You might also like
- MSK AllDocument113 pagesMSK AllMuhammed Elgasim100% (1)
- Red Flag: MSK Services Pathway - Hand PathologyDocument10 pagesRed Flag: MSK Services Pathway - Hand PathologyMuhammed ElgasimNo ratings yet
- Histopathology - Biopsy and AutopsyDocument14 pagesHistopathology - Biopsy and AutopsyTricia Claire Uy100% (1)
- Pilot Learn English Now Eng0343Document18 pagesPilot Learn English Now Eng0343pedro.muneerNo ratings yet
- Red Flag: MSK Services Pathway - Elbow PathologyDocument7 pagesRed Flag: MSK Services Pathway - Elbow PathologyMuhammed ElgasimNo ratings yet
- Approach To Polyarthritis For The Primary Care Physician: Arielle Freilich, DO, PGY2 & Helaine Larsen, DODocument8 pagesApproach To Polyarthritis For The Primary Care Physician: Arielle Freilich, DO, PGY2 & Helaine Larsen, DOLydia IsaacNo ratings yet
- Report For Oil ProcessingDocument83 pagesReport For Oil ProcessingabhayNo ratings yet
- Perioperative Pain ManagementFrom EverandPerioperative Pain ManagementFelicia CoxNo ratings yet
- Schofield1998 - The Mohr-Coulomb Error CorrectionDocument3 pagesSchofield1998 - The Mohr-Coulomb Error CorrectionandresmelodNo ratings yet
- Cyriax - Spine: by DR. Akshay A. Chougule (PT) Orthopaedic Manual TherapistDocument44 pagesCyriax - Spine: by DR. Akshay A. Chougule (PT) Orthopaedic Manual TherapistAishwarya Shah100% (1)
- Rheumatology: - Red Flag DiagnosisDocument3 pagesRheumatology: - Red Flag DiagnosisEmilee Joice Rochelle MalutoNo ratings yet
- 2y2s (Surgery) - The Abdomen PrintablesDocument9 pages2y2s (Surgery) - The Abdomen PrintablesCarmela MarianoNo ratings yet
- Approach To A Patient With PolyarthritisDocument29 pagesApproach To A Patient With PolyarthritisMd ImamuddinNo ratings yet
- Pain Dr. HenryDocument36 pagesPain Dr. Henryreagan setiawanNo ratings yet
- Anterior Uveitis: Ophthalmology Management TreeDocument2 pagesAnterior Uveitis: Ophthalmology Management TreeSandro PandurevicNo ratings yet
- Lidocaine Ferrous SulfateDocument6 pagesLidocaine Ferrous SulfateBrainard J OmanitoNo ratings yet
- P.05 Pain in The Extremities (Dr. Dominguez) (09-10-18)Document13 pagesP.05 Pain in The Extremities (Dr. Dominguez) (09-10-18)Raymund Dan AldabaNo ratings yet
- Arthritis AlgorithmDocument1 pageArthritis Algorithmaniqahmed6565No ratings yet
- Pedia RheumatologyDocument13 pagesPedia RheumatologyJuda Zhēn ZhūNo ratings yet
- Rachialgia 31 - 01Document4 pagesRachialgia 31 - 01Nathaly MoraNo ratings yet
- Week 13 Inflammatory Ncma219 Lec Finals ReviewerDocument4 pagesWeek 13 Inflammatory Ncma219 Lec Finals ReviewerWynahNo ratings yet
- HP Lec - Biopsy and AutopsyDocument7 pagesHP Lec - Biopsy and AutopsyAaron Vincent MillomedaNo ratings yet
- DR Natsir SPPD KR Painful JointDocument41 pagesDR Natsir SPPD KR Painful JointSITI BINTA MASYKURINNo ratings yet
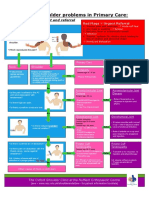
- NHS UK Diagnosis of Shoulder ProblemsDocument1 pageNHS UK Diagnosis of Shoulder ProblemsmertNo ratings yet
- ERPM Medicine Theory Session 2 TutesDocument88 pagesERPM Medicine Theory Session 2 TutesRoHIT ShowNo ratings yet
- Nyeri Dan TatalaksananyaDocument61 pagesNyeri Dan TatalaksananyaTatyana SianiparNo ratings yet
- ORTHOPEDIC PT 2 (Postlec #3) Arthritic & Connective Tissue DiseasesDocument5 pagesORTHOPEDIC PT 2 (Postlec #3) Arthritic & Connective Tissue DiseasesJastine AbigaileNo ratings yet
- Hand and Wrist PathwayDocument2 pagesHand and Wrist PathwaydrsadafrafiNo ratings yet
