You might also like
- Automatic Transmission Diagnosis Information SheetDocument1 pageAutomatic Transmission Diagnosis Information SheetValentin IvanovNo ratings yet
- Smile DesignDocument104 pagesSmile DesignEazhil Raj100% (3)
- University of Rizal System: UpperDocument2 pagesUniversity of Rizal System: UpperCes ReyesNo ratings yet
- Dental Record ChartDocument4 pagesDental Record ChartJacqueline Acera Balingit50% (2)
- Dental Trauma Professional PamphletDocument3 pagesDental Trauma Professional Pamphletnona aryan50% (2)
- UntitledDocument11 pagesUntitledibrahim bataNo ratings yet
- 12 Diagnostic Aids For Functional AppliancesDocument240 pages12 Diagnostic Aids For Functional AppliancesDr Shivam VermaNo ratings yet
- Horizontal Condylar AngleDocument2 pagesHorizontal Condylar Angleسلمى صلاح100% (2)
- 2020 Dental CertificateDocument36 pages2020 Dental Certificatebenz cadiongNo ratings yet
- Extraction of TeethDocument84 pagesExtraction of TeethAkram Thabet0% (1)
- Oral Health Examination Record For Teachers and Non-Teaching PersonnelDocument3 pagesOral Health Examination Record For Teachers and Non-Teaching PersonnelDaisy's Home Cooking100% (6)
- Oral Health Examination Record For TNTPDocument1 pageOral Health Examination Record For TNTPJellyn Cadorna100% (1)
- Root Canal Preparation Techniques - Endodontic TreatmentDocument1 pageRoot Canal Preparation Techniques - Endodontic TreatmentWeaam SharafNo ratings yet
- Dental Health CardDocument3 pagesDental Health Cardodessa delos santos100% (1)
- Dental Chart BSAVADocument1 pageDental Chart BSAVAFabiola CabreraNo ratings yet
- Oral Health Examination Record For Teaching and Non Teaching PersonnelDocument1 pageOral Health Examination Record For Teaching and Non Teaching PersonnelAda RicanaNo ratings yet
- Department of Education: Republic of The PhilippinesDocument1 pageDepartment of Education: Republic of The PhilippinesLicca ArgallonNo ratings yet
- DENTAL FORM Teaching and Non Teaching 2Document2 pagesDENTAL FORM Teaching and Non Teaching 2Connie JusosNo ratings yet
- Oral Health Examination RecordDocument1 pageOral Health Examination RecordJefrey N. Gonzales100% (1)
- Dental Health Record Teaching and Non-Teaching Personnel: Index: DMFTDocument2 pagesDental Health Record Teaching and Non-Teaching Personnel: Index: DMFTEmerson NunezNo ratings yet
- Oral Health Examination RecordDocument2 pagesOral Health Examination Recordeugene.camahinNo ratings yet
- UHS Dental Examination Form PDFDocument1 pageUHS Dental Examination Form PDFReaStephanieCidNo ratings yet
- Oral Health Examination Record For Teaching and Non-Teaching PersonnelDocument6 pagesOral Health Examination Record For Teaching and Non-Teaching PersonnelCarmela BlanquerNo ratings yet
- Dental BHSS 2019Document1 pageDental BHSS 2019roulette laypNo ratings yet
- DENTAL FORM T and NTPDocument2 pagesDENTAL FORM T and NTPTalaba ElementaryNo ratings yet
- Dental Form: Deciduous Maxillary TeethDocument1 pageDental Form: Deciduous Maxillary TeethBianca GermarNo ratings yet
- FDI - Functional Analysis No Doppler ExaminationDocument3 pagesFDI - Functional Analysis No Doppler ExaminationPP MulayNo ratings yet
- Dental Record SampleDocument2 pagesDental Record SampleregieNo ratings yet
- Form 1 Dental RecordDocument2 pagesForm 1 Dental RecordMaico Reyes50% (2)
- Insurance LoanDocument1 pageInsurance LoanshamasNo ratings yet
