You might also like
- Penile US and Doppler USDocument2 pagesPenile US and Doppler UShardrocker_2007No ratings yet
- Congenital Absence of The Portal Vein With Splenomegaly in A Young WomanDocument6 pagesCongenital Absence of The Portal Vein With Splenomegaly in A Young WomanIrara RaNo ratings yet
- Diag Imagem Shunt PDFDocument5 pagesDiag Imagem Shunt PDFIzabela RodriguesNo ratings yet
- Ultrasound Evaluation of Renal Artery StenosisDocument24 pagesUltrasound Evaluation of Renal Artery StenosisNguyen Tran CanhNo ratings yet
- Persist SCIAT VEIN and ART-MB-Parry 2002Document5 pagesPersist SCIAT VEIN and ART-MB-Parry 2002residentes dxiNo ratings yet
- New Perspectives On The Development of Extrahepatic Portosystemic ShuntsDocument9 pagesNew Perspectives On The Development of Extrahepatic Portosystemic Shuntsusuaria3No ratings yet
- JOURNALDocument4 pagesJOURNALChiara FajardoNo ratings yet
- Congenital and Acquired Anomalies of The Portal Venous SystemDocument19 pagesCongenital and Acquired Anomalies of The Portal Venous SystemKata TölgyesiNo ratings yet
- ReportDocument1 pageReportShashank Singh RajputNo ratings yet
- Aortic Dissection Associated With Aortic Aneurysms and Posterior Paresis in A DogDocument7 pagesAortic Dissection Associated With Aortic Aneurysms and Posterior Paresis in A DogMuhamad Abdul MubdiNo ratings yet
- Ultrasound Evaluation of Renal Artery StenosisDocument19 pagesUltrasound Evaluation of Renal Artery Stenosisroentgen169100% (1)
- Imagen Hepática Vascular Hígado 2022Document15 pagesImagen Hepática Vascular Hígado 2022Oscar BushNo ratings yet
- Kim 2001Document5 pagesKim 2001DH SiriruiNo ratings yet
- Double-Outlet Right Ventricle With An An Intact Interventricular Septum and Concurrent Hypoplastic Left Ventricle in A CalfDocument6 pagesDouble-Outlet Right Ventricle With An An Intact Interventricular Septum and Concurrent Hypoplastic Left Ventricle in A CalfYoga RivaldiNo ratings yet
- VenosoDocument6 pagesVenosocoopervascba.diradmNo ratings yet
- Utility of Endoscopic Ultrasound in Symptomatic Cut Corners of A ClotDocument3 pagesUtility of Endoscopic Ultrasound in Symptomatic Cut Corners of A ClotDjabhi SpinzzNo ratings yet
- Jurnal RadiologiDocument4 pagesJurnal RadiologielianNo ratings yet
- Obstructed Mediastinal Venous Flow Reverses Brain ScanDocument4 pagesObstructed Mediastinal Venous Flow Reverses Brain ScanRia AngganiNo ratings yet
- Imaging Spectrum of Diseases at the Porta HepatisDocument71 pagesImaging Spectrum of Diseases at the Porta Hepatisjskmkabongo100% (1)
- Doppler Venoso MMSSDocument12 pagesDoppler Venoso MMSSPaola TuerosNo ratings yet
- CT Features of Extrahepatic Arterioportal Fistula in Two CatsDocument4 pagesCT Features of Extrahepatic Arterioportal Fistula in Two CatsVennaOktaviaAnggrainiNo ratings yet
- Embolization of Bronchial Arteries For The Treatment of HEMOPTYSIS. Update and Literature ReviewDocument20 pagesEmbolization of Bronchial Arteries For The Treatment of HEMOPTYSIS. Update and Literature ReviewHai SheikhNo ratings yet
- Two Cases of Variceal Haemorrhage During Living DoDocument3 pagesTwo Cases of Variceal Haemorrhage During Living DoRENAULTNo ratings yet
