You might also like
- 2020 Dental-CertificateDocument3 pages2020 Dental-CertificateMc DLNo ratings yet
- Dental Health RecordDocument3 pagesDental Health RecordMc DLNo ratings yet
- GESP AY 2021-2022 Forms and AgreementDocument21 pagesGESP AY 2021-2022 Forms and AgreementMPDO LGU San AndresNo ratings yet
- Narrative Report and Documentation SampleDocument7 pagesNarrative Report and Documentation SampleClaire CabactulanNo ratings yet
- Dttes Ok Sa Deped Form C-1Document4 pagesDttes Ok Sa Deped Form C-1jerome100% (2)
- Form 138 E Grade 4 EDITEDDocument3 pagesForm 138 E Grade 4 EDITEDmichaelalangcasNo ratings yet
- Proposed Activities On Women's Month CelebrationDocument3 pagesProposed Activities On Women's Month CelebrationMELISSA PANAGA100% (1)
- Division Action Plan On The Policy and Guidelines On Healthy Food and Beverage Choices SY 2017-2018Document2 pagesDivision Action Plan On The Policy and Guidelines On Healthy Food and Beverage Choices SY 2017-2018mary grace villarenteNo ratings yet
- DO s2019 033Document14 pagesDO s2019 033merNo ratings yet
- Action Plan On Anti Rabies, Tobacco and Tuberculosis AwarenessDocument2 pagesAction Plan On Anti Rabies, Tobacco and Tuberculosis AwarenessMamaanun PS100% (1)
- Ages School Canteen Report 2022 2023Document3 pagesAges School Canteen Report 2022 2023Redempcion P QuiambaoNo ratings yet
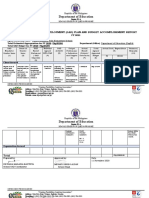
- Department of Education: Annual Gender and Development (Gad) Plan and Budget Accomplishment ReportDocument4 pagesDepartment of Education: Annual Gender and Development (Gad) Plan and Budget Accomplishment ReportReign Magadia BautistaNo ratings yet
- Dental Chart RecordDocument1 pageDental Chart RecordGinaNo ratings yet
- Dental PermitDocument1 pageDental PermitArlene A. PadillaNo ratings yet
- Dental Health ProgramDocument7 pagesDental Health ProgramNomelita LoNo ratings yet
- Aip Rizal 2017Document8 pagesAip Rizal 2017ELMER A. SOCITONo ratings yet
- School Oral Health ProgramDocument24 pagesSchool Oral Health ProgramRinku Roshan100% (1)
- Construction MOA Belen Elementary SchoolDocument1 pageConstruction MOA Belen Elementary SchoolConsuegra Elementary School100% (1)
- Brigada PagbasaDocument1 pageBrigada Pagbasahoney bee100% (1)
- Action Plan GPPDocument3 pagesAction Plan GPPMa Rk AntonioNo ratings yet
- School Annual Gender and Development (Gad) Plan and Budget BP 400/ FY 20Document5 pagesSchool Annual Gender and Development (Gad) Plan and Budget BP 400/ FY 20DAVID TITAN JR.No ratings yet
- Department of Education: Republic of The PhilippinesDocument6 pagesDepartment of Education: Republic of The PhilippinesJohnny ReglosNo ratings yet
- Memo and Letter Double Feed SBFPDocument3 pagesMemo and Letter Double Feed SBFPThamer Jan Son Daulong100% (1)
- Pilot Testing - Letter To BrgyDocument1 pagePilot Testing - Letter To BrgyCara Basnic LaguraNo ratings yet
- District Environmental Quiz Bee Preps StudentsDocument6 pagesDistrict Environmental Quiz Bee Preps StudentsMarjorie MaraveNo ratings yet
