You might also like
- Test Bank For Neuroscience Fundamentals For Rehabilitation 4th Edition by Lundy EkmanDocument24 pagesTest Bank For Neuroscience Fundamentals For Rehabilitation 4th Edition by Lundy EkmanDonaldSmithwrmc100% (45)
- MCQs in Applied Basic Sciences For The Primary FRCSDocument127 pagesMCQs in Applied Basic Sciences For The Primary FRCSGiovanni Henry100% (1)
- Small Animal Spinal Disorders (Second Edition)Document369 pagesSmall Animal Spinal Disorders (Second Edition)Aline Constantino100% (3)
- Essential Clinically Applied Anatomy of the Peripheral Nervous System in the LimbsFrom EverandEssential Clinically Applied Anatomy of the Peripheral Nervous System in the LimbsNo ratings yet
- USMLE High Yield Internal Medicine Notes-Part I 2020Document19 pagesUSMLE High Yield Internal Medicine Notes-Part I 2020usmlematerials.netNo ratings yet
- Biod 152 Final ExamDocument86 pagesBiod 152 Final Examandrew kasaineNo ratings yet
- Small Animal Spinal Disorders Diagnosis and Surgery, 2nd Edition (Vetbooks - Ir)Document369 pagesSmall Animal Spinal Disorders Diagnosis and Surgery, 2nd Edition (Vetbooks - Ir)ghimboasaNo ratings yet
- CVA Case PresentationDocument8 pagesCVA Case Presentationrichie_chan_2100% (3)
- The Linguistic CerebellumFrom EverandThe Linguistic CerebellumPeter MariënRating: 5 out of 5 stars5/5 (2)
- TB-Chapter 24 Neurologic System PDFDocument24 pagesTB-Chapter 24 Neurologic System PDFShawya Assadi100% (3)
- Neurosurgery - Specific Considerations - Schwartz's Principles of Surgery ABSITE and Board Review, 9th EdDocument17 pagesNeurosurgery - Specific Considerations - Schwartz's Principles of Surgery ABSITE and Board Review, 9th Edvnnv101.raceacNo ratings yet
- Pediatric Department Book Part 2 (2019-2020)Document236 pagesPediatric Department Book Part 2 (2019-2020)Mohammed ArarNo ratings yet
- Anatomy PDFDocument114 pagesAnatomy PDFkhualabear101100% (1)
- Ingles Parcial Domiciliario 2022Document5 pagesIngles Parcial Domiciliario 2022Macarena zapattaNo ratings yet
- Neurological System Questions Part 2Document35 pagesNeurological System Questions Part 2luna nguyenNo ratings yet
- Case Presentation About Spinal Shock SyndromeDocument56 pagesCase Presentation About Spinal Shock SyndromeAstral_edge010100% (1)
- Brain Anatomy ThesisDocument4 pagesBrain Anatomy Thesisbrittanyjonescolumbia100% (2)
- Dwnload Full Foundations of Psychiatric Mental Health Nursing A Clinical Approach 6th Edition Varcarolis Test Bank PDFDocument36 pagesDwnload Full Foundations of Psychiatric Mental Health Nursing A Clinical Approach 6th Edition Varcarolis Test Bank PDFscarletdrusillaplwrd100% (11)
- Neuromuscular and Nervous System 2010 With AnswersDocument13 pagesNeuromuscular and Nervous System 2010 With AnswersWenzy CruzNo ratings yet
- Case StudyDocument40 pagesCase StudySheryhan BayleNo ratings yet
- Brain 2009 Barkovich 3199 230 Neuroembyology1Document32 pagesBrain 2009 Barkovich 3199 230 Neuroembyology1Azalia BahatNo ratings yet
- Term Paper Nervous SystemDocument6 pagesTerm Paper Nervous Systemaflsmyebk100% (1)
- Neuroscience Thesis CarletonDocument8 pagesNeuroscience Thesis Carletonfjn3d3mc100% (2)
