You might also like
- Ineffective Breathing PatternDocument3 pagesIneffective Breathing PatternReichelle Perlas62% (13)
- Ineffective Breathing Pattern Pneumonia Nursing Care PlanDocument1 pageIneffective Breathing Pattern Pneumonia Nursing Care PlanJasonlee Baluyot100% (2)
- Date/ Time/ Shift Cues Need Nursing Diagnosis With Rationale Objectives of Care Nursing Interventions With Rationale EvaluationDocument2 pagesDate/ Time/ Shift Cues Need Nursing Diagnosis With Rationale Objectives of Care Nursing Interventions With Rationale EvaluationPauleen Trisha SamparaniNo ratings yet
- Nursing Care Plan in Pedia Ward: Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesNursing Care Plan in Pedia Ward: Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationCharlynne AraojoNo ratings yet
- New Group A - NURSING CARE PLANDocument10 pagesNew Group A - NURSING CARE PLANVelmar De BelenNo ratings yet
- Nursing Care Plan FinalDocument9 pagesNursing Care Plan FinalJny SthaNo ratings yet
- Assessment Planning Nursing Intervention Rationale Evaluation SubjectiveDocument4 pagesAssessment Planning Nursing Intervention Rationale Evaluation SubjectiveChristian Paul Reyes100% (1)
- Group 2 - Activity (NCP, Drug)Document25 pagesGroup 2 - Activity (NCP, Drug)christelNo ratings yet
- NCP Ineffective Breathing ActualDocument3 pagesNCP Ineffective Breathing ActualArian May Marcos100% (1)
- Ineffective Breathing Pattern Related To HyperventilationDocument4 pagesIneffective Breathing Pattern Related To HyperventilationVanessa Charlotte LagunayNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation SubjectiveDocument4 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjectivecammel ramos100% (1)
- Nursing Care Plan: Lorma Colleges Con Template Related Learning ExperienceDocument6 pagesNursing Care Plan: Lorma Colleges Con Template Related Learning ExperiencePauline GarciaNo ratings yet
- Nursing Care Plan: Ineffective Breathing Pattern Related ToDocument4 pagesNursing Care Plan: Ineffective Breathing Pattern Related ToFrudz OrjalezaNo ratings yet
- Nursing Care Plan: Assessment Nursing Diagnosis Nursing Analysis Planning Nursing Interventions Rationale EvaluationDocument4 pagesNursing Care Plan: Assessment Nursing Diagnosis Nursing Analysis Planning Nursing Interventions Rationale EvaluationElla EvangelistaNo ratings yet
- Amat Ncma 219 Pedia Week 5 CTDocument3 pagesAmat Ncma 219 Pedia Week 5 CTRaf AmatNo ratings yet
- Data NSG Diagnosis Goals & Outcomes NSG Interventions Rationale Evaluation O: StoDocument3 pagesData NSG Diagnosis Goals & Outcomes NSG Interventions Rationale Evaluation O: StoClaudineNo ratings yet
- NCP - Sleep ApneaDocument7 pagesNCP - Sleep ApneaEunick VillagraciaNo ratings yet
- NCP 1 AND SOAPIE 1) Ineffective Breathing PatternDocument5 pagesNCP 1 AND SOAPIE 1) Ineffective Breathing PatternMicaela CrisostomoNo ratings yet
- Er NCP AddahDocument2 pagesEr NCP AddahAddah, Dhenaraiza H.No ratings yet
- MCN NCPDocument4 pagesMCN NCPPEARL CHRISTINE CUDALNo ratings yet
- Group 1 Nursing Diagnosis FinalDocument59 pagesGroup 1 Nursing Diagnosis FinalChristian Angelo LeonorNo ratings yet
