You might also like
- OtosclerosisDocument31 pagesOtosclerosisashry909100% (1)
- OtosclerosisDocument36 pagesOtosclerosisShamsheer ShaikNo ratings yet
- OtosclerosisDocument8 pagesOtosclerosisAhlam DreamsNo ratings yet
- Understanding OtosclerosisDocument75 pagesUnderstanding OtosclerosisShivaam KesarwaaniNo ratings yet
- Background: MeningitisDocument7 pagesBackground: MeningitisranmiNo ratings yet
- Otosclerosis ExplainedDocument12 pagesOtosclerosis ExplainedAhmed MorsyNo ratings yet
- OTOSCLEROSISDocument75 pagesOTOSCLEROSISShivaam KesarwaaniNo ratings yet
- O To SclerosisDocument9 pagesO To SclerosisHelgaNo ratings yet
- OtosclerosisDocument31 pagesOtosclerosisSubramaniyanNo ratings yet
- OtosclerosisDocument9 pagesOtosclerosisHelgaNo ratings yet
- Pemicu 4 "Mengapa Telingaku Tak Dapat Mendengar?": Adrian - 405100018 - Blok PenginderaanDocument71 pagesPemicu 4 "Mengapa Telingaku Tak Dapat Mendengar?": Adrian - 405100018 - Blok PenginderaanRilianda SimbolonNo ratings yet
- Otosclerosis Anddysplasias of Thetemporal BoneDocument19 pagesOtosclerosis Anddysplasias of Thetemporal BoneDianithus169No ratings yet
- Jurding Otosklerosis Nor Azmina 112017074Document19 pagesJurding Otosklerosis Nor Azmina 112017074beatriceNo ratings yet
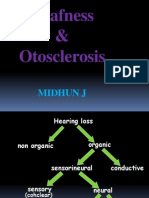
- Deafness & Otosclerosis: Midhun JDocument44 pagesDeafness & Otosclerosis: Midhun JRohit R PillaiNo ratings yet
- AR - 09-15 - Chen 5Document10 pagesAR - 09-15 - Chen 5Arnesh kumar issarNo ratings yet
- OTOSCLEROSISDocument21 pagesOTOSCLEROSISmounikaNo ratings yet
- Oto TemporalDocument13 pagesOto TemporalMoisés AarónNo ratings yet
- Meniere's Disease & OtosclerosisDocument44 pagesMeniere's Disease & OtosclerosisNadzirah Ahmad JailaniNo ratings yet
- Otosclerosis presentation MBBSDocument119 pagesOtosclerosis presentation MBBSFaltuNo ratings yet
- Makarem 2010Document4 pagesMakarem 2010Andi YayatNo ratings yet
- Pediatric - Hearing - Loss Lau 3-17-10Document45 pagesPediatric - Hearing - Loss Lau 3-17-10Arief FakhrizalNo ratings yet
- OTOSCLEROSIS: PATHOGENESIS, DIAGNOSIS AND MANAGEMENTDocument112 pagesOTOSCLEROSIS: PATHOGENESIS, DIAGNOSIS AND MANAGEMENTanon_205487480No ratings yet
- Danesh 2018Document16 pagesDanesh 2018gemapesfNo ratings yet
- Diseases of Periradicular TissuesDocument62 pagesDiseases of Periradicular Tissuesanubhutigupta1404No ratings yet
- OSTEOMYELITIS OF JAW: PATHOGENESIS & MANAGEMENTDocument35 pagesOSTEOMYELITIS OF JAW: PATHOGENESIS & MANAGEMENTOded KantzukerNo ratings yet
- Sensorineural Hearing LossDocument19 pagesSensorineural Hearing LossBenitaNo ratings yet
- Meniere's DiseaseDocument50 pagesMeniere's DiseaseRaisa CleizeraNo ratings yet
- Otosclerosis & Acostic NeuromaDocument44 pagesOtosclerosis & Acostic NeuromaAbdullah AnsarNo ratings yet
- OtosclerosisDocument9 pagesOtosclerosisSuprit SnNo ratings yet
- Imaging in Otosclerosis: A Pictorial ReviewDocument8 pagesImaging in Otosclerosis: A Pictorial ReviewChlo14No ratings yet
- Ear Notes - ExtractDocument50 pagesEar Notes - Extractadham bani younesNo ratings yet
- Nikolaus Ronald Indra 4Document137 pagesNikolaus Ronald Indra 4Florence StellaNo ratings yet
- Cochlear OtosclerosisDocument6 pagesCochlear OtosclerosisadriricaldeNo ratings yet
- Hennebert's SignDocument3 pagesHennebert's SignatmhyaNo ratings yet
- Superior Canal Dehiscence: Review of A New ConditionDocument7 pagesSuperior Canal Dehiscence: Review of A New Conditionapi-19500641No ratings yet
- Otosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandOtosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- AMBOSS Ear QuestionsDocument10 pagesAMBOSS Ear QuestionsSahil DnkNo ratings yet