- 1 s2.0 S0741521495702881 MainDocument12 pages1 s2.0 S0741521495702881 MainRonald VillaNo ratings yet
- Congenital Extrahepatic Portosystemic Deviation of Gastric VeinDocument5 pagesCongenital Extrahepatic Portosystemic Deviation of Gastric VeinMayumi ManoNo ratings yet
- A 2 Year Old Boy With Hypoxemia, Pulmonary HyperteDocument4 pagesA 2 Year Old Boy With Hypoxemia, Pulmonary HyperteagamerocallejasNo ratings yet
- 1 s2.0 073510979390668Q Main PDFDocument9 pages1 s2.0 073510979390668Q Main PDFPribac RamonaNo ratings yet
- Liver Study MaterialDocument17 pagesLiver Study MaterialRazan AlayedNo ratings yet
- Diagnosing Pleural Effusions Through Aspiration and AnalysisDocument28 pagesDiagnosing Pleural Effusions Through Aspiration and AnalysisdradrianramdhanyNo ratings yet
- B-Mode and Doppler Ultrasound Imaging of The Spleen With Canine Splenic Torsion - A Retrospective EvaluationDocument5 pagesB-Mode and Doppler Ultrasound Imaging of The Spleen With Canine Splenic Torsion - A Retrospective EvaluationdenisegmeloNo ratings yet
- Transhepatic Access: Alternative Approach For Right Heart Catheterization and Pulmonary AngiographyDocument3 pagesTranshepatic Access: Alternative Approach For Right Heart Catheterization and Pulmonary AngiographyDavids MarinNo ratings yet
- Inferior Mesenteric Arteriovenous Fistula With Ischemic Colitis: Multidetector Computed Tomographic Angiography For DiagnosisDocument4 pagesInferior Mesenteric Arteriovenous Fistula With Ischemic Colitis: Multidetector Computed Tomographic Angiography For DiagnosisGordana PuzovicNo ratings yet
- Image of The Month: Caput MedusaeDocument1 pageImage of The Month: Caput MedusaeRoery ImoetNo ratings yet
- Jonctiune Pielo UreteralaDocument5 pagesJonctiune Pielo UreteralaRoxana PascalNo ratings yet
- The Role of Ultrasonography in The Evaluation of Diffuse Liver DiseaseDocument13 pagesThe Role of Ultrasonography in The Evaluation of Diffuse Liver Disease{Phantom}No ratings yet
- Vasc Med 2006 Gerhard Herman 183 200Document19 pagesVasc Med 2006 Gerhard Herman 183 200Ahmad ShaltoutNo ratings yet
- Peripheral Arterial DopplerDocument43 pagesPeripheral Arterial Dopplereb3tleNo ratings yet
- 714 Full PDFDocument5 pages714 Full PDFMuhammad Aulia RahmanNo ratings yet
- Renal Vessels Anatomical StudyDocument13 pagesRenal Vessels Anatomical StudyBadea ValentinNo ratings yet
- Student Paper: Communication ÉtudianteDocument3 pagesStudent Paper: Communication ÉtudianteJohan DwiantokoNo ratings yet
- Bilateral Renal VariationsDocument6 pagesBilateral Renal VariationshmqNo ratings yet
- The Fontan Procedure: Anatomy, Complications, and Manifestations of FailureDocument12 pagesThe Fontan Procedure: Anatomy, Complications, and Manifestations of FailureEko SiswantoNo ratings yet
- Comparative Anatomo Radiological Study of Intrahe - 2021 - Annals of Anatomy - ADocument11 pagesComparative Anatomo Radiological Study of Intrahe - 2021 - Annals of Anatomy - AГне ДзжNo ratings yet
- Esophageal VaricesDocument11 pagesEsophageal Varicess.ullah janNo ratings yet
- Lecture Abdomen PediatricDocument85 pagesLecture Abdomen Pediatricdeneshanicholas123No ratings yet
- Adult Choroidal Vein of Galen MalformationDocument5 pagesAdult Choroidal Vein of Galen MalformationSonia Prima Arisa PutriNo ratings yet