- DM DFU Foot Assessment Form DraftDocument3 pagesDM DFU Foot Assessment Form DraftikhlaslivingNo ratings yet
- Intake Forms 2020Document5 pagesIntake Forms 2020api-624857223No ratings yet
- Dental Certificate 2010 Palaro CorrectedDocument2 pagesDental Certificate 2010 Palaro CorrectedYuri VillanuevaNo ratings yet
- Dental Examination Record FormDocument2 pagesDental Examination Record FormNinoslav MladenovicNo ratings yet
- Dental Examination Record FormDocument2 pagesDental Examination Record FormNurse AnnNo ratings yet
- Incident Form, NotesDocument16 pagesIncident Form, NotesIshan IqbalNo ratings yet
- Dental Health Record1Document2 pagesDental Health Record1Gerald Angelo AvendañoNo ratings yet
- Simulation Request Form: Copy Films Dr.'s Box OutsideDocument1 pageSimulation Request Form: Copy Films Dr.'s Box Outsiderobinsc7No ratings yet
- Dental Record FormDocument1 pageDental Record FormadoptifyNo ratings yet
- Dental Status/caries Recording Form: o M B D L o M B D LDocument1 pageDental Status/caries Recording Form: o M B D L o M B D LAnggia GebNo ratings yet
- 2020 Dental-CertificateDocument2 pages2020 Dental-CertificateTino SalabsabNo ratings yet
- Hansen Helicopters - CMM25 60 12 - KSE 35 - REV 10Document106 pagesHansen Helicopters - CMM25 60 12 - KSE 35 - REV 10Exzy EditNo ratings yet
- New Referral Form Sheet1Document2 pagesNew Referral Form Sheet1rebklineNo ratings yet
- Laporan KesehatanDocument1 pageLaporan KesehatanyusviaNo ratings yet
- Dental Health Record Blank SheetDocument1 pageDental Health Record Blank SheetMichael JohnNo ratings yet
- Companion Animal FormDocument2 pagesCompanion Animal FormGabriela GuerraNo ratings yet
- GCS Assessment Aid PortugueseDocument1 pageGCS Assessment Aid PortugueseYasmin RamosNo ratings yet
- Intra-Operative Nurse's RecordDocument2 pagesIntra-Operative Nurse's RecordAnna Margarett Mutia CaballarNo ratings yet
- 2020 Dental-CertificateDocument36 pages2020 Dental-Certificatebenz cadiongNo ratings yet
- BE INDEX For TutorialDocument1 pageBE INDEX For TutorialCollege ITNo ratings yet
- Dental Health Record: Department of EducationDocument2 pagesDental Health Record: Department of EducationJosie A. FranciscoNo ratings yet
- Health Card ElemDocument4 pagesHealth Card ElemBernadette Sambrano EmbienNo ratings yet
- Bellows-Enclosed Shape RFQDocument2 pagesBellows-Enclosed Shape RFQinfoNo ratings yet
- URI CombinedDocument2 pagesURI CombineddocschneidNo ratings yet
- Dental Requirements For 4th StageDocument7 pagesDental Requirements For 4th StageDt omarNo ratings yet
- Dental Requirements For 4th StageDocument7 pagesDental Requirements For 4th StageDt omarNo ratings yet
- Dental Requirements For 4th StageDocument7 pagesDental Requirements For 4th StageDt omarNo ratings yet
- 2020 - Dental Certificate LATESTDocument1 page2020 - Dental Certificate LATESTLeonimar duqueNo ratings yet
- Dental Certificate 2010 PalaroDocument1 pageDental Certificate 2010 PalaroERDA BUENAFENo ratings yet
- Dental Certificate 2010 PalaroDocument2 pagesDental Certificate 2010 Palarogtunida100% (1)
- Medical and Dental Form PPDocument8 pagesMedical and Dental Form PPKim MojicaNo ratings yet
- Bar Cutting ChecklistDocument1 pageBar Cutting ChecklistRosli Bin Abdul Shukor100% (1)
- Weekly Vehicle Check FormDocument1 pageWeekly Vehicle Check FormArsalan KhanNo ratings yet