- Neurocriticalcareresearch: Collaborations For Curing ComaDocument8 pagesNeurocriticalcareresearch: Collaborations For Curing ComaJonathan Mendoza V.No ratings yet
- CVD Case StudyDocument12 pagesCVD Case StudySean MercadoNo ratings yet
- Full Download Test Bank For Neuroscience Fundamentals For Rehabilitation 4th Edition by Lundy Ekman PDF Full ChapterDocument36 pagesFull Download Test Bank For Neuroscience Fundamentals For Rehabilitation 4th Edition by Lundy Ekman PDF Full Chapterzeugmapaidcbur100% (22)
- Full Test Bank For Neuroscience Fundamentals For Rehabilitation 4Th Edition by Lundy Ekman PDF Docx Full Chapter ChapterDocument36 pagesFull Test Bank For Neuroscience Fundamentals For Rehabilitation 4Th Edition by Lundy Ekman PDF Docx Full Chapter Chapterplaudittaborine.pqowz100% (8)
- Test Bank For Neuroscience Fundamentals For Rehabilitation 4th Edition by Lundy EkmanDocument7 pagesTest Bank For Neuroscience Fundamentals For Rehabilitation 4th Edition by Lundy Ekmaneirlysphoebe0qf67No ratings yet
- Research Paper Central Nervous SystemDocument5 pagesResearch Paper Central Nervous Systemlzpyreqhf100% (1)
- Cerebral Palsy and Congenital Malformations: Review ArticleDocument7 pagesCerebral Palsy and Congenital Malformations: Review ArticleC_DanteNo ratings yet
- DRSTMH MS WardDocument73 pagesDRSTMH MS WardClark LlameraNo ratings yet
- CVA Case ReportDocument76 pagesCVA Case ReportpaulaNo ratings yet
- JurnalDocument5 pagesJurnalAnonymous 65zjdAVNo ratings yet
- Neuromuscular 2 2010 With AnswersDocument13 pagesNeuromuscular 2 2010 With AnswersWenzy CruzNo ratings yet
- Ultrasound-Guided Nerve Blocks in The Head and Neck For Chronic Pain Management - The Anatomy, Sonoanatomy, and ProcedureDocument16 pagesUltrasound-Guided Nerve Blocks in The Head and Neck For Chronic Pain Management - The Anatomy, Sonoanatomy, and Proceduremarcus moraisNo ratings yet
- Caring For The Patient With Cerebrovascular Disease Super FinalDocument84 pagesCaring For The Patient With Cerebrovascular Disease Super FinalDexter Niel Ortilano CPAC-SNNo ratings yet
- A Ann CraniotomyDocument41 pagesA Ann CraniotomyF̳̿a̳̿l̳̿a̳̿h̳̿ Opcional S̳̿u̳̿d̳̿i̳̿r̳̿a̳̿d̳̿i̳̿r̳̿e̳̿j̳̿a̳̿No ratings yet
- Dwnload Full Varcarolis Foundations of Psychiatric Mental Nursing 8th Edition Margaret Test Bank PDFDocument36 pagesDwnload Full Varcarolis Foundations of Psychiatric Mental Nursing 8th Edition Margaret Test Bank PDFrapper.clearjyz53j100% (7)
- Pediatric Forensic Pathology: Limits and ControversiesDocument191 pagesPediatric Forensic Pathology: Limits and Controversieschrisr310No ratings yet
- Aps 100Document5 pagesAps 100Omair marohomNo ratings yet
- Basic Neuroanatomy and Stroke Syndromes PDFDocument15 pagesBasic Neuroanatomy and Stroke Syndromes PDFFrancisco A. Villegas-López100% (2)
- Neuro Study GuideDocument11 pagesNeuro Study GuideEllen Hennings100% (1)
- CASE STUDY - Cerebral ContusionDocument20 pagesCASE STUDY - Cerebral Contusionleyach80% (5)
- BRT Anatomy - NeuroanatomyDocument6 pagesBRT Anatomy - NeuroanatomyNicole Santos100% (3)
- Case Study TbiDocument13 pagesCase Study Tbiaica_184No ratings yet
- Acute HypoxiaDocument6 pagesAcute HypoxiaKarmeen HumaNo ratings yet