- Tuli Mendadak (Sudden Deafness)Document26 pagesTuli Mendadak (Sudden Deafness)Marisa FatkiyaNo ratings yet
- Otosclerosis Slides 061018Document96 pagesOtosclerosis Slides 061018Paraguay De La Cruz JoelNo ratings yet
- Cholesteatoma of External Auditory CanalDocument5 pagesCholesteatoma of External Auditory CanallolNo ratings yet
- (19330693 - Journal of Neurosurgery) Superior Semicircular Canal Dehiscence Syndrome - CopieDocument9 pages(19330693 - Journal of Neurosurgery) Superior Semicircular Canal Dehiscence Syndrome - CopieCarmen-BadeaNo ratings yet
- Hearing Loss in Children - Etiology - UpToDateDocument39 pagesHearing Loss in Children - Etiology - UpToDateAlexander AdrielNo ratings yet
- The Medical Treatment of Otosclerosis 20100730Document42 pagesThe Medical Treatment of Otosclerosis 20100730shibhiNo ratings yet
- Cysts of The Jaws and Neck: Wil Dustin P. SinlaoDocument46 pagesCysts of The Jaws and Neck: Wil Dustin P. Sinlaojamaica faith ramonNo ratings yet
- Batson2017 OtosclerosisDocument6 pagesBatson2017 OtosclerosisnuhajazminNo ratings yet
- Ear, Nose and Throat ConditionsDocument10 pagesEar, Nose and Throat ConditionsSaileekitha AjamoniNo ratings yet
- Bone Structure and DiseasesDocument191 pagesBone Structure and DiseasesDrRobin SabharwalNo ratings yet
- Medicine: Characteristics of Hearing Loss in Patients With Herpes Zoster OticusDocument6 pagesMedicine: Characteristics of Hearing Loss in Patients With Herpes Zoster OticusnabilulhakNo ratings yet
- Remota 170426124830Document34 pagesRemota 170426124830Lolo TotoNo ratings yet
- suddensnhl-160220190525Document80 pagessuddensnhl-160220190525mariahovhannisyanNo ratings yet
- Chapter 143: Otosclerosis (OS) : Sameer Ahmed 2/23/2011Document20 pagesChapter 143: Otosclerosis (OS) : Sameer Ahmed 2/23/2011Bedo BodyNo ratings yet
- Otosklerosis - ImradDocument5 pagesOtosklerosis - ImradPutri Dhea Nur AfidaNo ratings yet
- Imaging Appearances of Unusual Conditions of The Middle and Inner EarDocument11 pagesImaging Appearances of Unusual Conditions of The Middle and Inner EarKieda MaliqiNo ratings yet
- Entropion Lower Eyelid Reconstruction - Background, Problem, Epidemiology PDFDocument6 pagesEntropion Lower Eyelid Reconstruction - Background, Problem, Epidemiology PDFyudhaNo ratings yet
- Made By: DR Aditya RanjanDocument32 pagesMade By: DR Aditya RanjanArjun SainiNo ratings yet
- Odontogenic Keratocyst: - Jayalakshmi Preetha Meyyanathan CRIDocument48 pagesOdontogenic Keratocyst: - Jayalakshmi Preetha Meyyanathan CRIJayalakshmi PreethaNo ratings yet
- Inflammatory Lesions of The JAW: Bhavika Pol Vhatkar 1 Yr PGDocument132 pagesInflammatory Lesions of The JAW: Bhavika Pol Vhatkar 1 Yr PGArpita SankhwarNo ratings yet
- ENT - UnitDocument63 pagesENT - Unitsuganthi rajesh kannaNo ratings yet
- Imaging of PediatricHearing LossDocument13 pagesImaging of PediatricHearing LossDianithus169No ratings yet
- Maximising Mental Health Care and ReferralsDocument24 pagesMaximising Mental Health Care and ReferralsSULTAN ADINATANo ratings yet
- Andersson 2003Document6 pagesAndersson 2003IngrydCamposNo ratings yet
- Specialized Fields in Community Health NursingDocument36 pagesSpecialized Fields in Community Health NursingRei Angeline SueloNo ratings yet
- Academy of LDS Dentists Summer 2012 NewsletterDocument4 pagesAcademy of LDS Dentists Summer 2012 Newsletterjoe4299No ratings yet
- Top Hospitals in Bangalore with AddressesDocument183 pagesTop Hospitals in Bangalore with AddressesPrakash ArthurNo ratings yet
