clinical Implications of Pain Comprehensive Geriatric AssessmentAhmedNo ratings yet
- Jurnal Pubmed Tugas Sik 4Document6 pagesJurnal Pubmed Tugas Sik 4srimaryanitellNo ratings yet
- Week 5 Solution-2965087Document8 pagesWeek 5 Solution-2965087Satabdi SamantaNo ratings yet
- Does The Addition of Manual Therapy Approach To A Cervical Exercise Program Improve Clinical Outcomes For Patients With Chronic Neck Pain in Short - and Mid-Term? A Randomized Controlled Trial - PMCDocument26 pagesDoes The Addition of Manual Therapy Approach To A Cervical Exercise Program Improve Clinical Outcomes For Patients With Chronic Neck Pain in Short - and Mid-Term? A Randomized Controlled Trial - PMCEri KafexhiNo ratings yet
- 1 s2.0 S0015028218305685 PDFDocument8 pages1 s2.0 S0015028218305685 PDFYoza FirdaozNo ratings yet
- Surgical Treatment of Endometriosis: Prognostic Factors For Better Quality of LifeDocument6 pagesSurgical Treatment of Endometriosis: Prognostic Factors For Better Quality of LifePutri Tamara DasantosNo ratings yet
- Yoga PoseDocument7 pagesYoga Posetessie teoNo ratings yet
- Cpot ScoreDocument11 pagesCpot ScoreabdulkadirmunsyNo ratings yet
- Informatics 07 00036Document10 pagesInformatics 07 00036Manogna GvNo ratings yet
- Journal Homepage: - : IntroductionDocument8 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Pain: A Literature Review: Angela ChamberlainDocument7 pagesPain: A Literature Review: Angela Chamberlainapi-554398781No ratings yet
- Jurnal 1Document16 pagesJurnal 1Made WindaNo ratings yet
- Pain Assessment DissertationDocument4 pagesPain Assessment DissertationHelpWritingACollegePaperArlington100% (1)
- Systematic Review of Endometriosis Pain Assessment - How To Choose A ScaleDocument17 pagesSystematic Review of Endometriosis Pain Assessment - How To Choose A ScaleardirshajiNo ratings yet
- ModifiedDocument18 pagesModifiedHrishikeshNo ratings yet
- Complementary Therapies in Clinical Practice: Aslı Sis Çelik, Serap Ejder ApayDocument6 pagesComplementary Therapies in Clinical Practice: Aslı Sis Çelik, Serap Ejder Apayyudha adi saputaNo ratings yet
- Evaluation of Biological and Sociodemographic Factors Affecting DysmenorrheaDocument8 pagesEvaluation of Biological and Sociodemographic Factors Affecting Dysmenorrheashinta kusumastutiNo ratings yet
- 412-Article Text-1899-1-10-20221013Document6 pages412-Article Text-1899-1-10-20221013khairanitania1302No ratings yet
- Pediatricpainmanagement: Aarti Gaglani,, Toni GrossDocument12 pagesPediatricpainmanagement: Aarti Gaglani,, Toni GrossCarlos Manuel EscolasticoNo ratings yet
- 1 s2.0 S0965229924000013 MainDocument13 pages1 s2.0 S0965229924000013 MainAsadm HosshNo ratings yet
- Kuesioner American Pain SocietyDocument15 pagesKuesioner American Pain SocietyNamira Firdha KNo ratings yet
- Migraine and Body Mass Index Categories: A Systematic Review and Meta-Analysis of Observational StudiesDocument14 pagesMigraine and Body Mass Index Categories: A Systematic Review and Meta-Analysis of Observational StudiesRetno ManggalihNo ratings yet
- Study of Dienogest For Dysmenorrhea and Pelvic Pain Associated With EndometriosisDocument6 pagesStudy of Dienogest For Dysmenorrhea and Pelvic Pain Associated With Endometriosiskurnia fitriNo ratings yet
- Effect of Physical Activity and Exercise On Endometriosis-Associated Symptom - A Systematic ReviewDocument10 pagesEffect of Physical Activity and Exercise On Endometriosis-Associated Symptom - A Systematic ReviewSabryne RodriguesNo ratings yet
- s12978 018 0453 3 PDFDocument7 pagess12978 018 0453 3 PDFAyu HandokoNo ratings yet
- EBP K3 INTER - DikonversiDocument16 pagesEBP K3 INTER - DikonversiMartha ChristinaNo ratings yet
- Week 5 Solution-2965087Document8 pagesWeek 5 Solution-2965087Satabdi SamantaNo ratings yet
- Costache Cosmin-AndreiiiDocument22 pagesCostache Cosmin-AndreiiiCostache Cosmin-AndreiNo ratings yet
- OBJN Flvia CancerDocument11 pagesOBJN Flvia CancerarunNo ratings yet
- Moore (2014) - The Costs and Consequences of Adequately Managed Chronic Non-Cancer Pain and Chronic Neuropathic PainDocument16 pagesMoore (2014) - The Costs and Consequences of Adequately Managed Chronic Non-Cancer Pain and Chronic Neuropathic PainLuciana AraújoNo ratings yet
- Physical Therapy For BeginnersDocument4 pagesPhysical Therapy For BeginnersBogart MacatangayNo ratings yet
- Disability and Related Factors in Patients With Chronic Cervical Myofascial PainDocument8 pagesDisability and Related Factors in Patients With Chronic Cervical Myofascial Painaria tristayanthiNo ratings yet
- MB6 OG LP 2 RoshilDocument5 pagesMB6 OG LP 2 RoshilRoshilNo ratings yet
