You might also like
- Tumor Immune Microenvironment in Cancer Progression and Cancer TherapyFrom EverandTumor Immune Microenvironment in Cancer Progression and Cancer TherapyPawel KalinskiNo ratings yet
- 1 s2.0 S2311300617300034 MainDocument5 pages1 s2.0 S2311300617300034 MainDeynarazyAdhiSunjayaNo ratings yet
- Targeted Therapies for Lung CancerFrom EverandTargeted Therapies for Lung CancerRavi SalgiaNo ratings yet
- Nej M 200104053441404Document5 pagesNej M 200104053441404bennyrolandnababanNo ratings yet
- Leptin 1Document9 pagesLeptin 1vestibuleNo ratings yet
- The Potential of Conditionally Replicating AdenovirusDocument1 pageThe Potential of Conditionally Replicating AdenovirusJairo BermúdezNo ratings yet
- Constitutive Transduction of Peptide Transporter and HLA Genes Restores Antigen ProcessingDocument6 pagesConstitutive Transduction of Peptide Transporter and HLA Genes Restores Antigen Processingroyhiranmay94No ratings yet
- COX-2 Inhibitors Decrease Expression of PD-L1 in Colon Tumors and Increase The in Ux of Type I Tumor-In Filtrating LymphocytesDocument8 pagesCOX-2 Inhibitors Decrease Expression of PD-L1 in Colon Tumors and Increase The in Ux of Type I Tumor-In Filtrating LymphocytesAnu ShaNo ratings yet
- Allogeneic Expanded Human Peripheral NK Cells Control Prostate Cancer Growth in a Preclinical Mouse Model of Castration-Resistant Prostate CancerDocument11 pagesAllogeneic Expanded Human Peripheral NK Cells Control Prostate Cancer Growth in a Preclinical Mouse Model of Castration-Resistant Prostate Cancerhoangphuong08101992No ratings yet
- (Kyung Hee, Et Al, 2006) PGDocument4 pages(Kyung Hee, Et Al, 2006) PGWinda AlpiniawatiNo ratings yet
- 1 s2.0 S0360301619310193 MainDocument2 pages1 s2.0 S0360301619310193 MainStem EducationNo ratings yet
- Therapeutic Effects of Lentivirus-Mediated Shrna Targeting of Cyclin D1 in Human Gastric CancerDocument9 pagesTherapeutic Effects of Lentivirus-Mediated Shrna Targeting of Cyclin D1 in Human Gastric CancerBest of MeNo ratings yet
- Antiangiogenic and Antitumoral Effects Mediated by aDocument10 pagesAntiangiogenic and Antitumoral Effects Mediated by aMiss AmyNo ratings yet
- 10 1056@NEJMoa1900574 PDFDocument9 pages10 1056@NEJMoa1900574 PDFGhadah AlyousifNo ratings yet
- TNF-alpha Levels in Serum and Mononuclear Cell Lysate of Nigerian Tuberculosis Patients at DiagnosisDocument5 pagesTNF-alpha Levels in Serum and Mononuclear Cell Lysate of Nigerian Tuberculosis Patients at Diagnosisbanteng wibisonoNo ratings yet
- Anticancer Substances of Mushroom OriginDocument9 pagesAnticancer Substances of Mushroom OriginAKNo ratings yet
- Tenascin-C Promotes Tumor Cell Migration and Metastasis Through Integrin A9b1-Mediated YAP InhibitionDocument12 pagesTenascin-C Promotes Tumor Cell Migration and Metastasis Through Integrin A9b1-Mediated YAP InhibitionSayda DhaouadiNo ratings yet
- Inter-Cellular Nanovesicle Mediated MicroRNA TransferDocument19 pagesInter-Cellular Nanovesicle Mediated MicroRNA Transferanon_579968442No ratings yet
- Paper 3Document11 pagesPaper 3Ying-Chi ChuNo ratings yet
- Cancer Res 1982 Lotzová 2480 8Document10 pagesCancer Res 1982 Lotzová 2480 8BobbyGunarsoNo ratings yet