- Stress Coping Strategies Adopted by Pregnant Students in The University of Cape Coast and Their Implications For CounsellingDocument9 pagesStress Coping Strategies Adopted by Pregnant Students in The University of Cape Coast and Their Implications For CounsellingIJAR JOURNALNo ratings yet
- Pubmed Tutorial Pubmed TutorialDocument27 pagesPubmed Tutorial Pubmed TutorialSuci FaisalNo ratings yet
- Blom 2012, The Effect of Mouthrinses On Oral Malodor: A Systematic ReviewDocument14 pagesBlom 2012, The Effect of Mouthrinses On Oral Malodor: A Systematic ReviewPhuong ThaoNo ratings yet
- Effectiveness of Structured Teaching Programme On Knowledge Regarding Post - Menopausal Syndrome Among Menopausal WomenDocument4 pagesEffectiveness of Structured Teaching Programme On Knowledge Regarding Post - Menopausal Syndrome Among Menopausal WomenEditor IJTSRDNo ratings yet
- KUHS Changes BDS RegulationsDocument1 pageKUHS Changes BDS RegulationsJoseph John K PothanikatNo ratings yet
- AU Ortho Journal PDFDocument436 pagesAU Ortho Journal PDFadithyaram011549No ratings yet
- Final Ger Syllbus Jan16 Bridging 2016 After DR ModificationDocument2 pagesFinal Ger Syllbus Jan16 Bridging 2016 After DR ModificationHaneenNo ratings yet
- International Adoption EssayDocument6 pagesInternational Adoption Essayapi-461209759No ratings yet
- Alcoholism and Drugs Treatment PDFDocument305 pagesAlcoholism and Drugs Treatment PDFAnonymous g3sy0uINo ratings yet
- Coronavirus: The Commission Signs First Contract With AstrazenecaDocument2 pagesCoronavirus: The Commission Signs First Contract With AstrazenecaΤσιμπινός ΣπύροςNo ratings yet
- Obtaining A Diagnostic Electrocardiogram - Clinician's Brief PDFDocument7 pagesObtaining A Diagnostic Electrocardiogram - Clinician's Brief PDFpianisteverNo ratings yet
- Cinnamon Contact Stomatitis: A Case Report and ReviewDocument2 pagesCinnamon Contact Stomatitis: A Case Report and ReviewDwiNo ratings yet
- Quality Control in HistopathologyDocument6 pagesQuality Control in HistopathologyRK MalhotraNo ratings yet
- Treatment Protocol For Retrieval of Toothroot Fragment Displaced in Maxillary Sinus Report of Two CasesDocument4 pagesTreatment Protocol For Retrieval of Toothroot Fragment Displaced in Maxillary Sinus Report of Two CasesNeeta Joseph JohnNo ratings yet
- Pearl Zanker School: Shangrila Mia-Ramzan, Principal Recep Iscan, Assistant PrincipalDocument4 pagesPearl Zanker School: Shangrila Mia-Ramzan, Principal Recep Iscan, Assistant PrincipalsirishaNo ratings yet
- Stroke Rehabilitation: Therapy Stroke Rehabilitation: TherapyDocument12 pagesStroke Rehabilitation: Therapy Stroke Rehabilitation: TherapyKripa MathaiNo ratings yet
- ParamyxoviridaeDocument27 pagesParamyxoviridaeFarrah BenoitNo ratings yet
- Doctor, S DetailsDocument3 pagesDoctor, S DetailsSteven BryantNo ratings yet
- ADA 2022 - Tecnologia em DiabetesDocument16 pagesADA 2022 - Tecnologia em DiabetesRafael Porto LeiteNo ratings yet
- Hazard Assessment FormDocument4 pagesHazard Assessment FormБаясааАхNo ratings yet
- NCP MaternalDocument3 pagesNCP MaternalArmand CabonitaNo ratings yet
- Advanced Medicine Recall A Must For MRCP PDFDocument712 pagesAdvanced Medicine Recall A Must For MRCP PDFKai Xin100% (2)
- Vital InformationDocument2 pagesVital Informationletz_90No ratings yet
- 7 Reasons Youre Tired All The Time PreventionDocument16 pages7 Reasons Youre Tired All The Time Preventionsharkz fujiwaraNo ratings yet
- Nursing Process, Fluids, Acid Base, IV CalcDocument24 pagesNursing Process, Fluids, Acid Base, IV CalcStephanieNo ratings yet