You might also like
- Choanal Atresia2Document40 pagesChoanal Atresia2pramod555No ratings yet
- Tuberculous Spondylitis (TB Spine/pott's Disease)Document28 pagesTuberculous Spondylitis (TB Spine/pott's Disease)Divo Septian Zarwin100% (1)
- A Perspective in Accelerated Orthodontics With Aligner Treatment 2017 Seminars in OrthodonticsDocument7 pagesA Perspective in Accelerated Orthodontics With Aligner Treatment 2017 Seminars in Orthodonticsdruzair007No ratings yet
- Chapter 1 - Quiz 2 Form A: A. B. C. D. E. F. G. H. I. J. K. L. M. N. O. P. 1. 2. 3. 4. 5. 6. 7. 8Document2 pagesChapter 1 - Quiz 2 Form A: A. B. C. D. E. F. G. H. I. J. K. L. M. N. O. P. 1. 2. 3. 4. 5. 6. 7. 8Olalekan Oyekunle0% (1)
- Give Me Five 6 Pupils BookDocument129 pagesGive Me Five 6 Pupils BookAdrian Gonzalez100% (5)
- Otosclerosis LT11 KHDocument57 pagesOtosclerosis LT11 KHKyaw HtetNo ratings yet
- OtosclerosisDocument36 pagesOtosclerosisShamsheer ShaikNo ratings yet
- OtosclerosisDocument31 pagesOtosclerosisashry909100% (1)
- Meniere's Disease & OtosclerosisDocument44 pagesMeniere's Disease & OtosclerosisNadzirah Ahmad JailaniNo ratings yet
- OtosclerosisDocument9 pagesOtosclerosisSuprit SnNo ratings yet
- OTOSCLEROSISDocument21 pagesOTOSCLEROSISmounikaNo ratings yet
- OtosclerosisDocument85 pagesOtosclerosisigorNo ratings yet
- Otosclerosis presentation MBBSDocument119 pagesOtosclerosis presentation MBBSFaltuNo ratings yet
- Pediatric - Hearing - Loss Lau 3-17-10Document45 pagesPediatric - Hearing - Loss Lau 3-17-10Arief FakhrizalNo ratings yet
- Otosclerosis Slides 061018Document96 pagesOtosclerosis Slides 061018Paraguay De La Cruz JoelNo ratings yet
- Background: MeningitisDocument7 pagesBackground: MeningitisranmiNo ratings yet
- Tuli Mendadak (Sudden Deafness)Document26 pagesTuli Mendadak (Sudden Deafness)Marisa FatkiyaNo ratings yet
- Anesthetic Considerations in Patients Posted For Surgery With Ankylosing SpondylitisDocument43 pagesAnesthetic Considerations in Patients Posted For Surgery With Ankylosing Spondylitisanuk_1129No ratings yet
- OtosclerosisDocument44 pagesOtosclerosisSonal Sharma100% (1)
- OtosclerosisDocument9 pagesOtosclerosisHelgaNo ratings yet
- O To SclerosisDocument9 pagesO To SclerosisHelgaNo ratings yet
- Chapter 143: Otosclerosis (OS) : Sameer Ahmed 2/23/2011Document20 pagesChapter 143: Otosclerosis (OS) : Sameer Ahmed 2/23/2011Bedo BodyNo ratings yet
- Pott DiseaseDocument15 pagesPott DiseasejunkirinNo ratings yet
- O To SclerosisDocument23 pagesO To SclerosisJennifer Dixon100% (1)
- Orbital Tumors: James M. Ridgway, MDDocument25 pagesOrbital Tumors: James M. Ridgway, MDAyuni KarnielaNo ratings yet
- SNHLDocument200 pagesSNHLOwais NadeemNo ratings yet
- Stanford Medicine Conductive Hearing LossDocument2 pagesStanford Medicine Conductive Hearing LossStrawberry ShortcakeNo ratings yet
- Batson2017 OtosclerosisDocument6 pagesBatson2017 OtosclerosisnuhajazminNo ratings yet
- OtosclerosisDocument31 pagesOtosclerosisSubramaniyanNo ratings yet
- Sensorineural Hearing LossDocument19 pagesSensorineural Hearing LossBenitaNo ratings yet
- Diseases and Treatment of CartilageDocument42 pagesDiseases and Treatment of Cartilageheena solankiNo ratings yet
- Meniere's DiseaseDocument50 pagesMeniere's DiseaseRaisa CleizeraNo ratings yet
- Chronic Suppurative Otitis Media: Drhpsingh Additional ProfessorDocument44 pagesChronic Suppurative Otitis Media: Drhpsingh Additional ProfessorIndieNo ratings yet
- Choanal Atresia2Document40 pagesChoanal Atresia2Mavina ReeNaNo ratings yet