- Pain Assessment & Oxygen SaturationDocument4 pagesPain Assessment & Oxygen SaturationKathrine Isabelle CuevasNo ratings yet
- EAU Guidelines On Sexual and Reproductive Health 2022 - 2022 03 29 084141 - Megw (110 111)Document2 pagesEAU Guidelines On Sexual and Reproductive Health 2022 - 2022 03 29 084141 - Megw (110 111)CRISTH KIMBERLY ENEQUE DE LA CRUZNo ratings yet
- Prelims - MS RleDocument22 pagesPrelims - MS RlearianeandreaherreraNo ratings yet
- Reviewer in Physical Agents and Electrotherapy: Pagod Na Di Alam Kung BaketDocument8 pagesReviewer in Physical Agents and Electrotherapy: Pagod Na Di Alam Kung Baketrr4fgws945No ratings yet
- Drug Study - MONTELUKASTDocument3 pagesDrug Study - MONTELUKASTCHRISTINE GRACE ELLONo ratings yet
- Migraine and Tension Headache: Diagnosis and Treatment GuidelineDocument16 pagesMigraine and Tension Headache: Diagnosis and Treatment GuidelinecynthiaramaNo ratings yet
- Modalitas Tatalaksana Rehab MedikDocument6 pagesModalitas Tatalaksana Rehab Medikone dNo ratings yet
- M2 PPT Treating PainDocument44 pagesM2 PPT Treating PainMeena CtNo ratings yet
- Approach To Case of ArthritisDocument53 pagesApproach To Case of ArthritisdrsarathmenonNo ratings yet
- ORTHOPEDIC PT 2 (Prelec #3) Arthritic & Connective Tissue DiseasesDocument2 pagesORTHOPEDIC PT 2 (Prelec #3) Arthritic & Connective Tissue DiseasesJastine AbigaileNo ratings yet
- High Velocity Manipulation TechniquesDocument2 pagesHigh Velocity Manipulation TechniquesBhargavaNo ratings yet
- Focused ReviewDocument6 pagesFocused ReviewGina GiammalvoNo ratings yet
- Med BackDocument41 pagesMed BackKyle OrtegaNo ratings yet
- NCP - Imbalanced Nutrition - de Guzman, Gadia, Lacanilao, VergaraDocument4 pagesNCP - Imbalanced Nutrition - de Guzman, Gadia, Lacanilao, VergaraLuis Gatchalian LacanilaoNo ratings yet
- Red Flags: Indications For Urgent ReferralDocument5 pagesRed Flags: Indications For Urgent ReferralEndah Novianti SoenarsinNo ratings yet
- Approach To Joint Pain (October 2022)Document56 pagesApproach To Joint Pain (October 2022)imranmohammad968No ratings yet
- Evangelista Pagola Case StudyDocument21 pagesEvangelista Pagola Case StudyMikes CastroNo ratings yet
- NCM 112 (11F)Document15 pagesNCM 112 (11F)Justine April YbanezNo ratings yet
- 01 Cell Adaptations, Cell Injury, Cell DeathDocument7 pages01 Cell Adaptations, Cell Injury, Cell DeathcarlgangcaNo ratings yet
- Drug StudyDocument12 pagesDrug StudyJae TyNo ratings yet
- Acute Limb Compartment Syndrome: Observation ChartDocument2 pagesAcute Limb Compartment Syndrome: Observation CharttioNo ratings yet
- Musculoskeletal Trauma RSIJPKDocument41 pagesMusculoskeletal Trauma RSIJPKPegyNo ratings yet
- DR Adrian Jones - Seronegative SpondyloarthropathiesDocument38 pagesDR Adrian Jones - Seronegative SpondyloarthropathiesMaryam ShahbazNo ratings yet
- 1 3-ArthritisDocument9 pages1 3-ArthritisRohit kumar Saravana kumarNo ratings yet
- EMRGI 2 - RheumatologyDocument11 pagesEMRGI 2 - RheumatologyCindy CabrerosNo ratings yet
- Palliative Care Distressing Symptoms PainDocument36 pagesPalliative Care Distressing Symptoms PainskuahoNo ratings yet
- ProActive Training CaseStudy 5Document8 pagesProActive Training CaseStudy 5danthemanyvrNo ratings yet
- Pain Management - Prelim Notes - Clin Phar 1Document8 pagesPain Management - Prelim Notes - Clin Phar 1Jan Elishah Camarador AllareyNo ratings yet
- Pedia SeizuresDocument2 pagesPedia SeizuresZhantelle A. SantosNo ratings yet
