You might also like
- The Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionFrom EverandThe Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionNo ratings yet
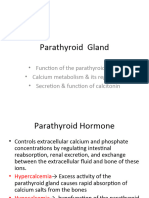
- A Simple Guide to Hyperparathyroidism, Treatment and Related DiseasesFrom EverandA Simple Guide to Hyperparathyroidism, Treatment and Related DiseasesNo ratings yet
- Calcium PhysiologyDocument17 pagesCalcium Physiologyالعياده التخصصيه للسكريNo ratings yet
- Calcium MetabolismDocument29 pagesCalcium MetabolismsnehaNo ratings yet
- Hypercalcemia (F&e)Document3 pagesHypercalcemia (F&e)Sarah Grace CajucomNo ratings yet
- Etiology of HypercalcemiaDocument10 pagesEtiology of HypercalcemiaJohan ArocaNo ratings yet
- Common ElectrolyteDocument48 pagesCommon ElectrolytemekuriawNo ratings yet
- FLUIDS AND ELECTROLYTES MNGTDocument44 pagesFLUIDS AND ELECTROLYTES MNGTremerose100% (1)
- Calcium Homeostasis: Normal Plasma LevelsDocument5 pagesCalcium Homeostasis: Normal Plasma LevelsE MeerNo ratings yet
- Etiology of HypercalcemiaDocument10 pagesEtiology of HypercalcemiaDrKnysaNo ratings yet
- Function Maintain Homeostatic Balance With Respect To Fluids, Electrolytes, and Organic SolutesDocument8 pagesFunction Maintain Homeostatic Balance With Respect To Fluids, Electrolytes, and Organic SolutesNikki SalivioNo ratings yet
- 6.1 Agents That Affect Bone Mineral HomeostasisDocument17 pages6.1 Agents That Affect Bone Mineral HomeostasisAsem AlhazmiNo ratings yet
- Electrolyte CompleteDocument6 pagesElectrolyte CompleteTofan Ana100% (2)
- 27 - Hypo and Hypernatremia - and Hypo and Hyperkalieama PDFDocument48 pages27 - Hypo and Hypernatremia - and Hypo and Hyperkalieama PDFEITHAR OmarNo ratings yet
- HypercalcemiaDocument11 pagesHypercalcemiaShizuka Marycris Amane100% (1)
- Calcium and PhosporusDocument29 pagesCalcium and PhosporusJoe AjibadeNo ratings yet
- Pathofishiologis Chronic Kidney DiseaseDocument4 pagesPathofishiologis Chronic Kidney DiseaseNisaNo ratings yet
- Acute Renal Failure8Document35 pagesAcute Renal Failure8Andrew MidaNo ratings yet
- Electrolytes Lab ValuesDocument3 pagesElectrolytes Lab Valuessublee75100% (1)
- Calcium ImbalancesDocument7 pagesCalcium ImbalancesLorelyn Santos CorpuzNo ratings yet
- Renal CalculiDocument3 pagesRenal Calculiasmauidris305No ratings yet
- Background: PTH-mediated HypercalcemiaDocument3 pagesBackground: PTH-mediated HypercalcemiaDiana TardecillaNo ratings yet
- HypercalcemiaDocument39 pagesHypercalcemiaPrajina KansakarNo ratings yet
- Hyper para Thyroid Is MDocument27 pagesHyper para Thyroid Is MIbrahimWagesNo ratings yet
- Hdp301f&e Imbalancesf2020Document6 pagesHdp301f&e Imbalancesf2020Linda NguyenNo ratings yet
- Calcium & Phosphorus AnishDocument52 pagesCalcium & Phosphorus AnishAnish JoshiNo ratings yet
- Hormonal Control of Calcium and Phosphate MetabolismDocument50 pagesHormonal Control of Calcium and Phosphate MetabolismhamidNo ratings yet
- Sirrhosis HatiDocument6 pagesSirrhosis HatikimokberusungNo ratings yet
- Parathyroid GlandsDocument4 pagesParathyroid GlandsMary Grace Buscargas PolancosNo ratings yet
- Hipokalsemia WikiDocument5 pagesHipokalsemia Wikiagee_quakerNo ratings yet
- Lect 9 Parathyroid Gland-1Document30 pagesLect 9 Parathyroid Gland-1warda farooqNo ratings yet
- CALCIUMDocument30 pagesCALCIUMMona Riza PagtabonanNo ratings yet
- Pa Tho PhysiologyDocument14 pagesPa Tho PhysiologyPatricia LeonorNo ratings yet
- NCM 3114 - Altered Urinary PatternsDocument18 pagesNCM 3114 - Altered Urinary PatternsKoleen Lhyte UyNo ratings yet
