You might also like
- Laboratory Report: M.D. (Path. & Bact.)Document13 pagesLaboratory Report: M.D. (Path. & Bact.)pateldrash2498No ratings yet
- YGT22541Document13 pagesYGT22541Suraj SheikhNo ratings yet
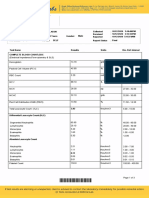
- Complete Blood Count (CBC With E.S.R) .: Investigation Units Result Biological Reference IntervalDocument4 pagesComplete Blood Count (CBC With E.S.R) .: Investigation Units Result Biological Reference Intervalmaryam.ksohrabNo ratings yet
- LPL - Pasricha Diagnostics & Ultrasound ClinicDocument4 pagesLPL - Pasricha Diagnostics & Ultrasound ClinicJohnnieNo ratings yet
- Indian EconomyDocument10 pagesIndian Economyrajputdhruv100No ratings yet
- 02 Mar 2021 PDFDocument8 pages02 Mar 2021 PDFVaibhav RamNo ratings yet
- ReportDocument5 pagesReportpateldrash2498No ratings yet
- LabreportnewDocument16 pagesLabreportnewmirashaik3No ratings yet
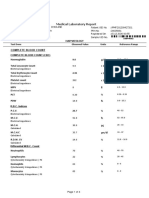
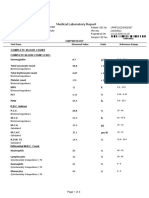
- Medical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWDocument4 pagesMedical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWdhavalNo ratings yet
- Indra Lal - (MRN 1006076) - 1023001085Document3 pagesIndra Lal - (MRN 1006076) - 1023001085yukeonnaNo ratings yet
- SVLT Lab Report DetailsDocument1 pageSVLT Lab Report Detailspancard1098No ratings yet
- Authenticity CheckDocument2 pagesAuthenticity Checkvlande897No ratings yet
- Shailesh 3Document2 pagesShailesh 3Shailesh MeenaNo ratings yet
- ABEEDA BIBI, 25 Year(s) /female: Outdoor-Taken in LabDocument1 pageABEEDA BIBI, 25 Year(s) /female: Outdoor-Taken in LabsaifNo ratings yet
- PatientreportviewinpdfDocument1 pagePatientreportviewinpdfSaba WaheedNo ratings yet
- Department of Hematology Covid-19 Health Checkup (Post Recovery)Document8 pagesDepartment of Hematology Covid-19 Health Checkup (Post Recovery)Geetika GuptaNo ratings yet
- Test Results Units Biological Reference Interval: Haematology Kushal Pro-1 (KP-1) CBC-Comprehensive (20 Paramaters)Document6 pagesTest Results Units Biological Reference Interval: Haematology Kushal Pro-1 (KP-1) CBC-Comprehensive (20 Paramaters)Ravindranatha AnNo ratings yet
- Routine Bio-Chemistry: Renal Function Tests (RFTS)Document1 pageRoutine Bio-Chemistry: Renal Function Tests (RFTS)Muhammad Arif NawazNo ratings yet
- Final: Code/Name & AddressDocument6 pagesFinal: Code/Name & AddresscrypticgarvNo ratings yet
- Investigation Report: Flowcytometry. Carried Out by Sysmex XN-2000 SeriesDocument1 pageInvestigation Report: Flowcytometry. Carried Out by Sysmex XN-2000 SeriesNafis ChowdhuryNo ratings yet
- S65 - PSC Haldwani Diagnostic Centre - Home Visit Sahukara Line, Opp. SS Jeena Base Hospital Nainital, HaldwaniDocument3 pagesS65 - PSC Haldwani Diagnostic Centre - Home Visit Sahukara Line, Opp. SS Jeena Base Hospital Nainital, Haldwanirajasereddy1275No ratings yet
- Ha 2Document3 pagesHa 2Divyansh Singh ChauhanNo ratings yet
- Z021 PDFDocument2 pagesZ021 PDFAditya RudraNo ratings yet
- Med111487409 33864299 118 79600569Document7 pagesMed111487409 33864299 118 79600569Akhil MuraliNo ratings yet
- Detection of Lupus Anticoagulant (LA)Document6 pagesDetection of Lupus Anticoagulant (LA)Esra AllamNo ratings yet
- Laboratory Report: M.D. (Patho) M.D. (Patho) M.D. (Patho)Document2 pagesLaboratory Report: M.D. (Patho) M.D. (Patho) M.D. (Patho)Parth KaravadraNo ratings yet
- Department of Hematology: Blood C/E (Complete, CBC)Document2 pagesDepartment of Hematology: Blood C/E (Complete, CBC)Muhammad UsmanNo ratings yet
- Screenshot 2023-12-19 at 15.34.42Document3 pagesScreenshot 2023-12-19 at 15.34.42yukeonnaNo ratings yet