- 2015 Article 4193Document12 pages2015 Article 4193Abid Hasan KhanNo ratings yet
- 9 FullDocument15 pages9 FulllipemagalhaesNo ratings yet
- MEDI-Q - English Menstrual Distress Questionnaire (MEDI-Q)Document6 pagesMEDI-Q - English Menstrual Distress Questionnaire (MEDI-Q)hanna.oravecz1No ratings yet
- Relationship Between Menstruation-Related Experiences and Health-Related Quality of Life of Japanese High School Students: A Cross Sectional StudyDocument8 pagesRelationship Between Menstruation-Related Experiences and Health-Related Quality of Life of Japanese High School Students: A Cross Sectional Studyhanna.oravecz1No ratings yet
- Vigorous Physical Activity, Mental Health, Perceived Stress, and Socializing Among College StudentsDocument18 pagesVigorous Physical Activity, Mental Health, Perceived Stress, and Socializing Among College Studentshanna.oravecz1No ratings yet
- A Group of 500 Women Whose Health May Depart Notably From The Norm: Protocol For A Cross-Sectional SurveyDocument12 pagesA Group of 500 Women Whose Health May Depart Notably From The Norm: Protocol For A Cross-Sectional Surveyhanna.oravecz1No ratings yet
- The Relationship Between Physical Activity Level and Dysmenorrhoea in Young WomenDocument5 pagesThe Relationship Between Physical Activity Level and Dysmenorrhoea in Young Womenhanna.oravecz1No ratings yet
- TheMidascode PDFDocument171 pagesTheMidascode PDFJoseph Riccardo75% (4)
- Online Examination Full ReportDocument119 pagesOnline Examination Full Reportjvdsyd100% (1)
- Brunnstrom's Movement Therapy in Hemiplegic Patient (Lower Limb)Document71 pagesBrunnstrom's Movement Therapy in Hemiplegic Patient (Lower Limb)Barney Cordova100% (1)
- Khauv, Britney ResumeDocument2 pagesKhauv, Britney Resumeapi-281920805No ratings yet
- Road Safety ProposalDocument10 pagesRoad Safety ProposalMinatiBindhani78% (18)
- BotnariDocument12 pagesBotnariAlexey DarievNo ratings yet
- Force UsersDocument64 pagesForce UsersLuftWulf100% (7)
- STAAR General BrochureDocument2 pagesSTAAR General BrochureChs BroncosNo ratings yet
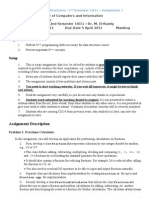
- Objectives: Assignment DescriptionDocument3 pagesObjectives: Assignment DescriptionEng Samar MostafaNo ratings yet
- Multigenre ProjectDocument13 pagesMultigenre Projectapi-429615976No ratings yet
- PreciControl AMH - Ms 06709966190.V2.EnDocument2 pagesPreciControl AMH - Ms 06709966190.V2.EnARIF AHAMMED PNo ratings yet
- Personality and CultureDocument31 pagesPersonality and CultureDavid Green100% (1)
- JAC Chandigarh Information BrochureDocument115 pagesJAC Chandigarh Information BrochureMota ChashmaNo ratings yet
- Usntps FTM 103Document684 pagesUsntps FTM 103unstamper100% (1)
- An Investigation Into The Personality (URJ, 2018, Vol.11, No.5)Document18 pagesAn Investigation Into The Personality (URJ, 2018, Vol.11, No.5)Lets LearnNo ratings yet
- DFMA Class AssignmentsDocument2 pagesDFMA Class Assignmentsr_rame76No ratings yet
- Community Oriented Primary Care: Book TitleDocument2 pagesCommunity Oriented Primary Care: Book Titlexxxxyyyyy1234No ratings yet
- Biochemical Biomarkers in Alzheimer's DiseaseDocument150 pagesBiochemical Biomarkers in Alzheimer's DiseaseInternational Medical PublisherNo ratings yet
- Enhancing Security Using Digital Image ProcessingDocument9 pagesEnhancing Security Using Digital Image ProcessingArulmozhi PugazhenthiNo ratings yet
- The Managerial Process of Crafting and Executing StrategyDocument2 pagesThe Managerial Process of Crafting and Executing StrategyCristian BlejeruNo ratings yet
- BooksDocument3 pagesBookspharma4uNo ratings yet
- A Pragmatic Legal Expert SystemDocument406 pagesA Pragmatic Legal Expert SystemJames Popple0% (1)
- III (2) Subjunctive Mood STDocument30 pagesIII (2) Subjunctive Mood STgocan12-1No ratings yet
- The Debate Between Feuerbach and Stirner An Introduction Frederic GordonDocument9 pagesThe Debate Between Feuerbach and Stirner An Introduction Frederic GordonLibrairie IneffableNo ratings yet
- 5 WORDS A WEEK/Reading Selections-ElementaryDocument3 pages5 WORDS A WEEK/Reading Selections-ElementaryGhebre PalloNo ratings yet
- Template Research ProjectDocument13 pagesTemplate Research ProjectTuấn Anh Đoàn CôngNo ratings yet
- Design and Analysis of Algorithm SyllabusDocument3 pagesDesign and Analysis of Algorithm SyllabusChoyoChoyoNo ratings yet
- D 4393 - 02 RdqzotmDocument7 pagesD 4393 - 02 RdqzotmJuanNo ratings yet
- Ta 06 CatDocument60 pagesTa 06 CatevanNo ratings yet
- 2 F.L Annual Learning Progression By. MR Benguemmar NacerDocument4 pages2 F.L Annual Learning Progression By. MR Benguemmar NacerNouzha Akoh100% (1)