You might also like
- The Future of Medicare Advantage - McKinseyDocument23 pagesThe Future of Medicare Advantage - McKinseyromainNo ratings yet
- 7 Market Access Trends For 2027Document14 pages7 Market Access Trends For 2027Anshuman BudhirajaNo ratings yet
- Health Insurance Trends 2020 PDFDocument28 pagesHealth Insurance Trends 2020 PDFdrarunoncoNo ratings yet
- 6 Top Trends For Ambulatory Surgery Centers in 2018 PDFDocument3 pages6 Top Trends For Ambulatory Surgery Centers in 2018 PDFJuan A. SanchezNo ratings yet
- Healthcare Payers Pivot Strategies for Telehealth, Reimbursement, Care ManagementDocument5 pagesHealthcare Payers Pivot Strategies for Telehealth, Reimbursement, Care ManagementNitesh LaguriNo ratings yet
- Preparing For The Next Normal Now How Health Systems Can Adopt A Growth Transformation in The COVID 19 WorldDocument8 pagesPreparing For The Next Normal Now How Health Systems Can Adopt A Growth Transformation in The COVID 19 WorldCassiopeia ValenciaNo ratings yet
- DUP 1063 Value Based Care VFINAL 5.11.15Document24 pagesDUP 1063 Value Based Care VFINAL 5.11.15Amare NeonNo ratings yet
- AV Comment Letter On 2024 MA Advance Notice FINALDocument5 pagesAV Comment Letter On 2024 MA Advance Notice FINALArnold VenturesNo ratings yet
- Engaging Commercial Payers On Multi-Payer Alignment:: Key Issues For SIM StatesDocument8 pagesEngaging Commercial Payers On Multi-Payer Alignment:: Key Issues For SIM StatesSHADACNo ratings yet
- VBID 2022 First Eval ReportDocument168 pagesVBID 2022 First Eval ReportCronopios Cortázar BurgosNo ratings yet
- GL 2023 MMB Health Trends Global ReportDocument46 pagesGL 2023 MMB Health Trends Global ReportTânia OliveiraNo ratings yet
- 2015 Health Care Providers Outlook: United StatesDocument5 pages2015 Health Care Providers Outlook: United StatesEmma Hinchliffe100% (1)
- CT Somatom Go Top Brochures Stand Out in Advanced CT Procedures Hood05162002856838 152099932Document56 pagesCT Somatom Go Top Brochures Stand Out in Advanced CT Procedures Hood05162002856838 152099932service iyadMedicalNo ratings yet
- Textbook of Urgent Care Management: Chapter 22, Health Plan ContractingFrom EverandTextbook of Urgent Care Management: Chapter 22, Health Plan ContractingNo ratings yet
- Global Health Care Sector Outlook 2024Document49 pagesGlobal Health Care Sector Outlook 2024Fikri HassanNo ratings yet
- DDocument8 pagesDapi-706911799No ratings yet
- GEP Outlook 2024Document28 pagesGEP Outlook 2024ageNo ratings yet
- What To Expect in Us Healthcare in 2023 and Beyond PDFDocument10 pagesWhat To Expect in Us Healthcare in 2023 and Beyond PDFSowmya MuraliNo ratings yet
- Nejmp 2207415Document4 pagesNejmp 2207415Akram IrmanNo ratings yet
- Engaging Commercial Payers On Multipayer AlignmentDocument8 pagesEngaging Commercial Payers On Multipayer AlignmentSHADACNo ratings yet
- GX LSHC HC Outlook 2019Document41 pagesGX LSHC HC Outlook 2019Saurav Mishra0% (1)
- The Shifting Landscape of The US Healthcare System Through The ACA and Specific InitiativesDocument3 pagesThe Shifting Landscape of The US Healthcare System Through The ACA and Specific InitiativesPhoebe MwendiaNo ratings yet
- 2022.11.16 - Global Insurance Report 2023 Reimagining Life InsuranceDocument26 pages2022.11.16 - Global Insurance Report 2023 Reimagining Life InsuranceMrDorakonNo ratings yet
- The Future of Us Healthcare Whats Next For The Industry Post Covid 19Document13 pagesThe Future of Us Healthcare Whats Next For The Industry Post Covid 19miltechinsightsNo ratings yet
