You might also like
- Student Guide: Cell Respiration - HS Handbook and STEM Case: ATP OurDocument4 pagesStudent Guide: Cell Respiration - HS Handbook and STEM Case: ATP OurAurora KongNo ratings yet
- CC - Liver FunctionDocument5 pagesCC - Liver FunctionOrhan AsdfghjklNo ratings yet
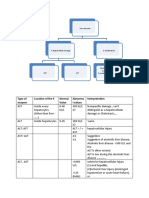
- Type of Enzyme Location of The E Normal Value Abnorma L Values InterpretationDocument4 pagesType of Enzyme Location of The E Normal Value Abnorma L Values InterpretationvisiniNo ratings yet
- Laboratory MedicineDocument17 pagesLaboratory MedicineShrests SinhaNo ratings yet
- Aplikasi Pemeriksaan EnzimDocument25 pagesAplikasi Pemeriksaan EnzimBaiq NashaNo ratings yet
- Amylase, Lipase, LDH, Trop I (Tabulated)Document9 pagesAmylase, Lipase, LDH, Trop I (Tabulated)maja.amora.swuNo ratings yet
- Lecture Clinical EnzymologyDocument30 pagesLecture Clinical Enzymologychocoholic potchi100% (8)
- Extracted Pages From Arneson - Clinical Chemistry-A LaboratDocument6 pagesExtracted Pages From Arneson - Clinical Chemistry-A Laboratastri yul fitrianaNo ratings yet
- 060 CLIN+PATH+43s Liver+Function+TestDocument43 pages060 CLIN+PATH+43s Liver+Function+TestMSKCNo ratings yet
- Class-14 - Plasma Lipoproteins - EnzymesDocument39 pagesClass-14 - Plasma Lipoproteins - EnzymesAyi FurqonNo ratings yet
- (CL8) Enzymes in MedicineDocument27 pages(CL8) Enzymes in MedicineManusha SelvarajooNo ratings yet
- كيمياء سريرية المحاضرة 2Document19 pagesكيمياء سريرية المحاضرة 2MohamedErrmaliNo ratings yet
- Liver Function Tests LFTsDocument4 pagesLiver Function Tests LFTsDr-Dalya ShakirNo ratings yet
- AST and ALTDocument7 pagesAST and ALTTrisha NavarceNo ratings yet
- Clinical EnzymologyDocument23 pagesClinical EnzymologyKishore KaranNo ratings yet
- Validation & Interpretation of Hepatitis Testing Results MF18092022Document90 pagesValidation & Interpretation of Hepatitis Testing Results MF18092022Laila NihayaNo ratings yet
- Clinical Chemistry Clinical Enzymology - Liver Enzymes: Enzyme Description & Function Clinical Significance AnalysisDocument4 pagesClinical Chemistry Clinical Enzymology - Liver Enzymes: Enzyme Description & Function Clinical Significance AnalysisWynlor AbarcaNo ratings yet
- CC2 LecDocument143 pagesCC2 Lechinata shoyoNo ratings yet
- Boyd1983 PDFDocument16 pagesBoyd1983 PDFRoberto GarceteNo ratings yet
- Ast CPDocument4 pagesAst CPLAB. GATOT SUBROTONo ratings yet
- Chem-Dr - Zainab-Liver Enzymes-Lab 3Document16 pagesChem-Dr - Zainab-Liver Enzymes-Lab 3gmpcbpzdysNo ratings yet
- Liver Function Tests (LFTS) : March 2010Document4 pagesLiver Function Tests (LFTS) : March 2010lavanyaNo ratings yet
- Pemeriksaan Fungsi HatiDocument46 pagesPemeriksaan Fungsi HatiNadyaWevtNo ratings yet
- Aspartate Amino TransferaseDocument2 pagesAspartate Amino TransferaseMwebesa GeraldNo ratings yet
- L8 - Hepatic EnzymesDocument30 pagesL8 - Hepatic Enzymesyouservezeropurpose113No ratings yet
- CC1 Lab Fin V2Document22 pagesCC1 Lab Fin V2Melody PardilloNo ratings yet
- Liver Function Tests (LFTS) : Laboratory InsightsDocument3 pagesLiver Function Tests (LFTS) : Laboratory InsightsmahithNo ratings yet
- Transaminases or Aminotransferases: 1. ObjectiveDocument8 pagesTransaminases or Aminotransferases: 1. ObjectiveSeng HongNo ratings yet
- Approach To Abnormal Liver Enzymes Whitepaper TI 07106Document6 pagesApproach To Abnormal Liver Enzymes Whitepaper TI 07106luceroNo ratings yet