- Drugs Affecting Calcium BalanceDocument63 pagesDrugs Affecting Calcium BalanceRd Chandane100% (1)
- Ca MG MetabolismDocument48 pagesCa MG MetabolismjusticeboakyeNo ratings yet
- Calcium Salts Calcitonin and CA RegulatorsDocument40 pagesCalcium Salts Calcitonin and CA RegulatorsSudhakar LakavathNo ratings yet
- Calcium Haemostasis: By: Vasavi.NDocument26 pagesCalcium Haemostasis: By: Vasavi.NmahalakshmiNo ratings yet
- Calcium HomeostasisDocument37 pagesCalcium Homeostasispolog.jm610No ratings yet
- Nephrolithiasis: Adnan Alsaka M.D. Nephrology FellowDocument69 pagesNephrolithiasis: Adnan Alsaka M.D. Nephrology FellowMegi Firmandas IINo ratings yet
- Schenck 2007Document16 pagesSchenck 2007Luisa Fernanda Rojas DiazNo ratings yet
- Fluidandelectrolyteimbalance2 220412174955Document39 pagesFluidandelectrolyteimbalance2 220412174955. anil dev.No ratings yet
- Management of Renale Disease-1Document20 pagesManagement of Renale Disease-1Abdur RehmanNo ratings yet
- Labs Electrolyte ChartDocument1 pageLabs Electrolyte ChartmdcmepNo ratings yet
- Endocrine Physiology - Part 3 Parathyroid GlandDocument30 pagesEndocrine Physiology - Part 3 Parathyroid GlandTerrence Beniasi CharumbiraNo ratings yet
- Liver CirrhosisDocument31 pagesLiver CirrhosisMarisol Jane Jomaya50% (2)
- Control Blood of Calcium LevelsDocument2 pagesControl Blood of Calcium Levelswoman in stemNo ratings yet
- Major Intra and Extracellular IonsDocument29 pagesMajor Intra and Extracellular IonsRasel IslamNo ratings yet
- New Guidelines For Potassium Replacement in Clinical PracticeDocument18 pagesNew Guidelines For Potassium Replacement in Clinical PracticeWilmer JimenezNo ratings yet
- What Does High Potassium in Blood Work MeanDocument2 pagesWhat Does High Potassium in Blood Work MeanMathumathi BalakrishnanNo ratings yet
- HypercalcemiaDocument3 pagesHypercalcemiaj h o eNo ratings yet
- Fluid Therapy - 2021Document10 pagesFluid Therapy - 2021Madiha MadiNo ratings yet
- HypocalcemiaDocument2 pagesHypocalcemiaRachel Frances SorillaNo ratings yet
- Hypocalcemia: Dept of Nephrology PsriDocument40 pagesHypocalcemia: Dept of Nephrology Psriind78No ratings yet
- Management of Patients With Urinary and Kidney Stones: On Completion of This Chapter, The Learner Will Be Able ToDocument11 pagesManagement of Patients With Urinary and Kidney Stones: On Completion of This Chapter, The Learner Will Be Able TojhcacbszkjcnNo ratings yet
- Calcium Homeostasis: General PhysiologyDocument6 pagesCalcium Homeostasis: General PhysiologyE MeerNo ratings yet
- Major Fluid and Electrolyte ImbalancesDocument5 pagesMajor Fluid and Electrolyte ImbalancestheglobalnursingNo ratings yet
- Renal StonesDocument48 pagesRenal StonesLamiaa AliNo ratings yet
- Acute Renal Failure & Chronic Renal FailureDocument38 pagesAcute Renal Failure & Chronic Renal FailureArti GondNo ratings yet
- DiureticsDocument3 pagesDiureticsCarl Simon CalingacionNo ratings yet
- Gender and HealthDocument10 pagesGender and HealthVinit KumarNo ratings yet
- Protocol ExampleDocument6 pagesProtocol ExampleWill RíosNo ratings yet
- Pest and Pathogen Threats To Plane Trees 2015Document16 pagesPest and Pathogen Threats To Plane Trees 2015Carles JiménezNo ratings yet
- Humalog Novolog Apidra: Type of Insulin & Brand Names Onset Peak Duration Role in Blood Sugar Management Rapid-ActingDocument2 pagesHumalog Novolog Apidra: Type of Insulin & Brand Names Onset Peak Duration Role in Blood Sugar Management Rapid-ActingkatrinasdNo ratings yet