- Narrative Report: 2018 District Kindergarten Festival of Talents SY: 2018-2019Document2 pagesNarrative Report: 2018 District Kindergarten Festival of Talents SY: 2018-2019Saima Nasroding100% (1)
- Client Satisfaction Form PDFDocument1 pageClient Satisfaction Form PDFLyn Tabelisma OzarNo ratings yet
- Accomplishment Reports in Gulayan Sa Tahanan ProgramDocument2 pagesAccomplishment Reports in Gulayan Sa Tahanan ProgramNorman LopezNo ratings yet
- ME AttendanceDocument5 pagesME AttendanceKaren Lumiguid JamisolaNo ratings yet
- Acr Orientation Dissemination of Student Code of ConductDocument2 pagesAcr Orientation Dissemination of Student Code of ConductTinTinNo ratings yet
- Narrative Report in School: Department of EducationDocument2 pagesNarrative Report in School: Department of EducationKairuz Demson Aquilam100% (1)
- SignageDocument4 pagesSignageJubilee B. SalvatieraNo ratings yet
- Rizal Central Elementary School Teacher ScheduleDocument1 pageRizal Central Elementary School Teacher ScheduleArianne Kimberlene AmorosoNo ratings yet
- Criteria For Mr. and MSDocument11 pagesCriteria For Mr. and MSQueen Ve NusNo ratings yet
- GP Nomination Form Individual Category - ALS - FinalDocument8 pagesGP Nomination Form Individual Category - ALS - FinalMARY JANE VILLOCERO100% (1)
- Sample PayrollDocument6 pagesSample PayrollDeborah Fajardo ManabatNo ratings yet
- GSIS Members Request Form 2asDocument1 pageGSIS Members Request Form 2asaerosmith_julio6627100% (1)
- RBI Script Sci6 Q1 W4Document8 pagesRBI Script Sci6 Q1 W4Joel Christian Salentes0% (1)
- F-015 CSC-DBM Form No. 1 - Position Description FormDocument8 pagesF-015 CSC-DBM Form No. 1 - Position Description FormPedro NepomucenoNo ratings yet
- Oath TakingDocument4 pagesOath TakingEivra SenreivNo ratings yet
- Aip App PPMPDocument88 pagesAip App PPMPJeurdecel Laborada Castro - MartizanoNo ratings yet
- Senior Citizenand PWDs PLanDocument2 pagesSenior Citizenand PWDs PLanReymond E. Delos ReyesNo ratings yet
- BSP Activity-DesignDocument2 pagesBSP Activity-DesignYamson MillerJr100% (1)
- Department of Education: Republic of The PhilippinesDocument1 pageDepartment of Education: Republic of The Philippinesmichelle100% (1)
- Date:: Noel B. CuadernoDocument4 pagesDate:: Noel B. CuadernoaprilNo ratings yet
- Capitol University Glee Club invited to perform for San Isidro Parish concertDocument2 pagesCapitol University Glee Club invited to perform for San Isidro Parish concertAnonymous 2PeLRG100% (1)
- MATATAG MUSIC and ARTS - CG 2023 - GRADE 4 and 7Document44 pagesMATATAG MUSIC and ARTS - CG 2023 - GRADE 4 and 7Cecile100% (1)
- District of Calumpit North Bulusan Elementary SchoolDocument8 pagesDistrict of Calumpit North Bulusan Elementary Schooldiane ronquillo julianNo ratings yet
- Cover Page - Tugopes Sip 2023-2028Document135 pagesCover Page - Tugopes Sip 2023-2028Joven BasarioNo ratings yet
- Research Proposal Application Form and Endorsement of Immediate SupervisorDocument2 pagesResearch Proposal Application Form and Endorsement of Immediate SupervisorRommel YabisNo ratings yet
- Activity Design For DRRMDocument3 pagesActivity Design For DRRMjrose fay amatNo ratings yet