- One True KingDocument5 pagesOne True KingQuijano GpokskieNo ratings yet
- Enzyme Notes: Comon Serum Enzyme TestsDocument2 pagesEnzyme Notes: Comon Serum Enzyme Testsالبتول تركستانيNo ratings yet
- Clinicalenzymology 220623200711 Deeb284aDocument8 pagesClinicalenzymology 220623200711 Deeb284aRahul guptaNo ratings yet
- Biochemistry 9 EnzymesDocument11 pagesBiochemistry 9 EnzymesAyan MukherjeeNo ratings yet
- Enzyme Class E.C. Code Assay Reaction Tissue Source Clinical Significance Source of ErrorDocument3 pagesEnzyme Class E.C. Code Assay Reaction Tissue Source Clinical Significance Source of ErrorStephen YorNo ratings yet
- 31 Greene Liver LM 428 2017Document59 pages31 Greene Liver LM 428 2017chip_darrisNo ratings yet
- Lecture 33 - Biomarkers: Learning ObjectivesDocument37 pagesLecture 33 - Biomarkers: Learning ObjectivesAustin KellyNo ratings yet
- Cpliver 1Document4 pagesCpliver 1isahNo ratings yet
- Biochemistry EnzymesDocument18 pagesBiochemistry EnzymesGiorgi TamazashviliNo ratings yet
- Toxicol Pathol-2002-Giffen-365-72-2Document8 pagesToxicol Pathol-2002-Giffen-365-72-2Sara MagoNo ratings yet
- CD Hepatitis - Dr. Yapendon 2014Document13 pagesCD Hepatitis - Dr. Yapendon 2014jeccomNo ratings yet
- Liver Function TestsDocument10 pagesLiver Function TestsShijumon KpNo ratings yet
- Liver Function: DRS' NotesDocument13 pagesLiver Function: DRS' NotesVijayabaskaran MNo ratings yet
- Liver Function: DRS' NotesDocument13 pagesLiver Function: DRS' NotesVijayabaskaran MNo ratings yet
- A&P - 3. Neurotransmission (10p)Document10 pagesA&P - 3. Neurotransmission (10p)Gabriel StratulatNo ratings yet
- Clinical EnzymologyDocument38 pagesClinical EnzymologyLloyd Jay LinNo ratings yet
- CC 2 Activity 2Document5 pagesCC 2 Activity 2Valdez Francis ZaccheauNo ratings yet
- Effek Beta-Blocker Pada Sistem Kardiovaskular-Praktikum-1Document54 pagesEffek Beta-Blocker Pada Sistem Kardiovaskular-Praktikum-1Fanny MaulidaNo ratings yet
- The de Ritis Ratio: The Test of TimeDocument14 pagesThe de Ritis Ratio: The Test of TimeMike NundweNo ratings yet
- Urinary Neurotransmitter Testing: Myths and Misconceptions: © 2007 Neuroscience, IncDocument6 pagesUrinary Neurotransmitter Testing: Myths and Misconceptions: © 2007 Neuroscience, IncMarcus Vinícius SouzaNo ratings yet
- Clinical Chemistry Part 2 - Garland Aug 2022Document4 pagesClinical Chemistry Part 2 - Garland Aug 2022DaNi RooTzNo ratings yet
- Liver TestsDocument17 pagesLiver TestsKreshnik HAJDARI100% (1)
- EnzymesDocument5 pagesEnzymesAhmed AlsarrafNo ratings yet
- Manejo Del VómitoDocument4 pagesManejo Del VómitoDennis J RiosNo ratings yet
- CC2 TransDocument12 pagesCC2 TransAnathalea ReyesNo ratings yet
- 11 Gastroenterology LiverDocument29 pages11 Gastroenterology LiverNoelle Grace Ulep BaromanNo ratings yet
- Enzymes in Diagnosis: OutlineDocument4 pagesEnzymes in Diagnosis: Outlineedh labNo ratings yet
- Study Notes HPBDocument34 pagesStudy Notes HPBTony NgNo ratings yet
- GRP 4 Drug StudyDocument24 pagesGRP 4 Drug StudyWinnie Salazar AriolaNo ratings yet
- Practical Clinical Biochemistry: Prepared by Amer AL-HamatiDocument85 pagesPractical Clinical Biochemistry: Prepared by Amer AL-HamatiAmer Al-hamatiNo ratings yet
- Forensic TraumatologyDocument31 pagesForensic TraumatologyZulhida YuniNo ratings yet
- Your Infidelity Will Result To The Treachery of Your Own Health.Document2 pagesYour Infidelity Will Result To The Treachery of Your Own Health.jsemlpzNo ratings yet