- How Is Health Care Reform Affecting U.S. Health Insurers' Market Opportunities and Risks?Document6 pagesHow Is Health Care Reform Affecting U.S. Health Insurers' Market Opportunities and Risks?api-227433089No ratings yet
- NHS FPX 6008 Assessment 3 Business Case for ChangeDocument8 pagesNHS FPX 6008 Assessment 3 Business Case for Changezadem5266No ratings yet
- Cheat Sheet Series Medicare Part C Medicare AdvantageDocument2 pagesCheat Sheet Series Medicare Part C Medicare AdvantageGirish KaimalNo ratings yet
- Medicare Is Not BankruptDocument3 pagesMedicare Is Not BankruptMustaffah KabelyyonNo ratings yet
- EL Star Ratings White Paper PDF DownloadDocument5 pagesEL Star Ratings White Paper PDF DownloadHarsh VardhanNo ratings yet
- Trends in Healthcare Payments Annual Report 2015 PDFDocument38 pagesTrends in Healthcare Payments Annual Report 2015 PDFAnonymous Feglbx5No ratings yet
- Insurance Sector Outlook For East Africa 2015: Continous ShiftsDocument12 pagesInsurance Sector Outlook For East Africa 2015: Continous ShiftsJonathan MahengeNo ratings yet
- Us Chs MondayMemo 2013healthcare 5Cs 021313Document1 pageUs Chs MondayMemo 2013healthcare 5Cs 021313Subhani ShaikNo ratings yet
- Arnold Ventures Comment On CY2024 MPFS RuleDocument9 pagesArnold Ventures Comment On CY2024 MPFS RuleArnold VenturesNo ratings yet
- Medicare Prescription Drugs: Medical Necessity Meets Fiscal Insanity Cato Briefing Paper No. 91Document12 pagesMedicare Prescription Drugs: Medical Necessity Meets Fiscal Insanity Cato Briefing Paper No. 91Cato InstituteNo ratings yet
- MCO Three-Year Cost ReportDocument28 pagesMCO Three-Year Cost Reporttinareedreporter100% (1)
- US Financial StudyDocument25 pagesUS Financial StudysandeepNo ratings yet
- NHS FPX 6008 Assessment 3 Business Case for ChangeDocument6 pagesNHS FPX 6008 Assessment 3 Business Case for Changefarwaamjad771No ratings yet
- Reshaping Retail Banking For Next Normal PDFDocument13 pagesReshaping Retail Banking For Next Normal PDFarisbudimanNo ratings yet
- An Open Letter To The Administrator For The Centers For Medicare and Medicaid Services (CMS)Document11 pagesAn Open Letter To The Administrator For The Centers For Medicare and Medicaid Services (CMS)Arnold VenturesNo ratings yet
- BCG Next Generation Medical Management - v3Document14 pagesBCG Next Generation Medical Management - v3Sumit Kumar AwkashNo ratings yet
- Millman 2016 Analysis of Medicare IndustryDocument25 pagesMillman 2016 Analysis of Medicare Industrykhyati123No ratings yet
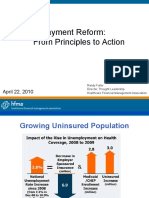
- Payment Reform: From Principles to ActionDocument34 pagesPayment Reform: From Principles to Actionibson045001256No ratings yet
- Mississippi Hospital Association's Comment On Inpatient Psychiatric Rate Update Proposed by CMSDocument6 pagesMississippi Hospital Association's Comment On Inpatient Psychiatric Rate Update Proposed by CMSJonathan AllenNo ratings yet
- White Paper - Utilization Management Through The Lens of Value-Based CareDocument7 pagesWhite Paper - Utilization Management Through The Lens of Value-Based CarevamseeNo ratings yet
- Medicare Revolution: Profiting from Quality, Not QuantityFrom EverandMedicare Revolution: Profiting from Quality, Not QuantityNo ratings yet
- AHIPDocument5 pagesAHIPPeter SullivanNo ratings yet
- How To Fix The Medicare Shared Savings Program: ExecutiveDocument8 pagesHow To Fix The Medicare Shared Savings Program: ExecutiveAnonymous jq2RD2wNNo ratings yet
