You might also like
- VBAC Doula Certification Manual v2 April 2019Document111 pagesVBAC Doula Certification Manual v2 April 2019The VBAC Link100% (2)
- OB Gyne Clinical and Teaching CasesDocument221 pagesOB Gyne Clinical and Teaching CaseszzNo ratings yet
- A Comparison of Obstetric Maneuvers For The Acute Management of Shoulder DystociaDocument7 pagesA Comparison of Obstetric Maneuvers For The Acute Management of Shoulder DystociaNellyn Angela HalimNo ratings yet
- Maternal ComplicationsDocument63 pagesMaternal Complicationseumusig4532No ratings yet
- HIV in Pregnancy TopicDocument50 pagesHIV in Pregnancy TopicstepnemoNo ratings yet
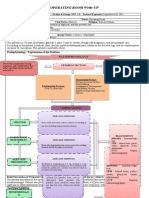
- Operating Room Write-Up: PathophysiologyDocument4 pagesOperating Room Write-Up: PathophysiologyArian May MarcosNo ratings yet
- Peanut Ball Packet For Nurses Final 2021 Updated Imbex0Document11 pagesPeanut Ball Packet For Nurses Final 2021 Updated Imbex0api-600421611No ratings yet
- L&D C-Section Care PlanDocument12 pagesL&D C-Section Care PlanGina Giammalvo100% (2)
- Cephalopelvic DisproportionDocument6 pagesCephalopelvic DisproportionQuennie Alam100% (1)
- Forced Labor: Maternity Care in the United States: Pergamon Studies in Critical SociologyFrom EverandForced Labor: Maternity Care in the United States: Pergamon Studies in Critical SociologyNo ratings yet
- Perceptions and Attitudes of Pregnant Women TowardDocument6 pagesPerceptions and Attitudes of Pregnant Women Towardogunwoleisrael1No ratings yet
- Chapter 2-1Document6 pagesChapter 2-1Robert OkeyoNo ratings yet
- The Knowledge and Attitudes of Palestinian Women Towards Different Childbirth Delivery OptionsDocument6 pagesThe Knowledge and Attitudes of Palestinian Women Towards Different Childbirth Delivery OptionsbaraaNo ratings yet
- Clinical Epidemiology and Global HealthDocument5 pagesClinical Epidemiology and Global Healthsouth8943No ratings yet
- Persepsi SCDocument5 pagesPersepsi SCCH3 CHOLIL R HNo ratings yet
- Literature Review On Uterine Prolapse in NepalDocument7 pagesLiterature Review On Uterine Prolapse in Nepaleyewhyvkg100% (1)
- World Journal of Surgical OncologyDocument9 pagesWorld Journal of Surgical OncologyNikita BowmanNo ratings yet
- The Role of Son Preference in Reproductive Behaviour in PakistanDocument10 pagesThe Role of Son Preference in Reproductive Behaviour in Pakistanbilal rajputNo ratings yet
- Female Sterilization by Tubal Ligation During C-Se PDFDocument5 pagesFemale Sterilization by Tubal Ligation During C-Se PDFYø KåiNo ratings yet
- Contraceptive Use and Unplanned Pregnancy Among Female Sex Workers in ZambiaDocument7 pagesContraceptive Use and Unplanned Pregnancy Among Female Sex Workers in ZambiaNiki Rizqi rachmawatiNo ratings yet
- BJOG - 2005 - Bartellas - Sexuality and Sexual Activity in PregnancyDocument5 pagesBJOG - 2005 - Bartellas - Sexuality and Sexual Activity in Pregnancyศุภชัย ศิลาวัชรพลNo ratings yet
- IDocument2 pagesIAllysa Megan OrpillaNo ratings yet
- Sectio in AfricaDocument10 pagesSectio in AfricaagilNo ratings yet
- Content ServerDocument7 pagesContent ServerNi Wayan Ana PsNo ratings yet
- Perception of Caesarean Section Among PRDocument7 pagesPerception of Caesarean Section Among PRogunwoleisrael1No ratings yet
- Parturition Events and Risk of Urinary Incontinence in Later LifeDocument16 pagesParturition Events and Risk of Urinary Incontinence in Later LifeMutia LailaniNo ratings yet
- Male ParticipationDocument12 pagesMale Participationsiska khairNo ratings yet