- Clinical Use of Lentiviral Vectors: Lentivirus BiologyDocument13 pagesClinical Use of Lentiviral Vectors: Lentivirus BiologyKyle MillerNo ratings yet
- Gene Therapy, Cell TherapyDocument3 pagesGene Therapy, Cell TherapyMayuri DuttaNo ratings yet
- Havunen Et Al 2017 Mol Ther OncoDocument10 pagesHavunen Et Al 2017 Mol Ther OncoKudelko MatNo ratings yet
- Immuno TherapyDocument20 pagesImmuno TherapyAttis PhrygiaNo ratings yet
- Ijmm 31 6 1375 PDFDocument6 pagesIjmm 31 6 1375 PDFAlex RogobeteNo ratings yet
- PQ 010391Document6 pagesPQ 010391Ajay KumarNo ratings yet
- Anticancer Activity of Phyllanthus Niruri Linn Extract in Colorectal Cancer Patients A Phase II Clinical TrialDocument5 pagesAnticancer Activity of Phyllanthus Niruri Linn Extract in Colorectal Cancer Patients A Phase II Clinical TrialAndi SaputraNo ratings yet
- Ultrasound-Targeted Microbubble Destruction Mediated Herpes Simplex Virus-Thymidine Kinase Gene Treats Hepatoma in MiceDocument6 pagesUltrasound-Targeted Microbubble Destruction Mediated Herpes Simplex Virus-Thymidine Kinase Gene Treats Hepatoma in MiceIndra17No ratings yet
- tmpD126 TMPDocument9 pagestmpD126 TMPFrontiersNo ratings yet
- Ijcep0007 0602Document9 pagesIjcep0007 0602Deedee RenovaldiNo ratings yet
- Detection of Mutations in EGFR in Circulating Lung-Cancer Cells.Document12 pagesDetection of Mutations in EGFR in Circulating Lung-Cancer Cells.Joonseok ParkNo ratings yet
- Long Noncoding Rna Pvt1 Promotes Stemness and Temozolomide Resistance Through Mir-365/Elf4/Sox2 Axis in GliomaDocument12 pagesLong Noncoding Rna Pvt1 Promotes Stemness and Temozolomide Resistance Through Mir-365/Elf4/Sox2 Axis in GliomaReena SharmaNo ratings yet
- Neuropeptide Y (NPY) Promotes Inflammation-Induced Tumorigenesis by Enhancing Epithelial Cell ProliferationDocument9 pagesNeuropeptide Y (NPY) Promotes Inflammation-Induced Tumorigenesis by Enhancing Epithelial Cell Proliferationcarlos marcelo concha vilcaNo ratings yet
- Cannabinoids Inhibit Tumor AngiogenesisDocument16 pagesCannabinoids Inhibit Tumor AngiogenesisjessicaNo ratings yet
- Hematolrep 03 E2 v2Document3 pagesHematolrep 03 E2 v2772450336No ratings yet
- A Stem Cell Gene Therapy ApproachDocument1 pageA Stem Cell Gene Therapy ApproachJairo BermúdezNo ratings yet
- Oncolytic PresentationDocument10 pagesOncolytic PresentationIceyfloesNo ratings yet
- Zeng 2013Document7 pagesZeng 2013angela_karenina_1No ratings yet
- Ernst - KDM4C in JAK2-Mutated Neoplasms, Leukemia, 2022Document7 pagesErnst - KDM4C in JAK2-Mutated Neoplasms, Leukemia, 2022Beatriz Garcia RiartNo ratings yet
- Gene Therapy Clinical Trials Worldwide To 2017 An UpdateDocument16 pagesGene Therapy Clinical Trials Worldwide To 2017 An UpdateLeonardo Sandi SalazarNo ratings yet
- Overcoming A Positive Crossmatch in Living-Donor Kidney TransplantationDocument7 pagesOvercoming A Positive Crossmatch in Living-Donor Kidney TransplantationPratik TripathiNo ratings yet
- New England Journal Medicine: The ofDocument10 pagesNew England Journal Medicine: The ofmayracppNo ratings yet