- Summary, Analysis & Review of Philip Moeller’s Get What’s Yours for MedicareFrom EverandSummary, Analysis & Review of Philip Moeller’s Get What’s Yours for MedicareNo ratings yet
- The Uncertain Road Ahead:: Could Technology Offer Hospitals Relief From Increasing Margin Pressures?Document18 pagesThe Uncertain Road Ahead:: Could Technology Offer Hospitals Relief From Increasing Margin Pressures?Gade NareshNo ratings yet
- The Challenges of Medicaid Expansion Will Limit U.S. Health Insurers' Profitability in The Short TermDocument8 pagesThe Challenges of Medicaid Expansion Will Limit U.S. Health Insurers' Profitability in The Short Termapi-227433089No ratings yet
- Value Based ProgramsDocument8 pagesValue Based ProgramsPremium GeeksNo ratings yet
- December Price Waters ReportDocument20 pagesDecember Price Waters Reportnchc-scribdNo ratings yet
- The ACA's Medicaid Expansion: Michigan Impact State Budgetary Estimates and Other ImpactsDocument8 pagesThe ACA's Medicaid Expansion: Michigan Impact State Budgetary Estimates and Other ImpactsBeverly TranNo ratings yet
- Analysis of Us Health Care PolicyDocument7 pagesAnalysis of Us Health Care Policyapi-520841770No ratings yet
- Hwang Health Care Cost Growth 10 ProfilesDocument38 pagesHwang Health Care Cost Growth 10 ProfilesBruhan KaggwaNo ratings yet
- 2021 Trends For OphthalmologyDocument10 pages2021 Trends For OphthalmologyNaresh SapoliaNo ratings yet
- NHS FPX 6008 Assessment 3 Business Case For ChangeDocument8 pagesNHS FPX 6008 Assessment 3 Business Case For ChangeEmma WatsonNo ratings yet
- PWC ESG Trends 2023Document15 pagesPWC ESG Trends 2023Kanika.SinghNo ratings yet
- Sent Via Federal Erulemaking Portal: The Medicare Payment Advisory Commission. - July 17, 2020Document4 pagesSent Via Federal Erulemaking Portal: The Medicare Payment Advisory Commission. - July 17, 2020Arnold VenturesNo ratings yet
- Letter of Support For ACOs and MSSP NPRM Sign On 09202018Document3 pagesLetter of Support For ACOs and MSSP NPRM Sign On 09202018HLMeditNo ratings yet
- Mapping The Road To Prosperity and Parity For Black and Latino Residents Across America - McKinseyDocument14 pagesMapping The Road To Prosperity and Parity For Black and Latino Residents Across America - McKinseyromainNo ratings yet
- Insights To Impact - A Weekly Business Briefing - McKinseyDocument26 pagesInsights To Impact - A Weekly Business Briefing - McKinseyromainNo ratings yet
- Identifying Value in Family-Owned Businesses - McKinseyDocument10 pagesIdentifying Value in Family-Owned Businesses - McKinseyromainNo ratings yet
- Southeast Asia - Economic Overview Q4 2023 - McKinseyDocument20 pagesSoutheast Asia - Economic Overview Q4 2023 - McKinseyromainNo ratings yet
- The CEO's Secret To Successful Leadership - CEO Excellence Revisited - McKinseyDocument20 pagesThe CEO's Secret To Successful Leadership - CEO Excellence Revisited - McKinseyromainNo ratings yet
- Mgi The Future of Women at Work in Brief July 2019Document2 pagesMgi The Future of Women at Work in Brief July 2019djmadpNo ratings yet
- Financial Data Unbound Discussion Paper June 2021Document36 pagesFinancial Data Unbound Discussion Paper June 2021romainNo ratings yet
- Modeling The Impact of AI On The World Economy September-2018Document64 pagesModeling The Impact of AI On The World Economy September-2018sylodhiNo ratings yet
