You might also like
- How To Switch Insulin Products - Pharm LetterDocument6 pagesHow To Switch Insulin Products - Pharm LetterAraceli LeonNo ratings yet
- Insulin Drug StudyDocument2 pagesInsulin Drug StudyRai Hanah92% (13)
- Vehicular AccidentDocument9 pagesVehicular AccidentCharm TanyaNo ratings yet
- Sonofthegods NeigongDocument797 pagesSonofthegods NeigongCAMERA WAS100% (1)
- Switching Between Insulin Products in Humanitarian Response 2022 Easter Europe 3 18 2022 DDRC English v3Document3 pagesSwitching Between Insulin Products in Humanitarian Response 2022 Easter Europe 3 18 2022 DDRC English v3vijay740No ratings yet
- GUIDELINES FOR INPATIENT DIABETES MANAGEMENT هااامDocument1 pageGUIDELINES FOR INPATIENT DIABETES MANAGEMENT هااامAbu HuzaifaNo ratings yet
- A Practical Guide To Insulin TherapyDocument42 pagesA Practical Guide To Insulin Therapyseun williams100% (2)
- Insulin ChartDocument2 pagesInsulin ChartJohanNone100% (1)
- 2022 Insulin Calculations Cheat Sheet ARDocument4 pages2022 Insulin Calculations Cheat Sheet ARGulsama BabarNo ratings yet
- Actraphane Epar Product Information - en PDFDocument125 pagesActraphane Epar Product Information - en PDFDivyanshu GuptaNo ratings yet
- Insulin Glargine Injection: Active IngredientDocument31 pagesInsulin Glargine Injection: Active Ingredient44abcNo ratings yet
- Novorapid Novomix Pi v8 2021Document19 pagesNovorapid Novomix Pi v8 2021Nazmul Hasan MahmudNo ratings yet
- Annex I Summary of Product CharacteristicsDocument115 pagesAnnex I Summary of Product Characteristicsmelda silviaNo ratings yet
- DM Lab 2 - FinalDocument33 pagesDM Lab 2 - FinalMahamed Wefkey OmranNo ratings yet
- Insulin in DiabetesDocument9 pagesInsulin in DiabetesAbdul SamadNo ratings yet
- Terapi Insulin-1Document46 pagesTerapi Insulin-1Yanti MoonNo ratings yet
- Insulin AdministrationDocument9 pagesInsulin AdministrationMonika JosephNo ratings yet
- Inhaled Insulin: Drug Information: ALERT: US Boxed WarningDocument13 pagesInhaled Insulin: Drug Information: ALERT: US Boxed WarningAnonymous wmF9p2ejNo ratings yet
- Insulin TypesDocument3 pagesInsulin TypesAbdullah A. ElgazarNo ratings yet
- Novo RapidDocument15 pagesNovo RapidPuniska ArtNo ratings yet
- Ryzodeg Epar Product Information - enDocument57 pagesRyzodeg Epar Product Information - enpamela joyce sorianoNo ratings yet
- ADA 2021 Instensifying Injectable Therapy.v.3Document2 pagesADA 2021 Instensifying Injectable Therapy.v.3Ariel GutierrezNo ratings yet
- Insulin Aspart Dan ProteminatedDocument4 pagesInsulin Aspart Dan ProteminatedSastra WijayaNo ratings yet
- Insulin Degludec Insulin Aspart (Ryzodeg 70 30) Prescribing ProtocolDocument5 pagesInsulin Degludec Insulin Aspart (Ryzodeg 70 30) Prescribing ProtocolMiraNo ratings yet
- Lantus Epar Product Information enDocument74 pagesLantus Epar Product Information enNisrinaNurfitriaNo ratings yet
- Optimizing The Use of NPH Insulin in Patients With Type 2 Diabetes MellitusDocument3 pagesOptimizing The Use of NPH Insulin in Patients With Type 2 Diabetes MellitusGulzaib KhokharNo ratings yet
- Insulin Initiation PPT - PPTX 2Document53 pagesInsulin Initiation PPT - PPTX 2Meno Ali100% (1)
- Insulin History & Modality For Diabetic Patient: A. Makbul M. AmanDocument69 pagesInsulin History & Modality For Diabetic Patient: A. Makbul M. AmanRey Alwiwikh100% (1)
- LantusDocument10 pagesLantusShanta100% (3)
- Annex I Summary of Product CharacteristicsDocument109 pagesAnnex I Summary of Product CharacteristicsiammarkeinsteinNo ratings yet