- Nursing Process Care Plan For Ineffective Breathing Pattern Assessment Diagnosis Planning Implementation EvaluationDocument19 pagesNursing Process Care Plan For Ineffective Breathing Pattern Assessment Diagnosis Planning Implementation EvaluationZIANAH JOY FAMYNo ratings yet
- Student NurseDocument2 pagesStudent NurseTAYABAN, KENNETH JAKE, Q.No ratings yet
- NCP, Drug StudyDocument9 pagesNCP, Drug StudyTresha CaliboNo ratings yet
- Cues Nursing Diagnos Is Backgro Und Knowled Ge Goals and Objectives Nursing Intervention and Rationale EvaluationDocument3 pagesCues Nursing Diagnos Is Backgro Und Knowled Ge Goals and Objectives Nursing Intervention and Rationale EvaluationSkyla FiestaNo ratings yet
- Nursing Care Plan: Lipa City CollegesDocument13 pagesNursing Care Plan: Lipa City CollegesVincent Maralit MaterialNo ratings yet
- NCP SampleDocument8 pagesNCP SampleKeneth Dave AglibutNo ratings yet
- Ineffective Breathing PatternDocument2 pagesIneffective Breathing PatternEna Katherine CanonoNo ratings yet
- Requirement in NCM 312: Presented By: Chloie Marie C. Rosalejos Submitted To: Ma. Lynn C. ParambitaDocument7 pagesRequirement in NCM 312: Presented By: Chloie Marie C. Rosalejos Submitted To: Ma. Lynn C. ParambitaChloie Marie RosalejosNo ratings yet
- NCP NRMFDocument2 pagesNCP NRMFJai CortezNo ratings yet
- PNNCPDocument2 pagesPNNCPJacky BrightNo ratings yet
- Defining CharacteristicsDocument2 pagesDefining CharacteristicsAngel MayNo ratings yet
- Assessment Diagnosis Planning Nursing Intervention Rationale EvaluationDocument15 pagesAssessment Diagnosis Planning Nursing Intervention Rationale EvaluationMariam Yiani Aspiras RacelesNo ratings yet
- Group 2 SOAPIE Case FinalDocument4 pagesGroup 2 SOAPIE Case FinalJames De VeraNo ratings yet
- Nursing Care Plan: Assessm ENT Nursing Diagnos IS Planning Intervention Rationale Evaluati ON Subjectiv eDocument4 pagesNursing Care Plan: Assessm ENT Nursing Diagnos IS Planning Intervention Rationale Evaluati ON Subjectiv eJ. TSNo ratings yet
- NCP SciDocument3 pagesNCP SciJaylord VerazonNo ratings yet
- Nursing Care Plan: Cystic FibrosisDocument4 pagesNursing Care Plan: Cystic FibrosisYael EzraNo ratings yet
- UntitledDocument4 pagesUntitledPie CanapiNo ratings yet
- NCP IcuDocument2 pagesNCP Icujennelyn losantaNo ratings yet
- NCP1223Document3 pagesNCP1223Divine Mercy De JulianNo ratings yet
- Bronchitis NCPDocument8 pagesBronchitis NCPNikael Patun-ogNo ratings yet
- Assessment Explanation of The Problem Objectives Nursing Interventions Rationale EvaluationDocument7 pagesAssessment Explanation of The Problem Objectives Nursing Interventions Rationale EvaluationDanica Kate GalleonNo ratings yet
- Darunday NCP Rotation 6Document3 pagesDarunday NCP Rotation 6Ezra Miguel DarundayNo ratings yet
- Darunday NCP Rotation 6Document3 pagesDarunday NCP Rotation 6Ezra Miguel DarundayNo ratings yet
- NCP 1 1Document10 pagesNCP 1 1Samantha VeraNo ratings yet
- General Question: "Ineffective Airway Clearance" in Children With AsthmaDocument3 pagesGeneral Question: "Ineffective Airway Clearance" in Children With AsthmaGil GanibanNo ratings yet
- NGT and OstomyDocument2 pagesNGT and OstomyDarianne B. BasaNo ratings yet