- Screenshot 2023-12-19 at 15.34.42Document3 pagesScreenshot 2023-12-19 at 15.34.42yukeonnaNo ratings yet
- 37120500696#43440#37120500696#1 - 11 - 2020 12 - 00 - 00 AmDocument2 pages37120500696#43440#37120500696#1 - 11 - 2020 12 - 00 - 00 AmMohammad BolockNo ratings yet
- Nate Ashton Quipot FileDocument1 pageNate Ashton Quipot FileNaughty or NiceNo ratings yet
- CBC Test Report Format Example Sample Template Drlogy Lab ReportDocument2 pagesCBC Test Report Format Example Sample Template Drlogy Lab Reportsa jaNo ratings yet
- WM68Document4 pagesWM68CloudCom TechnologyNo ratings yet
- Wa0002. - 2Document3 pagesWa0002. - 2underdog1246opNo ratings yet
- Complete Blood Picture (CBP), EDTA Whole Blood: Master - SushanthDocument3 pagesComplete Blood Picture (CBP), EDTA Whole Blood: Master - SushanthAbdul MuqeemNo ratings yet
- Fully Automated Lab Accurate Reports Reports Verified by PathologistDocument11 pagesFully Automated Lab Accurate Reports Reports Verified by PathologistBathri NathanNo ratings yet
- Creatinine & CBCDocument4 pagesCreatinine & CBCAira Joy AnyayahanNo ratings yet
- Department of Chemical Pathology: Test Reference Value UnitDocument1 pageDepartment of Chemical Pathology: Test Reference Value UnitMohammad Dayyan KhanNo ratings yet
- Jiyo Healthy Jiyo Wellthy Any Time Package: Complete Blood Count (CBC)Document6 pagesJiyo Healthy Jiyo Wellthy Any Time Package: Complete Blood Count (CBC)Lalit VashistaNo ratings yet
- TestosteroneDocument1 pageTestosteronetiwariharry539No ratings yet
- 3upneaa5qdckn2nonvdn0vouDocument7 pages3upneaa5qdckn2nonvdn0vouNitinNo ratings yet
- Fully Automated Lab Accurate Reports Reports Verified by PathologistDocument9 pagesFully Automated Lab Accurate Reports Reports Verified by PathologistJayshree BawaniyaNo ratings yet
- DHYANSH GANDHI-Male6 Years-44656Document4 pagesDHYANSH GANDHI-Male6 Years-44656Hitesh JainNo ratings yet
- Department of Hematology Comprehensive Full Body Checkup Test Name Result Unit Bio. Ref. IntervalDocument11 pagesDepartment of Hematology Comprehensive Full Body Checkup Test Name Result Unit Bio. Ref. IntervalshyamNo ratings yet
- HematologyDocument5 pagesHematologyDeepak KumarNo ratings yet
- Oliveros, Crystal Enriquez 2053044297Document8 pagesOliveros, Crystal Enriquez 2053044297Peter VukovicNo ratings yet
- R8830560 Srijith 151021193600Document7 pagesR8830560 Srijith 151021193600Tyrion LannisterNo ratings yet
- 5047UH0368065047 552937fDocument16 pages5047UH0368065047 552937fpeter smithNo ratings yet
- Leyva, Miguel Robert Ople 2151182765Document2 pagesLeyva, Miguel Robert Ople 2151182765Therese LeyvaNo ratings yet
- Medical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWDocument4 pagesMedical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWdhavalNo ratings yet
- CBC Test Report Format Example Sample Template Drlogy Lab ReportDocument1 pageCBC Test Report Format Example Sample Template Drlogy Lab ReportThota charanNo ratings yet
- Quillosa, Michelle Remotigue 2251290575Document3 pagesQuillosa, Michelle Remotigue 2251290575michael enriquezNo ratings yet
- Timesh of India PatientDocument24 pagesTimesh of India PatientRE INTERNET CAFENo ratings yet
- Dinesh SainiDocument2 pagesDinesh Sainifadikex618No ratings yet
- Department of Hematology Test Name Result Unit Bio. Ref. IntervalDocument3 pagesDepartment of Hematology Test Name Result Unit Bio. Ref. Intervalaf dNo ratings yet
- Thirumalai N:::: Patient Age / Sex 34 Y / Male BranchDocument6 pagesThirumalai N:::: Patient Age / Sex 34 Y / Male Branchthirumalai narayananNo ratings yet