- Mgi The Rise and Rise of The Global Balance Sheet Full Report VFDocument196 pagesMgi The Rise and Rise of The Global Balance Sheet Full Report VFromainNo ratings yet
- Empty Spaces and Hybrid Places v5Document88 pagesEmpty Spaces and Hybrid Places v5romainNo ratings yet
- Mgi The Future of Women at Work Exec Summary July 2019Document36 pagesMgi The Future of Women at Work Exec Summary July 2019romainNo ratings yet
- Five Insights About Harnessing Data and Ai From Leaders at The FrontierDocument5 pagesFive Insights About Harnessing Data and Ai From Leaders at The FrontierromainNo ratings yet
- Southeast Asia - Economic Overview Q4 2023 - McKinseyDocument20 pagesSoutheast Asia - Economic Overview Q4 2023 - McKinseyromainNo ratings yet
- Mgi The Future of Women at Work in The United KingdomDocument16 pagesMgi The Future of Women at Work in The United KingdomromainNo ratings yet
- What Is Economic InclusionDocument6 pagesWhat Is Economic InclusionromainNo ratings yet
- Gokul Rajaram On Product Thinking and Innovation - McKinseyDocument9 pagesGokul Rajaram On Product Thinking and Innovation - McKinseyromainNo ratings yet
- The Trends Transforming Mobility, Electric Vehicles, Autonomous Driving, and Micromobility - McKinseyDocument14 pagesThe Trends Transforming Mobility, Electric Vehicles, Autonomous Driving, and Micromobility - McKinseyromainNo ratings yet
- Insights To Impact - A Weekly Business Briefing - McKinseyDocument26 pagesInsights To Impact - A Weekly Business Briefing - McKinseyromainNo ratings yet
- Mgi The Rise and Rise of The Global Balance Sheet Full Report VFDocument196 pagesMgi The Rise and Rise of The Global Balance Sheet Full Report VFromainNo ratings yet
- The CEO's Secret To Successful Leadership - CEO Excellence Revisited - McKinseyDocument20 pagesThe CEO's Secret To Successful Leadership - CEO Excellence Revisited - McKinseyromainNo ratings yet
- Rekindling Us Labor Productivity For A New Era VfinalDocument29 pagesRekindling Us Labor Productivity For A New Era VfinalromainNo ratings yet
- Where Is Customer Care in 2024 v2Document8 pagesWhere Is Customer Care in 2024 v2romainNo ratings yet
- Reimagining Economic Growth in Africa AppendixDocument6 pagesReimagining Economic Growth in Africa AppendixromainNo ratings yet
- and MicromobilityDocument14 pagesand MicromobilityromainNo ratings yet
- Destination Zero An Action Plan For Shipping CeosDocument11 pagesDestination Zero An Action Plan For Shipping CeosromainNo ratings yet
- Peak Energy Peak Oil and The Rise of Renewables VFDocument9 pagesPeak Energy Peak Oil and The Rise of Renewables VFRanga ShingteNo ratings yet
- Gokul Rajaram On Product Thinking and Innovation - McKinseyDocument9 pagesGokul Rajaram On Product Thinking and Innovation - McKinseyromainNo ratings yet
- Accelerating Europe Competitiveness 1501 VFDocument13 pagesAccelerating Europe Competitiveness 1501 VFromainNo ratings yet
- Asia On The Cusp of A New Era - FinalDocument46 pagesAsia On The Cusp of A New Era - FinalSiya LimNo ratings yet
- Tendon and Ligament Healing: A New Approach Through Manual TherapyDocument1 pageTendon and Ligament Healing: A New Approach Through Manual TherapyMichael SelvarajNo ratings yet
- The Vibrant Nature of HealthDocument105 pagesThe Vibrant Nature of HealthDr. Peter Fritz Walter100% (4)
- Congestive Heart Failure 1 Concept Map !Document1 pageCongestive Heart Failure 1 Concept Map !Franklin A. Salaum IIINo ratings yet
- Svengali in Arizona - TIME 10-22-1973Document2 pagesSvengali in Arizona - TIME 10-22-1973tonyleontNo ratings yet