- NovoRapid (Insulin Aspart) PDFDocument113 pagesNovoRapid (Insulin Aspart) PDFAchmad SuryadiNo ratings yet
- DiabetesMellitisChap09 SpecialPopulationsDocument12 pagesDiabetesMellitisChap09 SpecialPopulationsarmandoNo ratings yet
- Apidra WC500025250Document165 pagesApidra WC500025250LaurenArperNo ratings yet
- Ryzodeg Product Information 13Document21 pagesRyzodeg Product Information 1311569No ratings yet
- Novolin R SQ (Regular Insulin)Document3 pagesNovolin R SQ (Regular Insulin)ENo ratings yet
- General Principles of Insulin Therapy in Diabetes MellitusDocument12 pagesGeneral Principles of Insulin Therapy in Diabetes MellitusRuban RichardNo ratings yet
- Annex I Summary of Product CharacteristicsDocument81 pagesAnnex I Summary of Product Characteristicsberliani zebuaNo ratings yet
- Novolog (Insulin Aspart)Document3 pagesNovolog (Insulin Aspart)ENo ratings yet
- InsulinDocument4 pagesInsulinHa Zizzle100% (1)
- Insulin Therapy: Prof. Khalifa AbdallahDocument33 pagesInsulin Therapy: Prof. Khalifa AbdallahAhmed Adel MostafaNo ratings yet
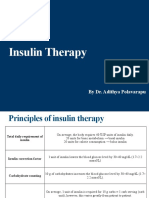
- Insulin Therapy: by Dr. Adithya PolavarapuDocument18 pagesInsulin Therapy: by Dr. Adithya Polavarapuadithya polavarapuNo ratings yet
- Calculate The Dose of Diabetes MellitusDocument5 pagesCalculate The Dose of Diabetes MellitusOmar Nassir MoftahNo ratings yet
- Insulin AdministrationDocument13 pagesInsulin AdministrationMuhammad Aji SantosoNo ratings yet
- Novorapid Product Monograph PDFDocument50 pagesNovorapid Product Monograph PDFAtid AmandaNo ratings yet
- Insulin AspartDocument6 pagesInsulin AspartHutomo PrawirohardjoNo ratings yet
- Novomix Epar Product Information - RoDocument91 pagesNovomix Epar Product Information - RoneculalorenaizabellaNo ratings yet
- Insulin: Deciding How Much Insulin To TakeDocument12 pagesInsulin: Deciding How Much Insulin To Takeராபர்ட் ஆன்றோ ரெனி100% (1)
- General Principles of Insulin Therapy in Diabetes Mellitus - UpToDateDocument25 pagesGeneral Principles of Insulin Therapy in Diabetes Mellitus - UpToDateNeider 1111No ratings yet
- Stimulates Peripheral Glucose Uptake, Inhibits Hepatic Glucose Production, Inhibits Lipolysis and Proteolysis, Regulating Glucose MetabolismDocument4 pagesStimulates Peripheral Glucose Uptake, Inhibits Hepatic Glucose Production, Inhibits Lipolysis and Proteolysis, Regulating Glucose MetabolismKey CelestinoNo ratings yet
- General Principles of Insulin Therapy in Diabetes Mellitus - UpToDateDocument20 pagesGeneral Principles of Insulin Therapy in Diabetes Mellitus - UpToDateabdulghaniNo ratings yet
- Newer Insulins in PediatricsDocument24 pagesNewer Insulins in PediatricsKishore ChandkiNo ratings yet
- Adjusting Your Insulin DoseDocument3 pagesAdjusting Your Insulin DoseLib AsNo ratings yet
- General Principles of Insulin Therapy in Diabetes MellitusDocument24 pagesGeneral Principles of Insulin Therapy in Diabetes MellitusEDWIN WIJAYANo ratings yet
- Calculating Insulin DoseDocument5 pagesCalculating Insulin DoseMąhmóúd SąmíNo ratings yet
- Mod4 Insulin CurvesDocument5 pagesMod4 Insulin Curvesjaya28655746No ratings yet
- Educational Inservice U500 InsulinDocument12 pagesEducational Inservice U500 InsulinCayla KassNo ratings yet
- Insulin Lispro Sanofi Epar Product Information - en PDFDocument63 pagesInsulin Lispro Sanofi Epar Product Information - en PDFAndreea Claudia NegrilaNo ratings yet
- Insulin TherapyDocument60 pagesInsulin Therapylight tweenNo ratings yet