- Case: Renal and Genitourinary Block Week 3 General DataDocument19 pagesCase: Renal and Genitourinary Block Week 3 General DataEveryday FundayNo ratings yet
- (2009) Gout PDFDocument11 pages(2009) Gout PDFWilsonne ChuaNo ratings yet
- Pathway For Shoulder PainDocument1 pagePathway For Shoulder Painrizk86No ratings yet
- Crps AlgorhythmDocument4 pagesCrps AlgorhythmroboNo ratings yet
- Hand and Wrist DisordersDocument25 pagesHand and Wrist Disorders202003339No ratings yet
- Kuliah 02 - Pengolahan Citra Digital Sampling Quantization 2Document18 pagesKuliah 02 - Pengolahan Citra Digital Sampling Quantization 2Zulkifli Nagh BalitanNo ratings yet
- The Marine WorkoutDocument7 pagesThe Marine WorkoutAndres Eco AldeanoNo ratings yet
- OD329422999281816100Document1 pageOD329422999281816100sanjeev kumarNo ratings yet
- Manual Safety SignDocument49 pagesManual Safety SignMuamar DhikriNo ratings yet
- Semantic Analysis of The Verbal Phraseological Units On The Examples in The German, English and Karakalpak LanguagesDocument3 pagesSemantic Analysis of The Verbal Phraseological Units On The Examples in The German, English and Karakalpak LanguagesEditor IJTSRDNo ratings yet
- Sky SurfingDocument10 pagesSky SurfingCamila Soledad Aguilera PizarroNo ratings yet
- Latihan SoalDocument7 pagesLatihan SoaljuliaNo ratings yet
- Critical Thinking and EBPDocument31 pagesCritical Thinking and EBPEni SukmawatiNo ratings yet
- Vacancy For Ceo-Tanzania Association of Accountants-RevisedDocument2 pagesVacancy For Ceo-Tanzania Association of Accountants-RevisedOthman MichuziNo ratings yet
- Project Charter.: Project Title:-A Google GlassesDocument3 pagesProject Charter.: Project Title:-A Google GlassesAliceNo ratings yet
- 10 CodesDocument4 pages10 Codestirso TansoNo ratings yet
- Safety Data Sheet According To EEC-Regulation 91/155/EECDocument6 pagesSafety Data Sheet According To EEC-Regulation 91/155/EECANIBALLOPEZVEGANo ratings yet
- 3.1 Mitosis Ans PDFDocument7 pages3.1 Mitosis Ans PDFtess_15No ratings yet
- Partners Case CCMNDocument4 pagesPartners Case CCMNapi-314349758No ratings yet
- Kotak Mahindra Bank: Presented by Navya.CDocument29 pagesKotak Mahindra Bank: Presented by Navya.CmaheshfbNo ratings yet
- Luxury Salon and SpaDocument10 pagesLuxury Salon and Spalucullan studioNo ratings yet
- Phlebotomy Essentials 5th Edition Ebook PDFDocument61 pagesPhlebotomy Essentials 5th Edition Ebook PDFeric.rodriguez669100% (42)
- GRP 1Document2 pagesGRP 1Yuva RaniNo ratings yet
- Bioshock Audio DiariesDocument6 pagesBioshock Audio DiariesGeorge CuriosoNo ratings yet
- FTL20.pdf Ultrasonic SondeDocument20 pagesFTL20.pdf Ultrasonic SondeJaroslav BiresNo ratings yet
- Thesis On Corporate Governance and Firm PerformanceDocument10 pagesThesis On Corporate Governance and Firm Performancegja8e2sv100% (2)
- Effect of Temperature On SolubilityDocument8 pagesEffect of Temperature On SolubilityMuzahid KhatryNo ratings yet
- Using Snap Test Kits Poster enDocument1 pageUsing Snap Test Kits Poster enMoisés RodríguezNo ratings yet
- Soal Pas B.ing KLS 7Document2 pagesSoal Pas B.ing KLS 7Hernadi TaLaNo ratings yet
- Lecture 3 - Pressure Distribution in FluidDocument22 pagesLecture 3 - Pressure Distribution in FluidChristophe EmerichNo ratings yet
- Uponor v. Sioux Chief Mfg.Document5 pagesUponor v. Sioux Chief Mfg.PriorSmartNo ratings yet
- RTI Online Submit Request FormDocument1 pageRTI Online Submit Request FormRinky SharmaNo ratings yet