- TG Case 1 - Congenital 2012Document17 pagesTG Case 1 - Congenital 2012Galih Nadhova Imana LiverpudlianNo ratings yet
- The Brachial Plexus PDFDocument2 pagesThe Brachial Plexus PDFmandalaNo ratings yet
- BARKOVICH Pediatric Neuroimaging 5Document1,145 pagesBARKOVICH Pediatric Neuroimaging 5Pepe ArsNo ratings yet
- Evidence-Based NursingDocument9 pagesEvidence-Based NursingKate AbadNo ratings yet
- Histology of Cns and Pns Wayan Sugiritama Learning Tasks Trigger Case 1Document1 pageHistology of Cns and Pns Wayan Sugiritama Learning Tasks Trigger Case 1Kristian Dwi CahyaNo ratings yet
- Alwahab2017 Article OccipitalMeningoencephaloceleC PDFDocument4 pagesAlwahab2017 Article OccipitalMeningoencephaloceleC PDFOvamelia JulioNo ratings yet
- World's Largest Science, Technology & Medicine Open Access Book PublisherDocument14 pagesWorld's Largest Science, Technology & Medicine Open Access Book PublisherAnnamaria GyőrfiNo ratings yet
- 3ftfbsdi "Sujdmf $pnqbsjtpo PG) JQQPDBNQBM 7Pmvnf Jo %fnfoujb 4vcuzqftDocument5 pages3ftfbsdi "Sujdmf $pnqbsjtpo PG) JQQPDBNQBM 7Pmvnf Jo %fnfoujb 4vcuzqftabhishekbmcNo ratings yet
- Usmle 1Document36 pagesUsmle 1Suruchi Jagdish SharmaNo ratings yet
- Atlas of The Human Body Central Nervous System and Vascularization Branislav Vidic Full ChapterDocument51 pagesAtlas of The Human Body Central Nervous System and Vascularization Branislav Vidic Full Chapteralisha.deane126100% (5)
- Neurosurgery: A Case-Based Approach Christos M. Tolias Anastasios Giamouriadis Florence Rosie Avila Hogg Prajwal GhimireDocument225 pagesNeurosurgery: A Case-Based Approach Christos M. Tolias Anastasios Giamouriadis Florence Rosie Avila Hogg Prajwal GhimireMystero Rasico100% (1)
- Musawi 35Document22 pagesMusawi 35Full MarksNo ratings yet
- Stroke DissertationDocument6 pagesStroke DissertationProfessionalPaperWriterPortland100% (1)
- Malnutrition SurgeryDocument18 pagesMalnutrition SurgerysamrusangaliNo ratings yet
- Meterology DaigrmsDocument13 pagesMeterology DaigrmssamrusangaliNo ratings yet
- Solid Waste Management:: 11. Draw Diff Type A) Bore Hole B) Dug Well C) Septic Tank D) Trench Type E) Pit LatrineDocument2 pagesSolid Waste Management:: 11. Draw Diff Type A) Bore Hole B) Dug Well C) Septic Tank D) Trench Type E) Pit LatrinesamrusangaliNo ratings yet
- Waste Water ManagementDocument13 pagesWaste Water ManagementsamrusangaliNo ratings yet
- Myofascial and Endodontics. 2022Document15 pagesMyofascial and Endodontics. 2022David MonroyNo ratings yet
- Safety Profile of Rotavac: Observational Prospective StudyDocument7 pagesSafety Profile of Rotavac: Observational Prospective StudyMalook Sekhon100% (1)
- Implementation of New Safety Protocols of Calle Arco Restaurant in Pagsanjan, Laguna During Pandemic CrisisDocument42 pagesImplementation of New Safety Protocols of Calle Arco Restaurant in Pagsanjan, Laguna During Pandemic CrisisOliveros John Brian R.No ratings yet
- Downer Cow Syndrome, Creeper Cows.Document8 pagesDowner Cow Syndrome, Creeper Cows.Ali H. Sadiek أ.د. علي حسن صديق100% (1)
- Erythrocytic Indices and Their Significance Final-1Document22 pagesErythrocytic Indices and Their Significance Final-1Asad ullahNo ratings yet