- Fhsis Formulas: Normal BMI Cutoff: (18.5-22.9 KG/M)Document2 pagesFhsis Formulas: Normal BMI Cutoff: (18.5-22.9 KG/M)Christelle Brookshiel Demayo Marba100% (3)
- Poster MidgutDocument1 pagePoster MidgutMuruga PrakashNo ratings yet
- Congenital Pulmonary Airway (Cystic Adenomatoid) Malformation - UpToDateDocument28 pagesCongenital Pulmonary Airway (Cystic Adenomatoid) Malformation - UpToDateTung PhamNo ratings yet
- Why Do Adolescents DrinkDocument6 pagesWhy Do Adolescents DrinkchukisaliNo ratings yet
- DiabetesMelitus ThalamustudyDocument14 pagesDiabetesMelitus ThalamustudyOktavinaNo ratings yet
- NBCOT Study GuideDocument6 pagesNBCOT Study GuideAlainaNo ratings yet
- Educational Manual Masterword SCD English FINALDocument111 pagesEducational Manual Masterword SCD English FINALbranchardmushabeNo ratings yet
- LUPALS Sexual Health and Contraception QuizDocument107 pagesLUPALS Sexual Health and Contraception QuizShan PatelNo ratings yet
- Successful Sample Medicine Personal Statements - July UpdateDocument50 pagesSuccessful Sample Medicine Personal Statements - July UpdateSamiha SaidNo ratings yet
- Animal BitesDocument48 pagesAnimal BitesJalouis GabalfinNo ratings yet
- Germ Theory of Disease CausationDocument11 pagesGerm Theory of Disease Causationnashreen83% (6)
- Legal Issues CHNDocument17 pagesLegal Issues CHNSamjhana NeupaneNo ratings yet
- DAV Public School, Hehal, Ranchi Monday Test, Class-XI M.M-25 Subject-English Time - 1 HourDocument3 pagesDAV Public School, Hehal, Ranchi Monday Test, Class-XI M.M-25 Subject-English Time - 1 HourSHIVAM KUMAR SINGHNo ratings yet
- Metabolic Syndrome Thesis PDFDocument5 pagesMetabolic Syndrome Thesis PDFafknawjof100% (2)
- Alpha Blockers: Sympatholytic Drugs (Adrenergic Antagonists)Document4 pagesAlpha Blockers: Sympatholytic Drugs (Adrenergic Antagonists)Almabella GecoleNo ratings yet
- Nursing Care Plan For Acute PainDocument5 pagesNursing Care Plan For Acute PainPhilippineNursingDirectory.com100% (9)
- Bangladesh MBBS Curriculum 2012Document489 pagesBangladesh MBBS Curriculum 2012mail_rajib100% (1)
- Heart Rate Variability Threshold As An Alternative.25Document6 pagesHeart Rate Variability Threshold As An Alternative.25Wasly SilvaNo ratings yet
- Clinical and Surgical Aspects of Congenital Heart DiseasesDocument242 pagesClinical and Surgical Aspects of Congenital Heart DiseasesCardiologia PediatricaNo ratings yet
- Ebook Community Pharmacy Symptoms Diagnosis and Treatment PDF Full Chapter PDFDocument67 pagesEbook Community Pharmacy Symptoms Diagnosis and Treatment PDF Full Chapter PDFnancy.larsen721100% (26)
- Chlorhexidine-Alcohol Compared With Povidone-Iodine Preoperative Skin Antisepsis For Cesarean Delivery A Systematic Review and Meta-AnalysisDocument6 pagesChlorhexidine-Alcohol Compared With Povidone-Iodine Preoperative Skin Antisepsis For Cesarean Delivery A Systematic Review and Meta-AnalysisjohnturpoNo ratings yet
- Examinations Council of Health Sciences/Unza: Final Examinations For Diploma in Environmental Sciences FORDocument12 pagesExaminations Council of Health Sciences/Unza: Final Examinations For Diploma in Environmental Sciences FORkalasa royd100% (3)
- AU-Strategi Nasional Mutu Pelayanan Kes-Nov 2019Document92 pagesAU-Strategi Nasional Mutu Pelayanan Kes-Nov 2019Ika Belia PratiwiNo ratings yet
- Massage PerineumDocument13 pagesMassage PerineumGladys AilingNo ratings yet
- JPM 12 01580 - 2022Document10 pagesJPM 12 01580 - 2022mihail.boldeanuNo ratings yet
- Activity - Nutrition On The Internet Worksheet 3Document2 pagesActivity - Nutrition On The Internet Worksheet 3Carlo FernandoNo ratings yet