You might also like
- Imaging Modalities For The Classi Fication of Gout: Systematic Literature Review and Meta-AnalysisDocument8 pagesImaging Modalities For The Classi Fication of Gout: Systematic Literature Review and Meta-Analysissiska tiaraNo ratings yet
- Diagnostic Accuracy of Examination Tests For Lateral Elbow Tendinopathy (LET) - A Systematic ReviewDocument10 pagesDiagnostic Accuracy of Examination Tests For Lateral Elbow Tendinopathy (LET) - A Systematic Reviewpatinoomar67No ratings yet
- Dionne Et Al - 2019 - Diagnostic Accuracy of Red Flags CESDocument9 pagesDionne Et Al - 2019 - Diagnostic Accuracy of Red Flags CESMohammad Al AbdullaNo ratings yet
- Questionnaire Tools For The Diagnosis of Carpal Tunnel Syndrome From The Patient HistoryDocument6 pagesQuestionnaire Tools For The Diagnosis of Carpal Tunnel Syndrome From The Patient HistoryMiguelNo ratings yet
- 10 1212@WNL 0000000000006876Document13 pages10 1212@WNL 0000000000006876Besta Arum BelaNo ratings yet
- Diagnostic Accuracy of 5 Dental Pulp Tests: A Systematic Review and Meta-AnalysisDocument9 pagesDiagnostic Accuracy of 5 Dental Pulp Tests: A Systematic Review and Meta-Analysispatel keralNo ratings yet
- Li Et Al. - 2013 - Weighted Youden Index and Its Two-Independent-SampDocument6 pagesLi Et Al. - 2013 - Weighted Youden Index and Its Two-Independent-SampAndrewNo ratings yet
- José Nunes de Alencar Neto Systematic Review and MetaDocument7 pagesJosé Nunes de Alencar Neto Systematic Review and Metayvvs5f9m4mNo ratings yet
- Mus 24761Document5 pagesMus 24761ricardoalfonsoavilaNo ratings yet
- Articulo 4 1Document8 pagesArticulo 4 1franciscoNo ratings yet
- C - SpineDocument10 pagesC - SpineCharly MontielNo ratings yet
- Value of Physical Tests in Diagnosing Cervical Radiculopathy: A Systematic ReviewDocument11 pagesValue of Physical Tests in Diagnosing Cervical Radiculopathy: A Systematic ReviewAndré LuizNo ratings yet
- Thoomes 2017Document11 pagesThoomes 2017alonsoNo ratings yet
- Panoramic Measures For Oral Bone Mass in Detecting Osteoporosis: A Systematic Review and Meta-AnalysisDocument11 pagesPanoramic Measures For Oral Bone Mass in Detecting Osteoporosis: A Systematic Review and Meta-AnalysisRSU DUTA MULYANo ratings yet
- Early Diagnosis and Prevention of Repetitive Strain Injury Induced Carpaltunnel Syndrome Among Computer Users 2471 2701 1000188Document2 pagesEarly Diagnosis and Prevention of Repetitive Strain Injury Induced Carpaltunnel Syndrome Among Computer Users 2471 2701 1000188febby astariNo ratings yet
- A Neurophysiological Grading Scale For Carpal Tunnel SyndromeDocument4 pagesA Neurophysiological Grading Scale For Carpal Tunnel SyndromemikhaelyosiaNo ratings yet
- Clinimetrics of Ultrasound Pathologies in Osteoarthritis: Systematic Literature Review and Meta-AnalysisDocument11 pagesClinimetrics of Ultrasound Pathologies in Osteoarthritis: Systematic Literature Review and Meta-AnalysisArkar SoeNo ratings yet
- Termaat 2005Document11 pagesTermaat 2005OkyôAmêliâNo ratings yet
- Combining Orthopedic Special Tests To ImDocument6 pagesCombining Orthopedic Special Tests To ImVladislav KotovNo ratings yet