- Decontamination of Equipment Environment Policy 5.1Document34 pagesDecontamination of Equipment Environment Policy 5.1Nur Aqilah IsmailNo ratings yet
- ICO International Clinical Guidelines: List of Guidelines AvailableDocument74 pagesICO International Clinical Guidelines: List of Guidelines AvailableOvidiu Rusu100% (1)
- Clinical Pharmacy ServicesDocument39 pagesClinical Pharmacy ServicesDhearara W RizkyNo ratings yet
- Curriculum Vitae: Personal InformationDocument2 pagesCurriculum Vitae: Personal InformationtyasNo ratings yet
- The Use of Moist Exposed Burn Ointment (MEBO) For The Treatment of Burn Wounds: A Systematic ReviewDocument8 pagesThe Use of Moist Exposed Burn Ointment (MEBO) For The Treatment of Burn Wounds: A Systematic ReviewPahang Reforansa PutraNo ratings yet
- Week 1 Module 1 HealthDocument28 pagesWeek 1 Module 1 Healthlucas'No ratings yet
- Principles of Toxicology SummaryDocument19 pagesPrinciples of Toxicology SummaryUrugonda VenumadhavNo ratings yet
- Who HRP e Motive Poster Original 1Document1 pageWho HRP e Motive Poster Original 1Andreina CamachoNo ratings yet
- June 2021Document90 pagesJune 2021SEIYADU IBRAHIM KNo ratings yet
- List of Clinical Medicine Books: Titles Authors Publisher YearDocument13 pagesList of Clinical Medicine Books: Titles Authors Publisher Yearwaqas_xsNo ratings yet
- Kasus Sistem Endokrin 1Document3 pagesKasus Sistem Endokrin 1lilik kartiniNo ratings yet
- Screening For Oral Cancer - Future Prospects, Research and Policy Development For AsiaDocument7 pagesScreening For Oral Cancer - Future Prospects, Research and Policy Development For AsiaCytha Nilam ChairaniNo ratings yet
- Lab 14 Urinary SystemDocument9 pagesLab 14 Urinary Systemzape limitedNo ratings yet
- Marrow Community MedicineDocument136 pagesMarrow Community Medicinesainithin88348No ratings yet
- Complaint LetterDocument4 pagesComplaint Lettereshwari0706No ratings yet
- Trochanteric Bursitis and HomoeopathyDocument5 pagesTrochanteric Bursitis and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- Design and Characterization of Bilayer Tablet of Rifampicin and Isoniazid For Tuberculosis TherapyDocument5 pagesDesign and Characterization of Bilayer Tablet of Rifampicin and Isoniazid For Tuberculosis TherapyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Renr Practice Test 9 FinalDocument12 pagesRenr Practice Test 9 FinalTk100% (2)
- Pathanatomy Unit 1 - Unit 6 Q&ADocument12 pagesPathanatomy Unit 1 - Unit 6 Q&AChris Queiklin0% (1)
- The Perfect ClerkDocument3 pagesThe Perfect ClerkKrystel BatinoNo ratings yet
- Essiac A Native Herbal Cancer Remedy Olsen, Cynthia 9781890941000 Books - Amazon.caDocument1 pageEssiac A Native Herbal Cancer Remedy Olsen, Cynthia 9781890941000 Books - Amazon.cahkvpchdbtpNo ratings yet
- CT - Week 16Document3 pagesCT - Week 16PAOLA LUZ CRUZNo ratings yet
- Set v. Care of Clients With Physiologic and Psychosocial Alterations C (Answers)Document11 pagesSet v. Care of Clients With Physiologic and Psychosocial Alterations C (Answers)Yaj CruzadaNo ratings yet
- Horowitz Taylor A Method of Tapering SSRI Treatment To Mitigate Withdrawal SymptomsDocument17 pagesHorowitz Taylor A Method of Tapering SSRI Treatment To Mitigate Withdrawal SymptomsDonaNo ratings yet
- Progress of Molecular Targeted Therapies For ProstatecancersDocument13 pagesProgress of Molecular Targeted Therapies For ProstatecancersNenad MladenovicNo ratings yet