- WSDDocument12 pagesWSDIvana SupitNo ratings yet
- Management of Paediatric Traumatic Cataract by Epilenticular Intraocular Lens Implantation: Long-Term Visual Results and Postoperative ComplicationsDocument5 pagesManagement of Paediatric Traumatic Cataract by Epilenticular Intraocular Lens Implantation: Long-Term Visual Results and Postoperative ComplicationsWahyu Tri UtomoNo ratings yet
- PA Tool PortraitDocument13 pagesPA Tool PortraitKSY JanedoeNo ratings yet
- Aquatic Animal Health and Immunology Chap-1-IntroductionDocument41 pagesAquatic Animal Health and Immunology Chap-1-IntroductionTaukir AhmedNo ratings yet
- Psychiatric NursingDocument58 pagesPsychiatric NursingNimrodNo ratings yet
- Placentofagia PDFDocument38 pagesPlacentofagia PDFluispaulohp2No ratings yet
- SCAT6Document10 pagesSCAT6harNo ratings yet
- Ebook Handbook of Structural Heart Interventions PDF Full Chapter PDFDocument67 pagesEbook Handbook of Structural Heart Interventions PDF Full Chapter PDFforest.gertelman418100% (27)
- A Color Atlas of Poultry Diseases by J.L VegadDocument131 pagesA Color Atlas of Poultry Diseases by J.L VegadAbubakar Tahir Ramay95% (63)
- Care of BedriddenDocument20 pagesCare of BedriddenNazar Ka100% (7)
- The Essential Tremor Rating Assessment ScaleDocument5 pagesThe Essential Tremor Rating Assessment ScaleDysprosodos AnomosNo ratings yet
- StomatitisDocument17 pagesStomatitis4A - Hazel Ann G. EspinolNo ratings yet
- 10 Cancer Symptoms Women Shouldnt IgnoreDocument4 pages10 Cancer Symptoms Women Shouldnt IgnoreRavindra DubeyNo ratings yet
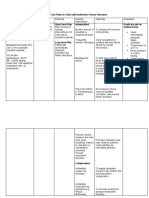
- Nursing Care Plan For Client With Ineffective Tissue PerfusionDocument2 pagesNursing Care Plan For Client With Ineffective Tissue PerfusionThe Right WayNo ratings yet
- Phenylephrine HydrochlorideDocument5 pagesPhenylephrine HydrochlorideSean Amir S. Savellano100% (1)
- Cardiac Approach SurgeryDocument6 pagesCardiac Approach SurgeryAmi NoviantiNo ratings yet
- 2022 Aha-Acc-hfsa HF GuidelineDocument138 pages2022 Aha-Acc-hfsa HF Guidelinekenzo awNo ratings yet
- The Complications of Unprotected SexDocument33 pagesThe Complications of Unprotected Seximi ridleyNo ratings yet
- Homeopathic Remedies: Remedy Traditional Use by Homeopaths NotesDocument8 pagesHomeopathic Remedies: Remedy Traditional Use by Homeopaths NotesAcharla SatyanarayanaNo ratings yet
- Immunobiology Class 8Document24 pagesImmunobiology Class 8viswas andrewsNo ratings yet
- Faktor-Faktor Yang Mempengaruhi Kepatuhan Ibu Hamil Mengkonsumsi Tablet Zat Besi (Fe) Di Wilayah Kerja Puskesmas Tirtajaya Kecamatan Bajuin Tahun 2018Document13 pagesFaktor-Faktor Yang Mempengaruhi Kepatuhan Ibu Hamil Mengkonsumsi Tablet Zat Besi (Fe) Di Wilayah Kerja Puskesmas Tirtajaya Kecamatan Bajuin Tahun 2018Agatha MarcelliaNo ratings yet
- Treatment of Endometriosis in Women Desiring FertilityDocument23 pagesTreatment of Endometriosis in Women Desiring FertilityVaisnavi Muthoovaloo67% (3)
- Astrand TestDocument33 pagesAstrand Testjayant rastogi100% (1)
- 4 Life TestimoniesDocument87 pages4 Life TestimoniesBhavin VoraNo ratings yet
- Vats Bullectomy: Initial Shillong ExperienceDocument21 pagesVats Bullectomy: Initial Shillong ExperiencelmdarlongNo ratings yet
- Pectus ExcavatumDocument16 pagesPectus ExcavatumChristina CluffNo ratings yet
- EndosDocument50 pagesEndosBMT100% (3)