- Fully Automated Lab Accurate Reports Reports Verified by PathologistDocument15 pagesFully Automated Lab Accurate Reports Reports Verified by PathologistKashishNo ratings yet
- L39 - Discovery Lab: Result UnitDocument3 pagesL39 - Discovery Lab: Result UnitanjnaNo ratings yet
- Vanjaarsveld MelodyM 1111992 PatientReportDocument2 pagesVanjaarsveld MelodyM 1111992 PatientReportmelodyvanjaasveldNo ratings yet
- Reviewer in Forensic Medicine: Melcon S. Lapina, MscrimDocument132 pagesReviewer in Forensic Medicine: Melcon S. Lapina, MscrimMoses VillagonzaloNo ratings yet
- PHC411 - Practical 3 - Oct 2021 - StudentsDocument14 pagesPHC411 - Practical 3 - Oct 2021 - StudentsALISYA SOPHIA MOHAMMAD ABU SHAHID CHRISNo ratings yet
- Blood Pressure ChartDocument5 pagesBlood Pressure ChartAnonymous LiddTaTaZTNo ratings yet
- PULSATILLA From Materia Medica by James Tyler Kent. Homeopathy - PDFDocument10 pagesPULSATILLA From Materia Medica by James Tyler Kent. Homeopathy - PDFpksNo ratings yet
- Fish Physiology 1Document17 pagesFish Physiology 1Shyamol BoseNo ratings yet
- Aldosteronism: Managing YourDocument3 pagesAldosteronism: Managing YourCamille AliNo ratings yet
- Nervous System Worksheet PDFDocument2 pagesNervous System Worksheet PDFMaryechu100% (2)
- Renal Embryology: Jason Ryan, MD, MPHDocument731 pagesRenal Embryology: Jason Ryan, MD, MPHFateh BoulounisNo ratings yet
- Obstructive JaundiceDocument54 pagesObstructive JaundiceJenine Ezra M. Conol50% (2)
- Ijavol 5no 3sep-Dec20161Document161 pagesIjavol 5no 3sep-Dec20161Ayesha JadoonNo ratings yet
- Skin Functions and LayersDocument23 pagesSkin Functions and LayersAnis Samrotul Lathifah100% (2)
- Emotions LectureDocument27 pagesEmotions LectureJennifer Isom Schmidtke, Ph.D.100% (2)
- Factors of Bone Resorption of The Residual Ridge Ortman1962Document12 pagesFactors of Bone Resorption of The Residual Ridge Ortman1962AbdelKhalek BouararaNo ratings yet
- 3.1 Homeostasis in Living ThingsDocument21 pages3.1 Homeostasis in Living ThingsHema LataNo ratings yet
- Case History 33Document4 pagesCase History 33Hida KurticNo ratings yet
- The Cephalic, Oral and Esophageal Phases of The Integrated Response To A MealDocument9 pagesThe Cephalic, Oral and Esophageal Phases of The Integrated Response To A MealpuchioNo ratings yet
- Anatomy Atlas PreviewDocument11 pagesAnatomy Atlas PreviewastrozzNo ratings yet
- Dr. Jyoti Prakash-CASDocument9 pagesDr. Jyoti Prakash-CASshrutiNo ratings yet
- Immunohematology MCQsDocument21 pagesImmunohematology MCQsMeerva El-zein86% (22)
- TMJ and Temporomandibular Joint Disorder: Dr. Soukaina RyalatDocument47 pagesTMJ and Temporomandibular Joint Disorder: Dr. Soukaina RyalatJohan Edward Franklin MarpaungNo ratings yet
- A Dancing Patient: Dr. Ahmed Al MontasirDocument33 pagesA Dancing Patient: Dr. Ahmed Al MontasirMontasir AhmedNo ratings yet
- Sanjeevini Combination Sheet For SSC 9 Blood Pressure LowDocument1 pageSanjeevini Combination Sheet For SSC 9 Blood Pressure LowEduardoNo ratings yet
- Anatomy and Physiology of ThyroidDocument23 pagesAnatomy and Physiology of ThyroidPonnan DasaiyanNo ratings yet
- Disseminated Intravascular Coagulation Concept MapDocument3 pagesDisseminated Intravascular Coagulation Concept MapphoebjaetanNo ratings yet
- Behavioral and Neural Effects of Compassion Medita9onDocument37 pagesBehavioral and Neural Effects of Compassion Medita9onccareemailNo ratings yet
- HHW Biology X PDFDocument9 pagesHHW Biology X PDFNikhil bhatiNo ratings yet
- Increase VolumeDocument31 pagesIncrease VolumeChris Doc RogersNo ratings yet
- Veterinary AcupunctureDocument19 pagesVeterinary AcupuncturekinezildiNo ratings yet
- Primary AldosteronismDocument31 pagesPrimary AldosteronismSteph100% (1)