- Barriers To Antenatal Care in An Urban Community GambiaDocument9 pagesBarriers To Antenatal Care in An Urban Community GambiaarifsandroNo ratings yet
- Lactation Induction in A Transgender WomanDocument6 pagesLactation Induction in A Transgender WomanM S de BarrosNo ratings yet
- Ojog 2017101317203815Document8 pagesOjog 2017101317203815Elsa Tamara SaragihNo ratings yet
- Perception of Child Bearing Women Towards Male Involvement in Midwifery Practice in Family Support Programme (FSP) Clinic Yenagoa, NigeriaDocument8 pagesPerception of Child Bearing Women Towards Male Involvement in Midwifery Practice in Family Support Programme (FSP) Clinic Yenagoa, NigeriaIOSRjournal100% (1)
- Feto-Maternal Outcomes Following Caesarean SectionDocument6 pagesFeto-Maternal Outcomes Following Caesarean Sectionkirandhami1520No ratings yet
- Chapter 2Document12 pagesChapter 2gkNo ratings yet
- Knowledge and Practice of Cervical Cancer Screening Amongst Nurses in Ahmadu Bello University Teaching Hospital ZariaDocument9 pagesKnowledge and Practice of Cervical Cancer Screening Amongst Nurses in Ahmadu Bello University Teaching Hospital ZariafxbukenyaNo ratings yet
- Partus LamaDocument8 pagesPartus LamaSulis SipinNo ratings yet
- Cesarean Section in Sub-Saharan Africa - Maternal Health, Neonatology and Perinatology - Full TextDocument41 pagesCesarean Section in Sub-Saharan Africa - Maternal Health, Neonatology and Perinatology - Full Textodunze augustusNo ratings yet
- Exploring The Concepts of Intended, Planned, and Wanted PregnancyDocument9 pagesExploring The Concepts of Intended, Planned, and Wanted PregnancyNalin AbeysingheNo ratings yet
- Proposal CS DilveraryDocument5 pagesProposal CS DilveraryhanadiNo ratings yet
- Knowledge and Perception of Women Regarding Bilateral Tubal Ligation in Southwest NigeriaDocument6 pagesKnowledge and Perception of Women Regarding Bilateral Tubal Ligation in Southwest NigeriaEndegena YidegNo ratings yet
- JWH 2006 0295 LowlinkDocument7 pagesJWH 2006 0295 LowlinkRiskhan VirniaNo ratings yet
- A Study of The Attitude and Knowledge of Teenagers in The Pietermaritzburg Area Towards ContraceptionDocument4 pagesA Study of The Attitude and Knowledge of Teenagers in The Pietermaritzburg Area Towards Contraceptionjoe blowNo ratings yet
- Barriers To Men's Involvement in Antenatal and Postnatal Care in Butula, Western KenyaDocument7 pagesBarriers To Men's Involvement in Antenatal and Postnatal Care in Butula, Western KenyaJorge JosaphatNo ratings yet
- The Magnitude of Abortion Complications in KenyaDocument7 pagesThe Magnitude of Abortion Complications in KenyaNaserian SalvyNo ratings yet
- Social Science & Medicine: Anna L. Altshuler, Alison Ojanen-Goldsmith, Paul D. Blumenthal, Lori R. FreedmanDocument8 pagesSocial Science & Medicine: Anna L. Altshuler, Alison Ojanen-Goldsmith, Paul D. Blumenthal, Lori R. FreedmanCristina ToaderNo ratings yet
- Foreign Studies About AbortionDocument3 pagesForeign Studies About AbortionJames MendozaNo ratings yet
- 1-S2.0-S1110569017302935-MainDocument5 pages1-S2.0-S1110569017302935-Maindara intanNo ratings yet
- Emergency Contraceptive Knowledge, Attitudes and Practices Among Female Students at The University of Botswana: A Descriptive SurveyDocument6 pagesEmergency Contraceptive Knowledge, Attitudes and Practices Among Female Students at The University of Botswana: A Descriptive SurveyNaveed AhmadNo ratings yet
- Labor Pain ControlDocument7 pagesLabor Pain ControlDevvy AprianiNo ratings yet