- Group 6 Group Case Study DONEDocument5 pagesGroup 6 Group Case Study DONEE.R.ONo ratings yet
- NCP Acute BronchitisDocument9 pagesNCP Acute BronchitisCarl Simon CalingacionNo ratings yet
- Ineffective Breathing Pattern Pneumonia Nursing Care PlanDocument1 pageIneffective Breathing Pattern Pneumonia Nursing Care PlanJasonlee BaluyotNo ratings yet
- NCP - Ineffective Airway ClearanceDocument2 pagesNCP - Ineffective Airway ClearancemaxynezolayvarNo ratings yet
- Skills Laboratory 3B (Ett Suctioning) End of Rotation EvaluationDocument4 pagesSkills Laboratory 3B (Ett Suctioning) End of Rotation EvaluationmnchyNo ratings yet
- NCP Ineffective Breathing PatternDocument4 pagesNCP Ineffective Breathing PatternSeika SouiNo ratings yet
- Behavior and Mental Status Can Be Early Signs of Impaired Gas ExchangeDocument2 pagesBehavior and Mental Status Can Be Early Signs of Impaired Gas ExchangeJoanna Marie Lumbre BalbiranNo ratings yet
- Case Study: Acute Exacarbation Chronic Obstructive Aspiration Disease (Aecoad)Document5 pagesCase Study: Acute Exacarbation Chronic Obstructive Aspiration Disease (Aecoad)Muhammad Alif100% (1)
- NCP1Document3 pagesNCP1Alissa MaghopoyNo ratings yet
- Apis Mellifica; or, The Poison of the Honey-Bee, Considered as a Therapeutic AgentFrom EverandApis Mellifica; or, The Poison of the Honey-Bee, Considered as a Therapeutic AgentNo ratings yet
- Snoring, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandSnoring, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
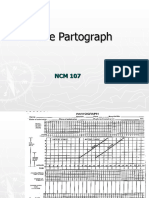
- PartographDocument59 pagesPartographWhitney CabanganNo ratings yet
- Basketball-Module 081755Document15 pagesBasketball-Module 081755Whitney CabanganNo ratings yet
- Mga Katanungan Sa THEO 4Document1 pageMga Katanungan Sa THEO 4Whitney CabanganNo ratings yet
- Facilities and EquipmentDocument11 pagesFacilities and EquipmentWhitney CabanganNo ratings yet
- Group 2Document37 pagesGroup 2Whitney CabanganNo ratings yet
- Maricar Cabangan Humms 11 EmpathyDocument5 pagesMaricar Cabangan Humms 11 EmpathyWhitney CabanganNo ratings yet
- Fellowship ProgramDocument3 pagesFellowship ProgramWhitney CabanganNo ratings yet
- Survey QuestionnaireDocument2 pagesSurvey QuestionnaireWhitney CabanganNo ratings yet
- Whitney CabanganDocument2 pagesWhitney CabanganWhitney CabanganNo ratings yet
- TOP in Clinical Pedutrics PDFDocument227 pagesTOP in Clinical Pedutrics PDFSoad ShedeedNo ratings yet
- Mengenal Kegawatan Pada AnakDocument45 pagesMengenal Kegawatan Pada Anakyasmin100% (1)
- Pulmonary Function Testing - Spirometry, Lung Volume Determination, Diffusing Capacity of Lung For Carbon MonoxideDocument4 pagesPulmonary Function Testing - Spirometry, Lung Volume Determination, Diffusing Capacity of Lung For Carbon MonoxideRundNo ratings yet
- LinesDocument46 pagesLinesHarris ShaikhNo ratings yet
- Aclidinium Bromide 340mcg + Formoterol Fumarate 11.8mcg (Duaklir Genuair Inhalation Powder)Document22 pagesAclidinium Bromide 340mcg + Formoterol Fumarate 11.8mcg (Duaklir Genuair Inhalation Powder)ddandan_2No ratings yet
- Material Safety Data Sheet: 1. Product Identification Curacron 8EDocument6 pagesMaterial Safety Data Sheet: 1. Product Identification Curacron 8EMuhammad El-karimNo ratings yet