- Document 32Document3 pagesDocument 32Play ListNo ratings yet
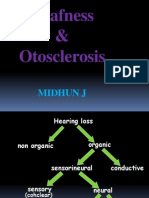
- Deafness & Otosclerosis: Midhun JDocument44 pagesDeafness & Otosclerosis: Midhun JRohit R PillaiNo ratings yet
- Balance Disorders and Vestibular Function Testing - 230602 - 081139Document55 pagesBalance Disorders and Vestibular Function Testing - 230602 - 081139diana mistraNo ratings yet
- Oral Pathology NotesDocument162 pagesOral Pathology NotesDaniel Atieh100% (1)
- Squamous Cell Carcinoma of the Tongue: A Case ReportDocument53 pagesSquamous Cell Carcinoma of the Tongue: A Case ReportWacky BlankNo ratings yet
- Background (2003)Document8 pagesBackground (2003)Jessarene Verzosa Latiza RNNo ratings yet
- Otosclerosis: Aditya Ghosh Roy PGT-2 M.S. E.N.T. N.R.S.M.C.HDocument130 pagesOtosclerosis: Aditya Ghosh Roy PGT-2 M.S. E.N.T. N.R.S.M.C.Hanon_205487480No ratings yet
- Temporal Bone Fractures and Surgical Approaches For CSF LeaksDocument29 pagesTemporal Bone Fractures and Surgical Approaches For CSF LeaksDrravikumar BhandariNo ratings yet
- Mandibulofacial Dysostosis, Also Known As Treacher CollinsDocument19 pagesMandibulofacial Dysostosis, Also Known As Treacher CollinsMoe KebabNo ratings yet
- Legg Calve PerthesDocument93 pagesLegg Calve PerthesAkshay LakraNo ratings yet
- Acute Otitis MediaDocument16 pagesAcute Otitis Mediaadrianne18sNo ratings yet
- Kung 2007Document10 pagesKung 2007Sarah fadlainiNo ratings yet
- Conductive Hearing Loss With An Intact Tympanic Membrane: Diagnosed ApproachesDocument5 pagesConductive Hearing Loss With An Intact Tympanic Membrane: Diagnosed ApproachesMonika ZikraNo ratings yet
- Understanding OtosclerosisDocument75 pagesUnderstanding OtosclerosisShivaam KesarwaaniNo ratings yet
- Pedi HN SlidesDocument71 pagesPedi HN SlidesvelangniNo ratings yet
- Transient Hip SynovitisDocument43 pagesTransient Hip SynovitisnurulNo ratings yet
- Craniofacial SyndromesDocument101 pagesCraniofacial SyndromesSaranya MohanNo ratings yet
- Squamous Cell CarcinomaDocument53 pagesSquamous Cell CarcinomaWacky BlankNo ratings yet
- Eruption Cyst 22Document40 pagesEruption Cyst 22Taki EmmanuelNo ratings yet
- Meniere's Disease Guide: Symptoms, Causes and TreatmentDocument47 pagesMeniere's Disease Guide: Symptoms, Causes and Treatmentadel madanyNo ratings yet
- Acute Scrotum, Differential DiagnosisDocument57 pagesAcute Scrotum, Differential DiagnosisRajesh Menon100% (1)
- Incus and Malleostapedotomy, Stapedectomy, StapedotomyDocument16 pagesIncus and Malleostapedotomy, Stapedectomy, Stapedotomyraghad.bassalNo ratings yet
- Otosclerosis Anddysplasias of Thetemporal BoneDocument19 pagesOtosclerosis Anddysplasias of Thetemporal BoneDianithus169No ratings yet
- Cystic Bone LesionsDocument47 pagesCystic Bone LesionsAnwar KhanNo ratings yet
- LARGE JOINTS IN HEALTH AND DiseaseDocument75 pagesLARGE JOINTS IN HEALTH AND DiseaseIdris Balasa IdrisNo ratings yet
- Nur Adzyan Ruhaizad Bone Joint Hand Infections 543-15-16Document51 pagesNur Adzyan Ruhaizad Bone Joint Hand Infections 543-15-16Star CruiseNo ratings yet
- Pott’s Disease: A Concise OverviewDocument54 pagesPott’s Disease: A Concise OverviewDexter Flores100% (1)
- 11.kuliah International 2009Document35 pages11.kuliah International 2009Magfira Al HabsyiNo ratings yet
- NEDO's Role in International Technical Cooperation ProjectsDocument45 pagesNEDO's Role in International Technical Cooperation Projectsamitsh20072458No ratings yet