- In Vitro Properties of Leukocyte Dialysates Containing Transfer FactorDocument6 pagesIn Vitro Properties of Leukocyte Dialysates Containing Transfer FactorijposadaaNo ratings yet
- Reviews: Neutrophil Diversity and Plasticity in Tumour Progression and TherapyDocument19 pagesReviews: Neutrophil Diversity and Plasticity in Tumour Progression and TherapySobek1789No ratings yet
- Cytokine 1Document7 pagesCytokine 1Nela SharonNo ratings yet
- Huang 2005Document6 pagesHuang 2005Hector Javier BurgosNo ratings yet
- Exp. Derm.-2008-Di Como-405-11Document7 pagesExp. Derm.-2008-Di Como-405-11Charles J. DiComo, PhDNo ratings yet
- MMP10 NSCLCDocument9 pagesMMP10 NSCLCbhaskarNo ratings yet
- CLINICS 2019 - Adoptive T-Cell Therapy For Solid MalignanciesDocument15 pagesCLINICS 2019 - Adoptive T-Cell Therapy For Solid MalignanciesWilverCarbonelLuyoNo ratings yet
- 10 1126@scitranslmed Aah6510Document14 pages10 1126@scitranslmed Aah6510翁子貽No ratings yet
- 2960 FullDocument7 pages2960 FullNela SharonNo ratings yet
- Zhao 2017Document8 pagesZhao 2017Pamela Guerrero RomeroNo ratings yet
- Cancer - 2004 - Li - Treatment Outcome and Pattern of Failure in 77 Patients With Sinonasal Natural Killer T Cell or T CellDocument10 pagesCancer - 2004 - Li - Treatment Outcome and Pattern of Failure in 77 Patients With Sinonasal Natural Killer T Cell or T Cell2512505993No ratings yet
- Gene Therapy For High-Grade GliomaDocument6 pagesGene Therapy For High-Grade GliomaArh SetiawanNo ratings yet
- Prins Et Al. - 2002 - Irradiated Tumor Cell Vaccine For Treatment of An Established Glioma. II. Expansion of Myeloid Suppressor Cells THDocument10 pagesPrins Et Al. - 2002 - Irradiated Tumor Cell Vaccine For Treatment of An Established Glioma. II. Expansion of Myeloid Suppressor Cells THJoeyOrpillaNo ratings yet
- 15-Li Chen (531-538)Document8 pages15-Li Chen (531-538)Nguyễn Thanh TùngNo ratings yet
- NEJMoa 074306Document10 pagesNEJMoa 074306monamustafaNo ratings yet
- Extracellular Nucleotides As Novel, Underappreciated Pro-Metastatic Factors That Stimulate Purinerhuman LuDocument15 pagesExtracellular Nucleotides As Novel, Underappreciated Pro-Metastatic Factors That Stimulate Purinerhuman LuLeonel LedezmaNo ratings yet
- Plos One Lmp1Document23 pagesPlos One Lmp1Karol BalsecaNo ratings yet
- Activity 1 - Secret Codon Write A Message in DNA!: MaterialsDocument3 pagesActivity 1 - Secret Codon Write A Message in DNA!: MaterialsJK De GuzmanNo ratings yet
- Proteins Explained: Their Structure, Functions and Essential Amino AcidsDocument5 pagesProteins Explained: Their Structure, Functions and Essential Amino AcidsPaula EdanoNo ratings yet
- Cytotoxic Effects of Ultra-Diluted Remedies On Breast Cancer CellsDocument9 pagesCytotoxic Effects of Ultra-Diluted Remedies On Breast Cancer CellsAPH - Associação Portuguesa de Homeopatia (repositório 2008-15)100% (4)
- A General Biology I Q1M1.2Document26 pagesA General Biology I Q1M1.2Queng Eledia0% (1)
- The S phase is the period of the cell cycle during interphase when DNA replication occurs. The cell makes an identical copy of its DNADocument53 pagesThe S phase is the period of the cell cycle during interphase when DNA replication occurs. The cell makes an identical copy of its DNAHonleth Jheney MamarilNo ratings yet
- STD 9 CHP 5 WorksheetDocument3 pagesSTD 9 CHP 5 WorksheetSarwan KumarNo ratings yet
- DNA Barcoding - Parasites and Vectors: Dan MasigaDocument21 pagesDNA Barcoding - Parasites and Vectors: Dan MasigavaidyamNo ratings yet
- BiophysicsMolecularTechniques PDFDocument116 pagesBiophysicsMolecularTechniques PDFAnwesha BoseNo ratings yet
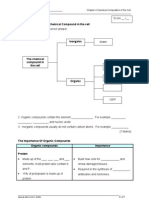
- WORKSHEET 4.2 The Chemical Compound in The CellDocument4 pagesWORKSHEET 4.2 The Chemical Compound in The Cellmira bonzay100% (1)
- Proteins and Denaturing AgentsDocument5 pagesProteins and Denaturing AgentsAbdulrahman Nabil MohammedNo ratings yet
- TranscriptionDocument20 pagesTranscriptionlordniklausNo ratings yet
- Prokaryote Vs Eukaryote WorksheetDocument2 pagesProkaryote Vs Eukaryote WorksheetTaylor50% (2)
- CytologyDocument8 pagesCytologyKin Long Chris WongNo ratings yet
- Cell Membrane Structure & FunctionsDocument2 pagesCell Membrane Structure & FunctionsKim Antonette50% (2)
- Transcription and TranslationDocument2 pagesTranscription and TranslationMary Rose Bobis VicenteNo ratings yet
- Hhmi Cell Cycle and Cancer - CompletedDocument3 pagesHhmi Cell Cycle and Cancer - CompletedAbel89% (9)
- Cell Biology: The Building Blocks of LifeDocument76 pagesCell Biology: The Building Blocks of LifeDave Arthur Robledo100% (11)
- Blood Clotting CascadeDocument10 pagesBlood Clotting CascadeAnonymous PaHej7KNo ratings yet
- Earth Science SOL Review - New One Answer KeyDocument30 pagesEarth Science SOL Review - New One Answer KeyXiandan AyjNo ratings yet
- Genetically Modified Apples Prevent BrowningDocument40 pagesGenetically Modified Apples Prevent BrowningBernardNo ratings yet
- Relationship between cell biology and biochemistryDocument8 pagesRelationship between cell biology and biochemistryLydia OctaviaNo ratings yet
- Journal of BiotechnologyDocument5 pagesJournal of BiotechnologyNur AzizahNo ratings yet
- General Principles of Cell OrganisationDocument3 pagesGeneral Principles of Cell Organisation22194No ratings yet
- Bacillus lipopeptides: versatile weapons against plant diseasesDocument11 pagesBacillus lipopeptides: versatile weapons against plant diseasesjazminNo ratings yet
- Monoclonal AntibodiesDocument14 pagesMonoclonal AntibodiesGAJENDRA RATHORNo ratings yet
- Short Tandem Repeats (STR) in Cattle Genomics and BreedingDocument21 pagesShort Tandem Repeats (STR) in Cattle Genomics and BreedingDušica Ostojić AndrićNo ratings yet
- Gel Electophoresis Simulation: Lab: Simulating ElectrophoresisDocument5 pagesGel Electophoresis Simulation: Lab: Simulating ElectrophoresisDaniel CondreayNo ratings yet
- Ch02 Test Bank For Modern Blood Banking and Transfusion Practices by Denise HarmenDocument6 pagesCh02 Test Bank For Modern Blood Banking and Transfusion Practices by Denise HarmenAJNo ratings yet
- Cell Organeeles IDocument7 pagesCell Organeeles ISaumya GopalNo ratings yet
- Ch4 Enzymes and Metabolism: Multiple-Choice QuestionsDocument4 pagesCh4 Enzymes and Metabolism: Multiple-Choice QuestionsmelNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)