- MSDS - Sodium Hypochlorite SolutionDocument3 pagesMSDS - Sodium Hypochlorite SolutionABHINAV MISHALNo ratings yet
- RRL 1Document5 pagesRRL 1Boy MadNo ratings yet
- Safety Data Sheet: Section 1. IdentificationDocument12 pagesSafety Data Sheet: Section 1. Identificationabdelhamid ghazalaNo ratings yet
- Appendix For Chiller MS Phase Rev.00 PDFDocument102 pagesAppendix For Chiller MS Phase Rev.00 PDFSamboy DionisioNo ratings yet
- A Review of The Breathing Mechanism For SingingDocument7 pagesA Review of The Breathing Mechanism For SingingKasia Brodowska-KlingerNo ratings yet
- 12 Ways To Breathe - WikihowDocument23 pages12 Ways To Breathe - WikihowvkseknNo ratings yet
- Miss.G.Nisha AS - TEN - US - 5726 19 - 005726 - 212267 13Y / Female DR - Self 4-Mar-2021Document2 pagesMiss.G.Nisha AS - TEN - US - 5726 19 - 005726 - 212267 13Y / Female DR - Self 4-Mar-2021jeyaraman jcbNo ratings yet
- Medical Terminology For Health Professions 6th Edition Ehrlich Test BankDocument9 pagesMedical Terminology For Health Professions 6th Edition Ehrlich Test Banksinapateprear4k100% (34)
- Drager Babylog 8000 PDFDocument1 pageDrager Babylog 8000 PDFramuNo ratings yet
- Executive Order No. 017 S. 2022 - ORGANIZING THE BARANGAY HEALTH EMERGENCY RESPONSE TEAM (BHERT) FOR NOVEL CORONA VIRUSDocument2 pagesExecutive Order No. 017 S. 2022 - ORGANIZING THE BARANGAY HEALTH EMERGENCY RESPONSE TEAM (BHERT) FOR NOVEL CORONA VIRUSSAMMY SARMIENTO100% (6)
- Pulmonary Board Review SeekDocument56 pagesPulmonary Board Review Seektechang1No ratings yet
- Hempathane Topcoat 55219 Base 5521967280 En-UsDocument11 pagesHempathane Topcoat 55219 Base 5521967280 En-UsSantiago Rafael Galarza JacomeNo ratings yet
- SDS, V-Grade Acrylic - From IPSDocument10 pagesSDS, V-Grade Acrylic - From IPSVio AmarieiNo ratings yet
- Mechanical VentilationDocument18 pagesMechanical VentilationM BNo ratings yet
- User's Instructions For Degil Safety Model No. 74006BDocument1 pageUser's Instructions For Degil Safety Model No. 74006BcandrauzNo ratings yet
- H2S Training Manual 4082472 01Document201 pagesH2S Training Manual 4082472 01Leonardo Gil100% (1)
- Medical Devices in Allergy Practice - 2020 - WaojouDocument27 pagesMedical Devices in Allergy Practice - 2020 - WaojouJoão Pedro SantanaNo ratings yet
- Southern Tagalog ChapterDocument4 pagesSouthern Tagalog ChapterwiltechworksNo ratings yet
- Bronchiectasis Is A Chronic, Irreversible Dilation of The Bronchi and The Bronchioles. Under TheDocument5 pagesBronchiectasis Is A Chronic, Irreversible Dilation of The Bronchi and The Bronchioles. Under Thesandra M. CovarrubiasNo ratings yet
- Emphysema Research ReportDocument19 pagesEmphysema Research Reportحرا مغلNo ratings yet
- Quiz ADocument2 pagesQuiz AMARIA CHARMIN M. MEJIANo ratings yet
- Case Study 2 Pcap-CDocument22 pagesCase Study 2 Pcap-CChona CastorNo ratings yet
- Guided Meditation BreathDocument4 pagesGuided Meditation BreathDomingo de LeonNo ratings yet
- 3M Disposable Filtering Facepiece Respirator Fitting Poster English and SpanishDocument2 pages3M Disposable Filtering Facepiece Respirator Fitting Poster English and SpanishTrunggana AbdulNo ratings yet