- Pulmonary Aneurysms Arteriovenous and FistulasDocument9 pagesPulmonary Aneurysms Arteriovenous and FistulasAlvaro OlateNo ratings yet
- Normal Duplex Doppler Waveforms of Major Abdominal Blood Vessels in Dogs - A ReviewDocument15 pagesNormal Duplex Doppler Waveforms of Major Abdominal Blood Vessels in Dogs - A ReviewdenisegmeloNo ratings yet
- Ecr2017 C-2166Document33 pagesEcr2017 C-2166jbmbritoNo ratings yet
- Color Doppler Ultrasound Critical for Dialysis Fistula AssessmentDocument12 pagesColor Doppler Ultrasound Critical for Dialysis Fistula Assessmenthermalina sabruNo ratings yet
- Dietrich Et Al-2002-Journal of Ultrasound in MedicineDocument9 pagesDietrich Et Al-2002-Journal of Ultrasound in MedicineErikaMRSiaNo ratings yet
- Colitis Due To Ancylostoma Duodenale: ReferencesDocument2 pagesColitis Due To Ancylostoma Duodenale: Referencesinggrit06No ratings yet
- Descricion ofDocument5 pagesDescricion ofLlrss AdnNo ratings yet
- Female Urethral Cavernous Hemangioma, A Rare EntityDocument3 pagesFemale Urethral Cavernous Hemangioma, A Rare EntityAndre GunawanNo ratings yet
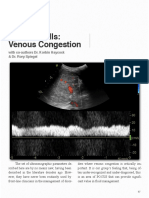
- Venous Congestion ChapterDocument8 pagesVenous Congestion ChapterpcarrascoeNo ratings yet
- (03241750 - Acta Medica Bulgarica) Horseshoe Kidney With Hydronephrosis - Tales of The UnexpectedDocument3 pages(03241750 - Acta Medica Bulgarica) Horseshoe Kidney With Hydronephrosis - Tales of The UnexpectedTeodorNo ratings yet
- Portal HypertensionDocument65 pagesPortal HypertensionVenu MadhavNo ratings yet
- Criss-Cross Heart With Double-Outlet Right VentricleDocument4 pagesCriss-Cross Heart With Double-Outlet Right Ventriclejuana lopezNo ratings yet
- Splanchnic Blood Flow in Patients With Cirrhosis and Portal Hypertension - Investigation With Duplex Doppler USDocument6 pagesSplanchnic Blood Flow in Patients With Cirrhosis and Portal Hypertension - Investigation With Duplex Doppler USdenisegmeloNo ratings yet
- Splenic Hemodynamics and Decreased Endothelial Nitric Oxide Synthase in The Spleen of Rats With Liver CirrhosisDocument9 pagesSplenic Hemodynamics and Decreased Endothelial Nitric Oxide Synthase in The Spleen of Rats With Liver CirrhosisdenisegmeloNo ratings yet
- Power Doppler Sonographic Diagnosis of Torsion in A Wandering SpleenDocument3 pagesPower Doppler Sonographic Diagnosis of Torsion in A Wandering SpleendenisegmeloNo ratings yet
- Splanchnic Blood Flow in Patients With Cirrhosis and Portal Hypertension - Investigation With Duplex Doppler USDocument6 pagesSplanchnic Blood Flow in Patients With Cirrhosis and Portal Hypertension - Investigation With Duplex Doppler USdenisegmeloNo ratings yet
- Suspected Relative Adrenal Insufficiency in A Critically Ill CatDocument5 pagesSuspected Relative Adrenal Insufficiency in A Critically Ill CatdenisegmeloNo ratings yet
- Giraffe Blood CirculationDocument9 pagesGiraffe Blood Circulationthalita asriandinaNo ratings yet
- IV Cannulation: A Guide to Peripheral Vein AccessDocument22 pagesIV Cannulation: A Guide to Peripheral Vein Accessnaveen kumarNo ratings yet
- Treatment of Portal HypertensionDocument10 pagesTreatment of Portal HypertensionLourianne NcNo ratings yet
