You might also like
- ECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasFrom EverandECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasRating: 5 out of 5 stars5/5 (2)
- Defibrillatorppt 131028115457 Phpapp01Document41 pagesDefibrillatorppt 131028115457 Phpapp01Qweku BlackNo ratings yet
- Ecg 111029102429 Phpapp01Document103 pagesEcg 111029102429 Phpapp01Vickry WahidjiNo ratings yet
- Ecg Treadmill and Holter TestDocument77 pagesEcg Treadmill and Holter TestRiteka Singh100% (1)
- Beta BlockersDocument70 pagesBeta BlockersIrina Cabac-PogoreviciNo ratings yet
- Basics of Ecg InterpretationDocument76 pagesBasics of Ecg InterpretationDennis MiritiNo ratings yet
- Disorders of The EyeDocument15 pagesDisorders of The EyeVinz Khyl G. Castillon100% (2)
- (Medicalstudyzone - Com) NBME 25 Answers VersionDocument200 pages(Medicalstudyzone - Com) NBME 25 Answers VersionMahnoor Tauqeer100% (1)
- Fundamentals of ECGDocument112 pagesFundamentals of ECGadithya polavarapu100% (1)
- Defibrillation and Electrical CardioversionDocument27 pagesDefibrillation and Electrical CardioversionYui Hirasawa100% (1)
- Nutritional Assessment StagesDocument6 pagesNutritional Assessment StagesVinz Khyl G. CastillonNo ratings yet
- Podrid's Real-World ECGs Volume 6 (2016) PDFDocument635 pagesPodrid's Real-World ECGs Volume 6 (2016) PDFRyan Kadavil100% (2)
- Electro Cardiogram: NCM 112:skills LaboratoryDocument7 pagesElectro Cardiogram: NCM 112:skills LaboratoryFaye Domini FederisNo ratings yet
- Electrical TimeDocument14 pagesElectrical TimeNithyaa SathishNo ratings yet
- Dec Cardiac Output NCPDocument2 pagesDec Cardiac Output NCPJoehoney BarreraNo ratings yet
- Electrocardiogram Nursing ResponsibilitiesDocument28 pagesElectrocardiogram Nursing ResponsibilitiesKristine Jade Rojas100% (1)
- 418RLE M2 SL1 Basic ECGDocument8 pages418RLE M2 SL1 Basic ECGCamille Neypes CarreraNo ratings yet
- Cardiovascular System NotesDocument43 pagesCardiovascular System Notestruefriends0809No ratings yet
- EKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationFrom EverandEKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationRating: 3 out of 5 stars3/5 (1)
- Cardiac MonitoringDocument5 pagesCardiac MonitoringAmit Kl100% (1)
- Cardiac MonitorDocument5 pagesCardiac MonitorhumbertolgeNo ratings yet
- Presented By-: ElectrocardiographyDocument18 pagesPresented By-: ElectrocardiographyArnab Guin100% (1)
- Introduction To ECG For NursingDocument75 pagesIntroduction To ECG For NursingRashid AlHamdan100% (1)
- Salbutamol Drug StudyDocument2 pagesSalbutamol Drug StudyVinz Khyl G. CastillonNo ratings yet
- 2022 Non-Cardiac SurgeryDocument105 pages2022 Non-Cardiac Surgeryhosameldin ahmedNo ratings yet
- Controlled Hypotension: Moderator: DR V. Y. Srinivas Presenter: Dr. Ann Susan MathewDocument49 pagesControlled Hypotension: Moderator: DR V. Y. Srinivas Presenter: Dr. Ann Susan MathewAnn Susan MathewNo ratings yet
- Rutherford Vascular Surgery 6th Edition Elsevier SDocument2 pagesRutherford Vascular Surgery 6th Edition Elsevier SJennifer Jane0% (1)