- Ilocos Sur Provincial Hospital-Gabriela Silang: Republic of The Philippines Province of Ilocos Sur Vigan CityDocument1 pageIlocos Sur Provincial Hospital-Gabriela Silang: Republic of The Philippines Province of Ilocos Sur Vigan CityRyrey Abraham PacamanaNo ratings yet
- Student Agreement /contract: GradeDocument2 pagesStudent Agreement /contract: GradeLinet PerlasNo ratings yet
- Principles of Cavity Preparation LECDocument2 pagesPrinciples of Cavity Preparation LECKen HoiNo ratings yet
- Health6 q1 Mod1 Personalhealthissuesandconcern v1Document23 pagesHealth6 q1 Mod1 Personalhealthissuesandconcern v1Lhen YanzonNo ratings yet
- Learning Material Topic 9 Oral Hygiene and Denture CareDocument6 pagesLearning Material Topic 9 Oral Hygiene and Denture CareUbay SegaNo ratings yet
- 32670052-USX-1904 Xive Product Catalog - LRDocument112 pages32670052-USX-1904 Xive Product Catalog - LRPabloNo ratings yet
- 1976 - Creeping Attachment After Free Gingival GraftDocument6 pages1976 - Creeping Attachment After Free Gingival GraftTien Li AnNo ratings yet
- Incorporating The Fundamentals of Patient Risk AssessmentDocument14 pagesIncorporating The Fundamentals of Patient Risk AssessmentMelanie CastroNo ratings yet
- Dentoalveolar Surgery 1 05Document76 pagesDentoalveolar Surgery 1 05I Putu Aditya Putra WirawanNo ratings yet
- Mouth Care For An Unconcious Patient (2201)Document5 pagesMouth Care For An Unconcious Patient (2201)Maggie LiNo ratings yet
- Patient Dentist CommunicationDocument37 pagesPatient Dentist CommunicationbarbacumlaudeNo ratings yet
- Types of Maxillary Major ConnectorsDocument15 pagesTypes of Maxillary Major Connectorsab0maiNo ratings yet
- Teeth, Vessels and Nerves of Oral CavityDocument86 pagesTeeth, Vessels and Nerves of Oral Cavityk20221163No ratings yet
- Is Coronal Restoration More Important Than Root Filling For Ultimate Endodontic Success?Document7 pagesIs Coronal Restoration More Important Than Root Filling For Ultimate Endodontic Success?GowriNo ratings yet
- Chang2004 2Document8 pagesChang2004 2AlfonsoNo ratings yet
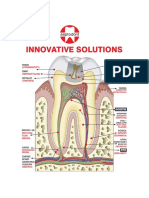
- Innovative Solutions: BiodentineDocument16 pagesInnovative Solutions: BiodentineRavi KumarNo ratings yet
- 4 ImpactionDocument188 pages4 ImpactionD YasIr MussaNo ratings yet
- Toefl Reading Practice (Test of English As A Foreign Language)Document14 pagesToefl Reading Practice (Test of English As A Foreign Language)Adinda Nur FaradilaNo ratings yet
- Senior Project Approval FormDocument2 pagesSenior Project Approval Formapi-592702004No ratings yet
- Int Endodontic J - 2022 - Neelakantan - Present Status and Future Directions Minimally Invasive Root Canal Preparation andDocument27 pagesInt Endodontic J - 2022 - Neelakantan - Present Status and Future Directions Minimally Invasive Root Canal Preparation andGherasimGloriaNo ratings yet
- E SpaceDocument6 pagesE SpaceNicolasFernandezNo ratings yet
- Delivery of Complete Dentures, Prostho Lec 11Document19 pagesDelivery of Complete Dentures, Prostho Lec 11JustDen09100% (4)
- Cogs ShafeesDocument20 pagesCogs ShafeesMariyamNo ratings yet
- Unit 1: Teeth: Grado Superior en Higiene BucodentalDocument11 pagesUnit 1: Teeth: Grado Superior en Higiene BucodentalelenaNo ratings yet
- Muhs Dissertation Title OrthodonticsDocument5 pagesMuhs Dissertation Title OrthodonticsMrunal Doiphode0% (1)