- 2019 EULAR SLE CriteriaDocument27 pages2019 EULAR SLE CriteriaLily ChandraNo ratings yet
- Ak Research Doc723062011105245Document19 pagesAk Research Doc723062011105245Alberto BeskowNo ratings yet
- BR J Sports Med-2008-Hegedus-80-92 PDFDocument14 pagesBR J Sports Med-2008-Hegedus-80-92 PDFAnonymous Jx2UvBeteNo ratings yet
- BR J Sports Med-2008-Hegedus-80-92Document14 pagesBR J Sports Med-2008-Hegedus-80-92api-263772125No ratings yet
- Chan Low Sensitivity of Physical Examination FindingsDocument5 pagesChan Low Sensitivity of Physical Examination FindingsxelinenieNo ratings yet
- Contemporary Clinical Trials: ArticleinfoDocument8 pagesContemporary Clinical Trials: ArticleinfoDavy JonesNo ratings yet
- Diagnostic Strategies For The Assessment of Suspected Stable Coronary Artery DiseaseDocument11 pagesDiagnostic Strategies For The Assessment of Suspected Stable Coronary Artery DiseasemamaluNo ratings yet
- N ClassDocument7 pagesN ClassCarlos CENo ratings yet
- SdarticleDocument6 pagesSdarticleClaudia Alejandra Molina SepulvedaNo ratings yet
- Pi Is 0007122605001840Document7 pagesPi Is 0007122605001840Annisa Fitri AnggrainiNo ratings yet
- 08 Can We Safely Apply The Ottawa Ankle Rules To ChildrenDocument3 pages08 Can We Safely Apply The Ottawa Ankle Rules To ChildrenAlejandro Godoy SaidNo ratings yet
- Tunel Del CarpoDocument6 pagesTunel Del CarpojoaquinNo ratings yet
- Freedman 2005Document6 pagesFreedman 2005aliNo ratings yet
- Vereckei Criteria As A Diagnostic Tool Amongst Emergency Medicine Residents To Distinguish Between Ventricular Tachycardia and Supra-Ventricular Tachycardia With AberrancyDocument6 pagesVereckei Criteria As A Diagnostic Tool Amongst Emergency Medicine Residents To Distinguish Between Ventricular Tachycardia and Supra-Ventricular Tachycardia With AberrancyGading AuroraNo ratings yet
- Perkins 2001Document7 pagesPerkins 2001ardyariniNo ratings yet
- Screening Tests For Cushing's Syndrome: Urinary Free Cortisol Role Measured by LC-MS/MSDocument6 pagesScreening Tests For Cushing's Syndrome: Urinary Free Cortisol Role Measured by LC-MS/MSAirene ZulfikarNo ratings yet
- Journal Pone 0160541Document8 pagesJournal Pone 0160541SriMathi Kasi Malini ArmugamNo ratings yet
- Accuracy of Clin. Tests 2020Document12 pagesAccuracy of Clin. Tests 2020Ahmed MortadaNo ratings yet
- Diagnostic Accuracy of Physical Examination Tests of The Ankle-Foot Complex - A Systematic Review.Document11 pagesDiagnostic Accuracy of Physical Examination Tests of The Ankle-Foot Complex - A Systematic Review.CambriaChicoNo ratings yet
- The Memorial SymptomDocument10 pagesThe Memorial SymptomChristine SiburianNo ratings yet
- Evaluación Clínica y Funcional Del HombroDocument9 pagesEvaluación Clínica y Funcional Del HombroLuis Eduardo Cabezas MirandaNo ratings yet
- American Journal of Emergency MedicineDocument5 pagesAmerican Journal of Emergency MedicineMaria teresa salinas merelloNo ratings yet
- Silva 155 166Document12 pagesSilva 155 166Antonio Quintero OtoyaNo ratings yet
- Chong 2015Document5 pagesChong 2015yaniNo ratings yet
- PIIS0003999311007957Document8 pagesPIIS0003999311007957soylahijadeunvampiroNo ratings yet