- Diabetes Insulin InitiationDocument12 pagesDiabetes Insulin InitiationSatinder BhallaNo ratings yet
- Test Bank For The Nurse The Math The Meds 3rd Edition by Mulholland DownloadDocument10 pagesTest Bank For The Nurse The Math The Meds 3rd Edition by Mulholland Downloadsarahwatsonmfjtabceri100% (17)
- Organizational Change and Stress Management: Chapter 18 OutlineDocument15 pagesOrganizational Change and Stress Management: Chapter 18 OutlineShreya Saransh GoelNo ratings yet
- MBT-Term Test 1Document45 pagesMBT-Term Test 1lkokodkodNo ratings yet
- Alexander Sanchez: 6046 West Pershing Road Cicero, IL, 60804 708-491-9859Document1 pageAlexander Sanchez: 6046 West Pershing Road Cicero, IL, 60804 708-491-9859Nicolle UreñaNo ratings yet
- Erectile Dysfunction FinalDocument68 pagesErectile Dysfunction Finalmuhibullah saifiNo ratings yet
- LSBM - Fellows 27th Dec 2022 2 PDFDocument2 pagesLSBM - Fellows 27th Dec 2022 2 PDFMullai Kodi KNo ratings yet
- Bahria University Karachi Campus: Transmission Line Fault MonitoringDocument4 pagesBahria University Karachi Campus: Transmission Line Fault Monitoringsaud aliNo ratings yet
- Supply Chain Visibility Excellence: Fostering Security, Resiliency, and EfficiencyDocument27 pagesSupply Chain Visibility Excellence: Fostering Security, Resiliency, and EfficiencyFreddy VargasNo ratings yet
- Group Cohesiveness Case StudyDocument9 pagesGroup Cohesiveness Case Studynsparth0% (1)
- Chapter 2 FluidDocument29 pagesChapter 2 FluidLeonard TanNo ratings yet
- Gly. CarbonateDocument5 pagesGly. Carbonate13201940No ratings yet
- Mg101 - Hygrometer Calibration Equipment English 0Document2 pagesMg101 - Hygrometer Calibration Equipment English 0Anoss OlierNo ratings yet
- ALF Survey Guideline IndexDocument4 pagesALF Survey Guideline IndexKendra Tice100% (2)
- Estimate: SSN Wiring Solutions CorpDocument2 pagesEstimate: SSN Wiring Solutions CorpviksursNo ratings yet
- Worksheet Present Con NameDocument3 pagesWorksheet Present Con NameAleksandra Simoncevska NecovskaNo ratings yet
- Cocoa-Value-Chain-Assessment-Pind FoundationDocument64 pagesCocoa-Value-Chain-Assessment-Pind FoundationAfaaqi Engineering LimitedNo ratings yet
- HDPE MSDS English V1.1Document7 pagesHDPE MSDS English V1.1Pradika WibowoNo ratings yet
- ARM - Grid Tie Inverter 1.5kW - 5kW SpecsDocument1 pageARM - Grid Tie Inverter 1.5kW - 5kW SpecsPhạm QuyếnNo ratings yet
- Jodhpur Sewerage SystemDocument14 pagesJodhpur Sewerage SystemKanishk BhattNo ratings yet
- Axillary Node DissectionDocument71 pagesAxillary Node DissectionKartik Kaistha100% (1)
- Unauthenticated Download Date - 1/31/17 4:04 AMDocument5 pagesUnauthenticated Download Date - 1/31/17 4:04 AMFahmi RaziNo ratings yet
- Hilti X-U NailsDocument10 pagesHilti X-U NailsLightninWolf32No ratings yet
- Boq 112229Document24 pagesBoq 112229neerajNo ratings yet
- Evolution of Dentition in Cattle LifeDocument7 pagesEvolution of Dentition in Cattle LifeDragos MisteryoNo ratings yet
- Brand & Product ManagementDocument10 pagesBrand & Product Managementkhushboo jamwalNo ratings yet
- Preneed Funeral Marketing Program Options For Funeral Home and Cemetery Operations - 3Document7 pagesPreneed Funeral Marketing Program Options For Funeral Home and Cemetery Operations - 3ldubetnt100% (3)
- Flexible Partial DentureDocument5 pagesFlexible Partial DentureDeasireeNo ratings yet
- Steam Bending WoodDocument10 pagesSteam Bending Wooddkpitterson0% (1)
- Fluid Mechanics PDFDocument59 pagesFluid Mechanics PDFsunny chaurasiaNo ratings yet