100% found this document useful (6 votes)
20K views6 pagesGroup Insurance Claim
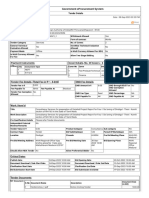
This document is a claim form and supporting documents for a life insurance claim by the family of a deceased government employee in Sindh, Pakistan. It includes the claim form requesting payment to the named nominee. It also includes documents verifying the employee's death, salary, and personal details. Certificates are provided stating there are no outstanding financial issues, audits, inquiries or court cases involving the deceased.
Uploaded by
Adv Sohail BhattiCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
100% found this document useful (6 votes)
20K views6 pagesGroup Insurance Claim
This document is a claim form and supporting documents for a life insurance claim by the family of a deceased government employee in Sindh, Pakistan. It includes the claim form requesting payment to the named nominee. It also includes documents verifying the employee's death, salary, and personal details. Certificates are provided stating there are no outstanding financial issues, audits, inquiries or court cases involving the deceased.
Uploaded by
Adv Sohail BhattiCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd