You might also like
- When Misfortune Becomes Injustice: Evolving Human Rights Struggles for Health and Social Equality, Second EditionFrom EverandWhen Misfortune Becomes Injustice: Evolving Human Rights Struggles for Health and Social Equality, Second EditionNo ratings yet
- Summary of Lessons from the Covid War by Covid Crisis Group: An Investigative ReportFrom EverandSummary of Lessons from the Covid War by Covid Crisis Group: An Investigative ReportNo ratings yet
- Health PolicyDocument15 pagesHealth PolicyJoão Pedro CaetanoNo ratings yet
- 2 RH 2006 For Nurses and Midwifery StsDocument259 pages2 RH 2006 For Nurses and Midwifery StsMiheret GetachewNo ratings yet
- Lisa Forman, The Evolution of The Right To Health in The Shadow of COVID - 19Document4 pagesLisa Forman, The Evolution of The Right To Health in The Shadow of COVID - 19Araceli DabuetNo ratings yet
- Kayla McConnell GOVN 540 Final PaperDocument22 pagesKayla McConnell GOVN 540 Final Paperkayla.mcconnell1No ratings yet
- Haberland, Rogow - 2015 - Sexuality Education Emerging Trends in Evidence and Practice - Journal of Adolescent Health-AnnotatedDocument7 pagesHaberland, Rogow - 2015 - Sexuality Education Emerging Trends in Evidence and Practice - Journal of Adolescent Health-AnnotatedmarencolombiaNo ratings yet
- Kayla PaperDocument11 pagesKayla Paperkayla.mcconnell1No ratings yet
- False Pretenses: The Anti Comprehensive Sexuality EducationDocument23 pagesFalse Pretenses: The Anti Comprehensive Sexuality EducationantondanielvvNo ratings yet
- Gender Health and The 2030 Agenda For SustainableDocument11 pagesGender Health and The 2030 Agenda For Sustainablerichard nagassarNo ratings yet
- Humanrights ChildrenDocument31 pagesHumanrights ChildrenSalvatore RiveraNo ratings yet
- A Review of Women's Intellectual Contribution Under The Bureaucracy in PakistanDocument36 pagesA Review of Women's Intellectual Contribution Under The Bureaucracy in PakistansalmankhataniNo ratings yet
- Social Science & Medicine: Phuong Ngoc Pham, Patrick Vinck, Harvey M. WeinsteinDocument8 pagesSocial Science & Medicine: Phuong Ngoc Pham, Patrick Vinck, Harvey M. WeinsteinIrvhyn Hinostroza AbadNo ratings yet
- A Call For Peoples' Vaccine Against Covid-19 Emmanuel P. FernandezDocument4 pagesA Call For Peoples' Vaccine Against Covid-19 Emmanuel P. FernandezEmman FernandezNo ratings yet
- Teaching Health As A Human Right in The Undergraduate Contexto Challenges and OpportunitiesDocument12 pagesTeaching Health As A Human Right in The Undergraduate Contexto Challenges and OpportunitiesMacarena Astudillo CastroNo ratings yet
- Ail Paper-SummaryDocument9 pagesAil Paper-SummaryKajori BhatnagarNo ratings yet
- Daab 064Document9 pagesDaab 064Getachew YematawNo ratings yet
- FergusonDocument12 pagesFergusontera baapNo ratings yet
- Socialdeterminantsof Health:Anoverviewforthe PrimarycareproviderDocument19 pagesSocialdeterminantsof Health:Anoverviewforthe PrimarycareproviderCarlos Hernan Castañeda RuizNo ratings yet
- The Significance of RH Law and Its OutcomeDocument7 pagesThe Significance of RH Law and Its Outcomeannuj738100% (1)
- PIIS0140673620312551Document3 pagesPIIS0140673620312551kayegi8666No ratings yet
- Chapter One - RH For Africa Medical College - MPHDocument72 pagesChapter One - RH For Africa Medical College - MPHTex ZgreatNo ratings yet
- HRL Reference 5 Dengvaxia and HIV (See Other References)Document2 pagesHRL Reference 5 Dengvaxia and HIV (See Other References)bcarNo ratings yet
- Securing Humans in A Dangerous WorldDocument23 pagesSecuring Humans in A Dangerous WorldAureo de Toledo GomesNo ratings yet
- Duffield and Waddell - Securing Humans in A Dangerous WorldDocument24 pagesDuffield and Waddell - Securing Humans in A Dangerous WorldSandraPatargoNo ratings yet
- FN Health Resource DocumentDocument7 pagesFN Health Resource DocumentEddieNo ratings yet
- SDG and Women EmpowermentDocument14 pagesSDG and Women EmpowermentDeepansha TyagiNo ratings yet
- The Injustice of Covid 19Document2 pagesThe Injustice of Covid 19LYZLEE ANNE VIRGONo ratings yet
- Crisis and Critique On Preparedness, Authoritarianism and The Regulatory StateDocument11 pagesCrisis and Critique On Preparedness, Authoritarianism and The Regulatory StateNikos KarfakisNo ratings yet
- The Moral Imperative of Reproductive Rights, Health, and JusticeDocument8 pagesThe Moral Imperative of Reproductive Rights, Health, and JusticeKepa NeritaNo ratings yet
- Building Health Literacy System CapacityDocument11 pagesBuilding Health Literacy System Capacitynuno ferreiraNo ratings yet
- Human Development & GenderDocument10 pagesHuman Development & GenderProf. Vibhuti PatelNo ratings yet
- Primaryhealthcareandthesocial Determinantsof Health EssentialDocument5 pagesPrimaryhealthcareandthesocial Determinantsof Health Essential98b5jc5hgtNo ratings yet
- Nurse in The National and Global Health Care Delivery SystemDocument9 pagesNurse in The National and Global Health Care Delivery Systemczeremar chanNo ratings yet
- Bioterrorism and Emergency PreparednessDocument3 pagesBioterrorism and Emergency PreparednessRoschelle MiguelNo ratings yet
- Walsh Development As Buen VivirDocument7 pagesWalsh Development As Buen VivirmecdinsueNo ratings yet
- Chapter Four Gender Envionment and Sustianable DevelopmentDocument10 pagesChapter Four Gender Envionment and Sustianable DevelopmentWALLELGNNo ratings yet
- Character Strengths For Post Covid-19 Growth: March 2020Document17 pagesCharacter Strengths For Post Covid-19 Growth: March 2020ravikanth kNo ratings yet
- Covid-19 Pandemic The Imperative For Sta PDFDocument18 pagesCovid-19 Pandemic The Imperative For Sta PDFMAHANTESH GNo ratings yet
- Health Policy and Ethics Forum: The Population Debate: Editor's Note: Public Health Nihilism RevisitedDocument3 pagesHealth Policy and Ethics Forum: The Population Debate: Editor's Note: Public Health Nihilism RevisitedSusy NuryantyNo ratings yet
- Health InfographicsDocument1 pageHealth InfographicsFelicity SanchezNo ratings yet
- Anand Sen 1994. SHD Concepts and PrioritiesDocument7 pagesAnand Sen 1994. SHD Concepts and PrioritiesIndraNo ratings yet
- Discursive StudiesDocument11 pagesDiscursive StudiesSohag LTCNo ratings yet
- Courage, Justice, and Practical Wisdom As Key Virtues in The Era of COVID-19Document22 pagesCourage, Justice, and Practical Wisdom As Key Virtues in The Era of COVID-19Kristian Edsel AmaranteNo ratings yet
- Aging and Human Rights A Rights Based Approach To Social Work With Older AdultsDocument9 pagesAging and Human Rights A Rights Based Approach To Social Work With Older AdultsTaanzNo ratings yet
- Appi Ps 202000725Document6 pagesAppi Ps 202000725Qali IbrahinNo ratings yet
- COVID 19 IS KIL-WPS OfficeDocument2 pagesCOVID 19 IS KIL-WPS Officejg09104350605No ratings yet
- Social Implication of Corruption in Developing CountriesDocument13 pagesSocial Implication of Corruption in Developing CountriesMee MeeNo ratings yet
- Redefining Trauma - Utilizing Restorative Justice To Repair Care SDocument53 pagesRedefining Trauma - Utilizing Restorative Justice To Repair Care SLacatus OlimpiuNo ratings yet
- Who Is Responsible For Mental Health?Document4 pagesWho Is Responsible For Mental Health?Ijahss JournalNo ratings yet
- 2.2 Nussbaum Human Right and Human Capabilities PDFDocument4 pages2.2 Nussbaum Human Right and Human Capabilities PDFgpnasdemsulselNo ratings yet
- A Concept Analysis of Social Justice in Global HealthDocument8 pagesA Concept Analysis of Social Justice in Global HealthHomelo EstoqueNo ratings yet
- A Relational Account of Public Health EthicsDocument14 pagesA Relational Account of Public Health EthicsadrianaNo ratings yet
- Fielding Miller2020Document13 pagesFielding Miller2020ucan fajrinNo ratings yet
- Intervention21120-5570393 152823Document10 pagesIntervention21120-5570393 152823Fauzi MahediNo ratings yet
- Czad 002Document15 pagesCzad 002abeer alrofaeyNo ratings yet
- World Health Organization: by Wendy BraunDocument8 pagesWorld Health Organization: by Wendy BraunAnonymous AvbmJ5JTNo ratings yet
- Martin Health Impact Pyramid PaperDocument10 pagesMartin Health Impact Pyramid Paperapi-653966712No ratings yet
- Technicians of Human Dignity: Bodies, Souls, and the Making of Intrinsic WorthFrom EverandTechnicians of Human Dignity: Bodies, Souls, and the Making of Intrinsic WorthNo ratings yet
- Amalgamation of SocietiesDocument4 pagesAmalgamation of SocietiesKen ChepkwonyNo ratings yet
- Windows 10 100% Disk Usage in Task Manager (SOLVED) - Driver EasyDocument46 pagesWindows 10 100% Disk Usage in Task Manager (SOLVED) - Driver EasyMrinal K MahatoNo ratings yet
- 18.2 Gargallo vs. DOHLE Seafront Crewing August 2016Document10 pages18.2 Gargallo vs. DOHLE Seafront Crewing August 2016French Vivienne TemplonuevoNo ratings yet
- Báo Cáo Nghiên Cứu TMĐTDocument66 pagesBáo Cáo Nghiên Cứu TMĐTAn NguyenNo ratings yet
- AMCTender DocumentDocument135 pagesAMCTender DocumentsdattaNo ratings yet
- The Carta de Jamaica 1815. Simon BolivarDocument16 pagesThe Carta de Jamaica 1815. Simon BolivarOmarNo ratings yet
- India 1885 To 1947Document154 pagesIndia 1885 To 1947KHALIDOO6No ratings yet
- Case Digest 9 October 2020Document5 pagesCase Digest 9 October 2020Gilbert VasquezNo ratings yet
- PAGCOR - Application Form For Gaming SiteDocument4 pagesPAGCOR - Application Form For Gaming SiteJovy JorgioNo ratings yet
- Energy Investor's Guidebook 2013 (Philippines)Document149 pagesEnergy Investor's Guidebook 2013 (Philippines)idoru_m015No ratings yet
- SaraikistanDocument31 pagesSaraikistanKhadija MirNo ratings yet
- NHA V BasaDocument3 pagesNHA V BasaKayeNo ratings yet
- Two-Nation TheoryDocument6 pagesTwo-Nation TheoryAleeha IlyasNo ratings yet
- TTX Human Trafficking With ANSWERS For DavaoDocument7 pagesTTX Human Trafficking With ANSWERS For DavaoVee DammeNo ratings yet
- Samandar Bagh SP College Road, Srinagar: Order No: S14DSEK of 2022Document1 pageSamandar Bagh SP College Road, Srinagar: Order No: S14DSEK of 2022Headmasterghspandrathan GhspandrathanNo ratings yet
- Revenue Regulations No. 7-2012 (Sections 3 To 9 Only)Document43 pagesRevenue Regulations No. 7-2012 (Sections 3 To 9 Only)Charmaine GraceNo ratings yet
- Architect / Contract Administrator's Instruction: Estimated Revised Contract PriceDocument6 pagesArchitect / Contract Administrator's Instruction: Estimated Revised Contract PriceAfiya PatersonNo ratings yet
- Receivable Financing IllustrationDocument3 pagesReceivable Financing IllustrationVatchdemonNo ratings yet
- Chapter 1Document25 pagesChapter 1Annie Basing-at AngiwotNo ratings yet
- Professional Practice of Accounting With AnswerDocument12 pagesProfessional Practice of Accounting With AnswerRNo ratings yet
- On Rural America - Understanding Isn't The ProblemDocument8 pagesOn Rural America - Understanding Isn't The ProblemReaperXIXNo ratings yet
- Tecno Spark Power 2 Misty Grey, 64 GB: Grand Total 9999.00Document2 pagesTecno Spark Power 2 Misty Grey, 64 GB: Grand Total 9999.00Lucky KumarNo ratings yet
- Beta Theta Pi InformationDocument1 pageBeta Theta Pi Informationzzduble1No ratings yet
- Bantolo V CastillonDocument3 pagesBantolo V Castillongoma21No ratings yet
- Tale of Education Policy in BangladeshDocument13 pagesTale of Education Policy in BangladeshSammi bithyNo ratings yet
- Filipino ValuesDocument26 pagesFilipino ValuesDan100% (14)
- 016 - Neda SecretariatDocument4 pages016 - Neda Secretariatmale PampangaNo ratings yet
- Management of TrustsDocument4 pagesManagement of Trustsnikhil jkcNo ratings yet
- Bond Sums For ClassDocument3 pagesBond Sums For ClassShubhangi TerapanthiNo ratings yet
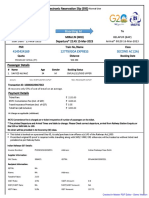
- 12779/GOA EXPRESS Second Ac (2A)Document2 pages12779/GOA EXPRESS Second Ac (2A)Altamash ShaikhNo ratings yet