- Book Review - Water, Ecosystems and Society A Confluence of Disciplines. by Jayanta BandyopadhyayDocument2 pagesBook Review - Water, Ecosystems and Society A Confluence of Disciplines. by Jayanta BandyopadhyayPDNo ratings yet
- Life Saving Appliance: Personal Life-Saving Appliances Lifeboats & Rescue Boats LiferaftsDocument18 pagesLife Saving Appliance: Personal Life-Saving Appliances Lifeboats & Rescue Boats Liferaftsdafa dzaky100% (1)
- JAOP Progress ReportDocument36 pagesJAOP Progress ReportnidhisasidharanNo ratings yet
- Unit 1 Unit 2 Unit 3 DIFFERENTIAL CALCULUS 1 2 3 PDFDocument124 pagesUnit 1 Unit 2 Unit 3 DIFFERENTIAL CALCULUS 1 2 3 PDFjayaram prakash kNo ratings yet
- Hazardous Waste Identification GuidanceDocument105 pagesHazardous Waste Identification GuidanceMiguel TorresNo ratings yet
- Cast Steel y Strainer Ansi Class 150Document2 pagesCast Steel y Strainer Ansi Class 150aurinkokelloNo ratings yet
- Usg Iom PDFDocument56 pagesUsg Iom PDFAnonymous 7xHNgoKE6eNo ratings yet
- Gardening Tool Identification QuizDocument3 pagesGardening Tool Identification Quizcaballes.melchor86No ratings yet
- Gujarat Technological University: W.E.F. AY 2018-19Document4 pagesGujarat Technological University: W.E.F. AY 2018-19Premal PatelNo ratings yet
- Rodriguez ViereaDocument51 pagesRodriguez ViereaAwawawawa UwuwuwuwuNo ratings yet
- Analyzing the Effects of Changing the Values of a, b, and c in the Equation of a Quadratic Function on Its GraphDocument13 pagesAnalyzing the Effects of Changing the Values of a, b, and c in the Equation of a Quadratic Function on Its GraphRamil NacarioNo ratings yet
- Taylor Ebooks 4 Web 0218Document360 pagesTaylor Ebooks 4 Web 0218aquahellNo ratings yet
- Future Visualized in The Movie BrazilDocument16 pagesFuture Visualized in The Movie BrazilsloutfyNo ratings yet
- Interview Questions - Godrej Technical & HR Interview QuestionsDocument9 pagesInterview Questions - Godrej Technical & HR Interview Questionssasithar jaisankaranNo ratings yet
- PWR Bi2Document11 pagesPWR Bi2GOMTINo ratings yet
- Rift Vally BC N RegularDocument308 pagesRift Vally BC N RegularCabdisacid yasinNo ratings yet
- The Sound of MusicDocument6 pagesThe Sound of MusicRajdeep MukherjeeNo ratings yet
- Parts of the Globe: Prime Meridian, Equator and Climate ZonesDocument18 pagesParts of the Globe: Prime Meridian, Equator and Climate Zonesmelgazar tanjayNo ratings yet
- Ymfc Al SetupDocument18 pagesYmfc Al SetupredaNo ratings yet
- July 17, 2015 Strathmore TimesDocument32 pagesJuly 17, 2015 Strathmore TimesStrathmore TimesNo ratings yet
- Nexon Genuine AccessoriesDocument15 pagesNexon Genuine AccessoriesjagaaniNo ratings yet
- Modeling Endocrine Control of The Pituitary-Ovarian Axis: Androgenic Influence and Chaotic DynamicsDocument22 pagesModeling Endocrine Control of The Pituitary-Ovarian Axis: Androgenic Influence and Chaotic DynamicsKerin ArdyNo ratings yet
- Literature ReviewDocument2 pagesLiterature ReviewFaith Arpon AbogandaNo ratings yet
- Wall Mountable Switches - Wall Mounting GuideDocument3 pagesWall Mountable Switches - Wall Mounting GuideMarcos FilipeNo ratings yet
- Oukfxu DH Lwpuk Ladyu@Izs'K.K GSRQ Izns"K LRJ Ij MRRJNK H Ysoy 1) 2, Oa 3 LRJ Ds VF/KDKFJ Ksa Ds Leidz LWDocument12 pagesOukfxu DH Lwpuk Ladyu@Izs'K.K GSRQ Izns"K LRJ Ij MRRJNK H Ysoy 1) 2, Oa 3 LRJ Ds VF/KDKFJ Ksa Ds Leidz LWNishant KumarNo ratings yet
- Due Amount: We're ListeningDocument2 pagesDue Amount: We're ListeningYogesh PawarNo ratings yet