- Delamou2016 Contoh ScopingDocument18 pagesDelamou2016 Contoh ScopingNoor AnisaNo ratings yet
- Recurrence of Preeclampsia in Northern Tanzania: A Registry-Based Cohort StudyDocument9 pagesRecurrence of Preeclampsia in Northern Tanzania: A Registry-Based Cohort StudyLuwuk PosoNo ratings yet
- Impact of Knowledge and AttituDocument23 pagesImpact of Knowledge and AttituAnis SolikahNo ratings yet
- 10.7556 Jaoa.2005.105.8.369Document11 pages10.7556 Jaoa.2005.105.8.369Usman AR VainceNo ratings yet
- Situations of Obstetric Violence From The Perspective of Puerperal WomenDocument7 pagesSituations of Obstetric Violence From The Perspective of Puerperal WomenIJAERS JOURNALNo ratings yet
- Factors Influencing The Health Seeking Behaviors of Wo - 2021 - International JoDocument9 pagesFactors Influencing The Health Seeking Behaviors of Wo - 2021 - International JoRonald QuezadaNo ratings yet
- Obstetric Fistula A Preventable TragedyDocument9 pagesObstetric Fistula A Preventable TragedysrterduNo ratings yet
- CITRADocument9 pagesCITRAAchriani AsraNo ratings yet
- P ('t':'3', 'I':'670968655') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Document10 pagesP ('t':'3', 'I':'670968655') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Septi RahadianNo ratings yet
- The Double-Edged Scalpel: Experiences and Perceptions of Pregnancy and Parenthood During Canadian Surgical Residency TrainingDocument11 pagesThe Double-Edged Scalpel: Experiences and Perceptions of Pregnancy and Parenthood During Canadian Surgical Residency TrainingNikhil ChoudharyNo ratings yet
- Women's Expectations From Delivery Nurses of Vaginal Birth: A Qualitative StudyDocument9 pagesWomen's Expectations From Delivery Nurses of Vaginal Birth: A Qualitative Studykaycelyn jimenezNo ratings yet
- Review of Literature On Breast Self Examination in IndiaDocument8 pagesReview of Literature On Breast Self Examination in Indiac5m82v4xNo ratings yet
- Literature Review On Abortion in GhanaDocument10 pagesLiterature Review On Abortion in Ghanaafdtsebxc100% (1)
- Breast Cancer Screening Practices Among Hong Kong Chinese WomenDocument7 pagesBreast Cancer Screening Practices Among Hong Kong Chinese Womendwi wahyuniNo ratings yet
- An Observation of The Practices of Two Urhobo Traditional Birth AttendantsDocument5 pagesAn Observation of The Practices of Two Urhobo Traditional Birth AttendantsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Abortion Literature ReviewDocument7 pagesAbortion Literature Reviewea8m12sm100% (1)
- Rodiyah Mulyadi (Tugas ANC, InC, PNC)Document40 pagesRodiyah Mulyadi (Tugas ANC, InC, PNC)adelacalistaaNo ratings yet
- Wiklund2012 (Indication)Document8 pagesWiklund2012 (Indication)Noah Borketey-laNo ratings yet
- Birth Preparedness, Complication Readiness and Fathers'Document12 pagesBirth Preparedness, Complication Readiness and Fathers'azida90No ratings yet
- Acog Committee Opinion: Cesarean Delivery On Maternal RequestDocument5 pagesAcog Committee Opinion: Cesarean Delivery On Maternal RequestfbihansipNo ratings yet
- M Heffernan Thesis - Full Version Attitude and Intentions of Healthcare Providers For HPV VaccinesDocument510 pagesM Heffernan Thesis - Full Version Attitude and Intentions of Healthcare Providers For HPV VaccinesHimanshu ShahNo ratings yet
- Admission Into Part-Time Degree ProgrammesDocument3 pagesAdmission Into Part-Time Degree Programmesogunwoleisrael1No ratings yet
- Knowledge and Practice On Exclusive BreaDocument7 pagesKnowledge and Practice On Exclusive Breaogunwoleisrael1No ratings yet