- School feeding program improves nutritionDocument3 pagesSchool feeding program improves nutritionJoseph NoblezaNo ratings yet
- BP Form 400-A FY 2019: Annual Gender and Development (Gad) Accomplishment ReportDocument4 pagesBP Form 400-A FY 2019: Annual Gender and Development (Gad) Accomplishment ReportMhikez GnalagnasNo ratings yet
- LIVE-IN BKD LEADERSHIP TRAININGDocument3 pagesLIVE-IN BKD LEADERSHIP TRAININGEmily Jamio0% (1)
- New Ict Designation Mam CecilleDocument1 pageNew Ict Designation Mam CecilleAnthony GonzalesNo ratings yet
- Name of School DEPED PROFILING For SDO Cagayan With Staffing ComplementDocument15 pagesName of School DEPED PROFILING For SDO Cagayan With Staffing ComplementLiza EmmanuelleNo ratings yet
- Memo LAS Writing Final EditedDocument4 pagesMemo LAS Writing Final EditedRaquel Bona ViñasNo ratings yet
- San Rafael Elementary School LAC Implementation PlanDocument8 pagesSan Rafael Elementary School LAC Implementation PlanKate Lorraine Dagohoy100% (1)
- PERSONNEL Health CardDocument1 pagePERSONNEL Health Cardarnulyn.garciaNo ratings yet
- Coaching Session For MTs SummitDocument43 pagesCoaching Session For MTs SummitAda RicanaNo ratings yet
- Cagay National High School 2nd Periodical Test in Contemporary Philippine ArtsDocument3 pagesCagay National High School 2nd Periodical Test in Contemporary Philippine ArtsAda Ricana100% (3)
- 3rd Q. Summative 1Document3 pages3rd Q. Summative 1Ada RicanaNo ratings yet
- CPAR Quarter 2 Week 2Document33 pagesCPAR Quarter 2 Week 2Ada RicanaNo ratings yet
- REportingDocument8 pagesREportingAda RicanaNo ratings yet
- Unifying Themes BiologyDocument65 pagesUnifying Themes BiologyAda RicanaNo ratings yet
- Earth and Life Science Week 1Document20 pagesEarth and Life Science Week 1Ada RicanaNo ratings yet
- DLP 4th Quarter Health 9-InjuriesDocument13 pagesDLP 4th Quarter Health 9-InjuriesAda Ricana100% (1)
- TB MasterlistDocument2 pagesTB MasterlistAda RicanaNo ratings yet
- Cpar 12Document28 pagesCpar 12Ada RicanaNo ratings yet
- Brigada Eskwela 2022 Accomplishment ReportDocument2 pagesBrigada Eskwela 2022 Accomplishment ReportAda RicanaNo ratings yet
- MAPEH (Music) G9: Quarter 2Document40 pagesMAPEH (Music) G9: Quarter 2Krisha Tañare-Malate83% (6)
- Teaching Ethics and Professional StandardsDocument12 pagesTeaching Ethics and Professional StandardsAda Ricana100% (1)
- CAGAY NHS-ARH-2022-reportDocument4 pagesCAGAY NHS-ARH-2022-reportAda RicanaNo ratings yet
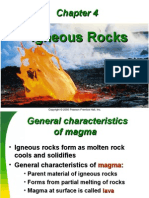
- CH 4-Igneous RocksDocument49 pagesCH 4-Igneous RocksNickolEstradaNo ratings yet
- Anecdotal-Record RPMSModule12Document1 pageAnecdotal-Record RPMSModule12SM MalasagaNo ratings yet
- Narrative Report On Covid 19Document2 pagesNarrative Report On Covid 19Ada RicanaNo ratings yet
- Health QuestionnaireDocument1 pageHealth QuestionnaireAda RicanaNo ratings yet
- Roles of An Emcee 2021Document17 pagesRoles of An Emcee 2021Ada RicanaNo ratings yet
- Creating Interactive Materials Using Scratch Animation - CertificatesDocument2 pagesCreating Interactive Materials Using Scratch Animation - CertificatesAda RicanaNo ratings yet