- Nclex Questions For Fundamentals of NursDocument32 pagesNclex Questions For Fundamentals of NursJrBong SemaneroNo ratings yet
- Hypoxia: Name: Abdalaziz Mostafa No: 1176Document14 pagesHypoxia: Name: Abdalaziz Mostafa No: 11763omar18No ratings yet
- Seminar: Christian Trépo, Henry L Y Chan, Anna LokDocument11 pagesSeminar: Christian Trépo, Henry L Y Chan, Anna LokGERALDINE JARAMILLO VARGASNo ratings yet
- SGOT (Aspartate Aminotransferase, AST, Glutamic Oxaloacetic Transaminase)Document9 pagesSGOT (Aspartate Aminotransferase, AST, Glutamic Oxaloacetic Transaminase)Reman A. AlingasaNo ratings yet
- Angina PectorisDocument4 pagesAngina PectorisJohiarra Madanglog TabigneNo ratings yet
- Hannover Polytrauma Score.4Document2 pagesHannover Polytrauma Score.4Azmi FarhadiNo ratings yet
- Endodontics Principles and Practice (139 279)Document141 pagesEndodontics Principles and Practice (139 279)Daniel Ricardo Moreno HernandezNo ratings yet
- 2022 Safe Motherhood and Newborn Health Communication PlanDocument4 pages2022 Safe Motherhood and Newborn Health Communication PlanZenard de la CruzNo ratings yet
- Anatomy and Physiology of The EyeDocument22 pagesAnatomy and Physiology of The EyeBalkos 61No ratings yet
- 10 Penyakit Terbanyak Di Rawat Jalan Di Puskesmas Provinsi Dki Jakarta TW I Tahun 2019Document9 pages10 Penyakit Terbanyak Di Rawat Jalan Di Puskesmas Provinsi Dki Jakarta TW I Tahun 2019Klinik pratama Iqra' medical centreNo ratings yet
- Deped Question SurveyDocument3 pagesDeped Question SurveyFCI Isabela SHS100% (1)
- 978-3-030-84134-8 - COVID-19 and CitiesDocument337 pages978-3-030-84134-8 - COVID-19 and CitiesJose Ferreira PintoNo ratings yet
- Shibari - Japanese Bondage Techniques - Learn The Most Popular Japanese Art of SeductionDocument57 pagesShibari - Japanese Bondage Techniques - Learn The Most Popular Japanese Art of SeductionFrancisco MartinezNo ratings yet
- Calamansi and Lemongrass As Alternative Mosquito Coil: Submitted By: Kristhel Nieves N. Zamora 10-AmethystDocument6 pagesCalamansi and Lemongrass As Alternative Mosquito Coil: Submitted By: Kristhel Nieves N. Zamora 10-AmethystKristhel ZamoraNo ratings yet
- Genetics Notes - Other Patterns of Inheritance & PedigreesDocument4 pagesGenetics Notes - Other Patterns of Inheritance & PedigreesJoseph Dav6657No ratings yet
- THYROIDINIUMDocument13 pagesTHYROIDINIUMUnnathi TNo ratings yet
- Menstrual - Disorders 2Document24 pagesMenstrual - Disorders 2Abdibaset Mohamed AdenNo ratings yet
- Research Paper On Recombinant Dna TechnologyDocument7 pagesResearch Paper On Recombinant Dna Technologyvagipelez1z2100% (1)
- Chapter 8. Cholinoceptor Blockers & Amp Cholinesterase RegeneratorsDocument8 pagesChapter 8. Cholinoceptor Blockers & Amp Cholinesterase RegeneratorsChrysler Hans GuttenbergNo ratings yet
- Activity Intolerance NCPDocument7 pagesActivity Intolerance NCPamitNo ratings yet
- Soal Ujian SekolahDocument47 pagesSoal Ujian SekolahClemens JasonNo ratings yet
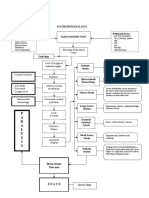
- Pathophysiology: P A R A L Y S I SDocument1 pagePathophysiology: P A R A L Y S I SJordan Garcia AguilarNo ratings yet
- Lec 7 Cardiac RehabilitationDocument53 pagesLec 7 Cardiac RehabilitationSaeed SaeedNo ratings yet