- Implementation of Chatbot in Students PoDocument3 pagesImplementation of Chatbot in Students Poogunwoleisrael1No ratings yet
- E-Waste Management - A Case Study of Lagos State, NigeriaDocument73 pagesE-Waste Management - A Case Study of Lagos State, Nigeriaogunwoleisrael1No ratings yet
- RetroDocument2 pagesRetroogunwoleisrael1No ratings yet
- Chapter 1 To 3 ProfffDocument37 pagesChapter 1 To 3 Profffogunwoleisrael1No ratings yet
- Cystic Fibrosis and PregnancyDocument2 pagesCystic Fibrosis and Pregnancyscience world publishingNo ratings yet
- Changing Trends in Cesarean DeliveryDocument7 pagesChanging Trends in Cesarean DeliveryEditor_IAIMNo ratings yet
- Perceptions and Beliefs Regarding Caesarean Section Among Pregnant Women Receiving Antenatal Care at Ishaka Adventist HospitalDocument12 pagesPerceptions and Beliefs Regarding Caesarean Section Among Pregnant Women Receiving Antenatal Care at Ishaka Adventist HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- Changing Trends in The Indications of Obstetric Hysterectomies in Teaching Rural HospitalDocument5 pagesChanging Trends in The Indications of Obstetric Hysterectomies in Teaching Rural HospitalArun MorayNo ratings yet
- Surgical Approaches For Cesarean Section in CattleDocument5 pagesSurgical Approaches For Cesarean Section in Cattlecatalina igorNo ratings yet
- Kelompok 2 - Tugas Pratikum PT 12 - KODEFIKASI.Document3 pagesKelompok 2 - Tugas Pratikum PT 12 - KODEFIKASI.Nalisa JasrinNo ratings yet
- Care of Post Pasrtal MotherDocument10 pagesCare of Post Pasrtal MotherKelvin KurtNo ratings yet
- Perinatal SbarDocument1 pagePerinatal SbarGlendy DelrioNo ratings yet
- Cesarean Section Postoperative ManagementDocument3 pagesCesarean Section Postoperative ManagementVikas Mohan0% (1)
- Analgesia and Cesarean Delivery RatepdfDocument2 pagesAnalgesia and Cesarean Delivery RatepdfzaftotNo ratings yet
- Gastroschisis and Omphalocele PDFDocument8 pagesGastroschisis and Omphalocele PDFUtama puteraNo ratings yet
- History of Midwifery Era - Stephanie PrestonDocument4 pagesHistory of Midwifery Era - Stephanie Prestonapi-260605210No ratings yet
- Postoperative Pain After Cesarean Section: Assessment and Management in A Tertiary Hospital in A Low-Income CountryDocument6 pagesPostoperative Pain After Cesarean Section: Assessment and Management in A Tertiary Hospital in A Low-Income CountryAkun KelasBNo ratings yet
- Vaginal Birth After Previous Caesarean SectionDocument26 pagesVaginal Birth After Previous Caesarean SectionWonyenghitari George100% (1)
- Maternal and Foetal Outcomes in Pregnancy With Gestational Thrombocytopenia: A Prospective Observational StudyDocument6 pagesMaternal and Foetal Outcomes in Pregnancy With Gestational Thrombocytopenia: A Prospective Observational StudyIJAR JOURNALNo ratings yet
- Cesarean Section PDFDocument9 pagesCesarean Section PDFIeien MuthmainnahNo ratings yet
- Vacuum DeliveryDocument7 pagesVacuum DeliveryJemin KimNo ratings yet
- Trends of Various Techniques of Tubectomy: A Five Year Study in A Tertiary InstituteDocument4 pagesTrends of Various Techniques of Tubectomy: A Five Year Study in A Tertiary InstituteJer KelNo ratings yet
- Vasa Praevia RCOG GTGDocument13 pagesVasa Praevia RCOG GTGMariaBrincatNo ratings yet
- Cesarean Delivery of The Obese Woman - UpToDateDocument25 pagesCesarean Delivery of The Obese Woman - UpToDateBárbara JunqueiraNo ratings yet
- Breech Presentation Delivery CareDocument12 pagesBreech Presentation Delivery CareFatmaNo ratings yet