- EcgDocument45 pagesEcgkamel6No ratings yet
- Topic:: Performing and Interpreting Electrocardiogram (ECG)Document137 pagesTopic:: Performing and Interpreting Electrocardiogram (ECG)Tiffany AdriasNo ratings yet
- ECG Placement Final DLSL - DDocument44 pagesECG Placement Final DLSL - DAlma Janella TOSINONo ratings yet
- DEB 221 Electro Medical Devices SENT 4 02 2020Document20 pagesDEB 221 Electro Medical Devices SENT 4 02 2020Ocwich FrancisNo ratings yet
- Demonstration On EcgDocument15 pagesDemonstration On EcgShafna SirajNo ratings yet
- ECGfinalDocument10 pagesECGfinalSarah FerguzonNo ratings yet
- ECGDocument62 pagesECGSanju TanwarNo ratings yet
- Basic ElectrophysiologyDocument18 pagesBasic ElectrophysiologyCarlo Domingo LadieroNo ratings yet
- Electrocardiography Is The Most Commonly Used Test For EvaluatingDocument5 pagesElectrocardiography Is The Most Commonly Used Test For Evaluatingmyk_1102No ratings yet
- The Wiring Diagram of The HeartDocument4 pagesThe Wiring Diagram of The Heartgurneet kourNo ratings yet
- Basic Electrocardiogram (Ecg) : Mr. Hamza Ratrout Revised By: Dr. Irene RocoDocument28 pagesBasic Electrocardiogram (Ecg) : Mr. Hamza Ratrout Revised By: Dr. Irene Rocoأبوأحمد الحكيمNo ratings yet
- DefibrillatorDocument8 pagesDefibrillatorJisha JanardhanNo ratings yet
- 12 Lead Ecg PlacementsDocument9 pages12 Lead Ecg Placementskim reyesNo ratings yet
- 12 Lead Ecg Placements The HeartDocument9 pages12 Lead Ecg Placements The HeartFalusi Blessing OlaideNo ratings yet
- ECG Monitor and RhythmDocument9 pagesECG Monitor and Rhythmboxed juiceNo ratings yet
- Detailed Cen01 2019Document13 pagesDetailed Cen01 2019ChanNo ratings yet
- ElectrocardiogramDocument17 pagesElectrocardiogramvinnu kalyanNo ratings yet
- Electro PhysiologyDocument108 pagesElectro PhysiologyGUTIERREZ, CRISHA ANDREA M.No ratings yet
- Ecg or Electro Cardiogram and ElectrocardiographDocument20 pagesEcg or Electro Cardiogram and ElectrocardiographsureshNo ratings yet
- Electrocardiogram12 LeadsDocument28 pagesElectrocardiogram12 LeadsshyluckmayddpNo ratings yet
- Ecg + Ventricular Tachycardia and FibrillationDocument9 pagesEcg + Ventricular Tachycardia and Fibrillationsakkiyy154No ratings yet
- Electrocardiogram (EKG or ECG)Document12 pagesElectrocardiogram (EKG or ECG)श्रीकृष्ण हेङ्गजूNo ratings yet
- The CardiacDocument7 pagesThe CardiacCake ManNo ratings yet
- Major Project Phase 1 Report CloudDocument35 pagesMajor Project Phase 1 Report CloudPraj CNo ratings yet
- 418rle m2 Sl1+Basic+EcgDocument8 pages418rle m2 Sl1+Basic+EcgPaul SahagunNo ratings yet
- Biomedical Instrumentation (BM8502)Document34 pagesBiomedical Instrumentation (BM8502)1011 BMENo ratings yet
- Ecg PrsentationDocument33 pagesEcg Prsentationtehillahkabwe100No ratings yet
- NMTEC 211-ECG Lab InstructionsDocument4 pagesNMTEC 211-ECG Lab InstructionsRisleNo ratings yet
- Nursing Journal EcgDocument2 pagesNursing Journal EcgCharlene Jacobe CornistaNo ratings yet
- Pratik PPT Registration SeminarDocument45 pagesPratik PPT Registration SeminarPratik SinghNo ratings yet
- Ecg 1Document198 pagesEcg 1hibaNo ratings yet
- 1621324573PHYSIOLOGY, SEM-2 - K-Sembulingam-Essentials-Of-Medical-PhysiologyDocument7 pages1621324573PHYSIOLOGY, SEM-2 - K-Sembulingam-Essentials-Of-Medical-PhysiologyAyoola BolajiNo ratings yet
- Practical 2: Electrocardiogram (Ecg/Ekg) : by - Mohamad Azmir Bin Azizan Medical Lab Technologist Faculty of Medicine UitmDocument19 pagesPractical 2: Electrocardiogram (Ecg/Ekg) : by - Mohamad Azmir Bin Azizan Medical Lab Technologist Faculty of Medicine UitmraburtonNo ratings yet
- Electrocardiography: An Introduction To The ECGDocument76 pagesElectrocardiography: An Introduction To The ECGInnocent Clifford MaranduNo ratings yet
- IV A Ecg Preparation 12 Lead Placements NCM 118 Nursing Care of Clients With Life Threatening CondDocument13 pagesIV A Ecg Preparation 12 Lead Placements NCM 118 Nursing Care of Clients With Life Threatening CondRio DanteNo ratings yet
- A Guide TO: Noob'SDocument103 pagesA Guide TO: Noob'SAgleema AhmedNo ratings yet
- ECG and XRAYDocument47 pagesECG and XRAYSwaroop KumarNo ratings yet
- Ecg FinalDocument61 pagesEcg Finalmahes2011No ratings yet
- Modern Electronic InstrumentsDocument7 pagesModern Electronic InstrumentsuatilakarathnaNo ratings yet
- ElectrocardiographyDocument4 pagesElectrocardiographyJho BuanNo ratings yet
- 12 Lead Electrocardiogram (Ecg) Placement: Module DescriptionDocument11 pages12 Lead Electrocardiogram (Ecg) Placement: Module DescriptionHanna La MadridNo ratings yet
- Unit 2 BmiDocument188 pagesUnit 2 Bmiaarthir88No ratings yet
- Bio SignalDocument20 pagesBio SignalThiyagu RajanNo ratings yet
- Decoding Cardiac Electrophysiology: Understanding the Techniques and Defining the JargonFrom EverandDecoding Cardiac Electrophysiology: Understanding the Techniques and Defining the JargonAfzal SohaibNo ratings yet
- WEEK 7 8 STS and The Human Condition Part 1 1Document30 pagesWEEK 7 8 STS and The Human Condition Part 1 1Vinz Khyl G. CastillonNo ratings yet
- STS Module Week 7 8 ST and The Human FlourishingDocument8 pagesSTS Module Week 7 8 ST and The Human FlourishingVinz Khyl G. CastillonNo ratings yet
- NQS - August2020 (Phase2) - FinalDocument5 pagesNQS - August2020 (Phase2) - FinalVinz Khyl G. CastillonNo ratings yet
- Disorders of The EarDocument8 pagesDisorders of The EarVinz Khyl G. CastillonNo ratings yet
- Indwelling Urinary Catheter FemaleDocument9 pagesIndwelling Urinary Catheter FemaleVinz Khyl G. CastillonNo ratings yet
- Reflection RubricDocument1 pageReflection RubricVinz Khyl G. CastillonNo ratings yet
- Gone Girl Monologue Amy PDFDocument2 pagesGone Girl Monologue Amy PDFVinz Khyl G. CastillonNo ratings yet
- Phenylephrine Hydrochloride PDFDocument5 pagesPhenylephrine Hydrochloride PDFVinz Khyl G. CastillonNo ratings yet
- Concept MapDocument2 pagesConcept MapVinz Khyl G. CastillonNo ratings yet
- The Growing Fetus During The Second TrimesterDocument5 pagesThe Growing Fetus During The Second TrimesterVinz Khyl G. CastillonNo ratings yet
- Howell, Martha and Walter PrevenierDocument1 pageHowell, Martha and Walter PrevenierVinz Khyl G. CastillonNo ratings yet