- Non Sirosis PHDocument11 pagesNon Sirosis PHHIstoryNo ratings yet
- Jama Siegler 2024 Ed 240004 1706915651.01607Document2 pagesJama Siegler 2024 Ed 240004 1706915651.01607Srinivas PingaliNo ratings yet
- Hypoplastic Left Heart Syndrome Diagnosis and ManagementDocument10 pagesHypoplastic Left Heart Syndrome Diagnosis and ManagementMore InterestingNo ratings yet
- Atrial Fibrillation: Classification, Pathophysiology, Mechanisms and Drug Treatment PDFDocument6 pagesAtrial Fibrillation: Classification, Pathophysiology, Mechanisms and Drug Treatment PDFAlya MaulidaNo ratings yet
- Cardio FolletoDocument2 pagesCardio Folletoapi-540783366No ratings yet
- Anti-Anginal Drugs ExplainedDocument19 pagesAnti-Anginal Drugs ExplainedAnusha ZubairNo ratings yet
- Blood Pressure and Pulse LabDocument6 pagesBlood Pressure and Pulse Labapi-638517319No ratings yet
- BP Chart Girls Color WideDocument1 pageBP Chart Girls Color WidealbertNo ratings yet
- Prasugrel Vs Tikagrelor AppendixDocument34 pagesPrasugrel Vs Tikagrelor AppendixSlobodan ObradovicNo ratings yet
- Andreas Kousios, Panayiotis Kouis, Alexandros Hadjivasilis, and Andrie PanayiotouDocument15 pagesAndreas Kousios, Panayiotis Kouis, Alexandros Hadjivasilis, and Andrie Panayiotou7 MNTNo ratings yet
- Dural Venous Sinus Azam SirDocument6 pagesDural Venous Sinus Azam SirLaserdotNo ratings yet
- Ninja - Antianginal Drugs PDFDocument2 pagesNinja - Antianginal Drugs PDFErica Hyeyeon LeeNo ratings yet
- Jurnal CT Cardiac 3Document27 pagesJurnal CT Cardiac 3Kakhfi Gemah PNo ratings yet
- Compare Bisoprolol Vs AtenololDocument4 pagesCompare Bisoprolol Vs AtenololMohammed shamiul ShahidNo ratings yet
- Cambridge English For Nursing 1 PDFDocument123 pagesCambridge English For Nursing 1 PDFMuhNo ratings yet
- A Study To Assess The Knowledge About Risk Factors and Warning Signs of Acute Coronary Syndrome Among Patients Admitted in Cardiac Medical Unit at Sctimst, Triv AndrumDocument72 pagesA Study To Assess The Knowledge About Risk Factors and Warning Signs of Acute Coronary Syndrome Among Patients Admitted in Cardiac Medical Unit at Sctimst, Triv AndrumNise Mon KuriakoseNo ratings yet
- Pulmonary TraumatologyDocument15 pagesPulmonary Traumatologynoor88No ratings yet
- 3.2. ECMO Cannulation and PitfallDocument85 pages3.2. ECMO Cannulation and PitfallEko SarwowibowoNo ratings yet
- Harvey ManualDocument89 pagesHarvey ManualFlowerNo ratings yet
- Cardiovascular System - 4th EdDocument33 pagesCardiovascular System - 4th EdLeah ArabesNo ratings yet
- Dysrhythmia Interpretation Modules 1-6 June 2012Document126 pagesDysrhythmia Interpretation Modules 1-6 June 2012Jess Varose100% (3)
- Arteries vs Veins: The Differences in Blood VesselsDocument11 pagesArteries vs Veins: The Differences in Blood VesselsyarinaosuNo ratings yet
- Hypertension in ElderlyDocument13 pagesHypertension in ElderlybookwormMD100% (2)
- ECG seminar on electrocardiography basicsDocument16 pagesECG seminar on electrocardiography basicsVibha C PrabhuNo ratings yet
- CABGDocument4 pagesCABGMaria Janet BasalloNo ratings yet
- Hemodynamic Monitoring Pocket CardDocument5 pagesHemodynamic Monitoring Pocket CardFitz JaminitNo ratings yet
- Marfan SyndromeDocument4 pagesMarfan SyndromeAtheer AlenziNo ratings yet