- English 7 NC Timetable THF 10:30 Date Lessons/Tasks/ActivitiesDocument2 pagesEnglish 7 NC Timetable THF 10:30 Date Lessons/Tasks/ActivitiesVinz Khyl G. CastillonNo ratings yet
- Pediatric Nursing. PPDocument4 pagesPediatric Nursing. PPVinz Khyl G. CastillonNo ratings yet
- Bioassay of DigitalisDocument11 pagesBioassay of DigitalisMasum Billa MollaNo ratings yet
- ECG Criterias For Ventricular Hypertrophy by DR PRASANTH SDocument13 pagesECG Criterias For Ventricular Hypertrophy by DR PRASANTH SnadineNo ratings yet
- iPM Operator's Manual - V12.0 - EN PDFDocument318 pagesiPM Operator's Manual - V12.0 - EN PDFmarceNo ratings yet
- Noise Pollution FlyerDocument2 pagesNoise Pollution FlyerShannon RaspNo ratings yet
- Anestesia Consideraciones de Anesthesia en Paciente Geratricos PDFDocument3 pagesAnestesia Consideraciones de Anesthesia en Paciente Geratricos PDFFernanda PérezNo ratings yet
- Class 7 Holiday Homework-MergedDocument29 pagesClass 7 Holiday Homework-MergedidkNo ratings yet
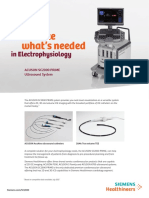
- Siemens Acuson Sc2000 Ep Flyer v2Document4 pagesSiemens Acuson Sc2000 Ep Flyer v2bashir019No ratings yet
- Clinical Exam RequirementDocument7 pagesClinical Exam Requirementyb5fdt8cp7No ratings yet
- 12 Lead Electrocardiogram (Ecg) Placement: Module DescriptionDocument11 pages12 Lead Electrocardiogram (Ecg) Placement: Module DescriptionHanna La MadridNo ratings yet
- CARVEDILOL Nursing ImplicationsDocument2 pagesCARVEDILOL Nursing Implicationsshiraz.aNo ratings yet
- Updates in Vascular Computed TomographyDocument21 pagesUpdates in Vascular Computed TomographyHector Hernandez-SoriaNo ratings yet
- Cardiovascular Disorders: Coronary AtherosclerosisDocument6 pagesCardiovascular Disorders: Coronary AtherosclerosisHazel BandayNo ratings yet
- ASSIST Magazine Image Based FFR With QFRDocument9 pagesASSIST Magazine Image Based FFR With QFRAsim AliNo ratings yet
- Aortic Dissection AtfDocument8 pagesAortic Dissection AtfAmir mohammad moori MohammadiNo ratings yet
- Cardiac Auscultation 3696Document2 pagesCardiac Auscultation 3696nutype01No ratings yet
- J Strength Cond Res - 2011 - A Comparison of The Immediate Effects of Resistance, Aerobic, and Concurrent Exercise On Postexercise HypotensionDocument8 pagesJ Strength Cond Res - 2011 - A Comparison of The Immediate Effects of Resistance, Aerobic, and Concurrent Exercise On Postexercise HypotensionTAINAH DE PAULANo ratings yet
- Eco DopplerDocument8 pagesEco DopplerClaudia IsabelNo ratings yet
- 1 Ame-Feno TrainingDocument12 pages1 Ame-Feno TrainingThet Su LwinNo ratings yet
- CV PharmaDocument2 pagesCV PharmaAnshulNo ratings yet
- IAL - Bio - SB2 - Teaching Plans - 7BDocument29 pagesIAL - Bio - SB2 - Teaching Plans - 7BsalmaNo ratings yet
- Tetraogy of FallotDocument9 pagesTetraogy of FallotMary Louise MadariagaNo ratings yet
- Basic Principles of Platelet Biology and Clinical ImplicationsDocument11 pagesBasic Principles of Platelet Biology and Clinical ImplicationsIsmael Rivera DiazNo ratings yet