- UlnarNeur ReaffirmedDocument33 pagesUlnarNeur ReaffirmedEstefania ChaponNo ratings yet
- Screenshot 2024-02-20 at 23.03.52Document6 pagesScreenshot 2024-02-20 at 23.03.52qory fitrahtulNo ratings yet
- A Clinical Prediction Rule For Meniscal Tears in Primary CareDocument7 pagesA Clinical Prediction Rule For Meniscal Tears in Primary CareDeivisonNo ratings yet
- 1547 5654 Article p607Document10 pages1547 5654 Article p607wilsonwqaNo ratings yet
- 8907-Manuscript Clean VersionDocument24 pages8907-Manuscript Clean Versionmoralesjinamay108No ratings yet
- Diagnosis of Carpal Tunnel SyndromeDocument11 pagesDiagnosis of Carpal Tunnel SyndromeMrAppleNo ratings yet
- The Value Added by Electrodiagnostic Testing in The Diagnosis of Carpal Tunnel SyndromeDocument7 pagesThe Value Added by Electrodiagnostic Testing in The Diagnosis of Carpal Tunnel SyndromeSRIJANNo ratings yet
- Prognostic Tools For ....Document15 pagesPrognostic Tools For ....I'am AjhaNo ratings yet
- Triage Tools For Detecting Cervical Spine Injury in Paediatric Trauma PatientsDocument41 pagesTriage Tools For Detecting Cervical Spine Injury in Paediatric Trauma Patientsd69hffy472No ratings yet
- Penugasan STARDDocument14 pagesPenugasan STARDdindaNo ratings yet
- Bmjopen 2021 050711Document10 pagesBmjopen 2021 050711Iveth CoralNo ratings yet
- MeeralamDocument8 pagesMeeralamHyagoNo ratings yet
- Diagnostic Utility of Ultrasonography Versus Nerve Conduction Studies in Mild Carpal Tunnel SyndromeDocument10 pagesDiagnostic Utility of Ultrasonography Versus Nerve Conduction Studies in Mild Carpal Tunnel SyndromeJP ChenNo ratings yet
- Journal of Critical CareDocument8 pagesJournal of Critical CareMuhammad HidayantoNo ratings yet
- Ed Triage ReviewDocument13 pagesEd Triage ReviewTheala RadistaNo ratings yet
- Revisión Sistematica Con Ma de Epicondilitis LateralDocument10 pagesRevisión Sistematica Con Ma de Epicondilitis LateralJorge GámezNo ratings yet
- PHQ-9 GoodDocument9 pagesPHQ-9 GoodJorge GámezNo ratings yet
- Articulo #6Document9 pagesArticulo #6Jorge GámezNo ratings yet
- Articulo #5Document8 pagesArticulo #5Jorge GámezNo ratings yet
- Articulo #4Document9 pagesArticulo #4Jorge GámezNo ratings yet
- Journal of Bodywork & Movement TherapiesDocument11 pagesJournal of Bodywork & Movement TherapiesJorge GámezNo ratings yet
- ESSAYDocument2 pagesESSAYBokNo ratings yet
- Done - EDITED-HOPE1 - q1 - Mod5 - ObservesPersonalSafetyProtocolDocument21 pagesDone - EDITED-HOPE1 - q1 - Mod5 - ObservesPersonalSafetyProtocolVivencio Pascual JrNo ratings yet
- Godbout, J. P., & Glaser, R. (2006) - Stress-Induced Immune Dysregulation. Implications For Wound Healing, Infectious Disease and CancerDocument7 pagesGodbout, J. P., & Glaser, R. (2006) - Stress-Induced Immune Dysregulation. Implications For Wound Healing, Infectious Disease and CancerFranco Paolo Maray-GhigliottoNo ratings yet
- Tungul - Activity 1 Midterms (Pharmacology)Document6 pagesTungul - Activity 1 Midterms (Pharmacology)Ma. Rita Concepcion TungulNo ratings yet
- PDFDocument12 pagesPDFGalih Miftah SgkNo ratings yet
- Feline Immunodeficiency Virus Fibrin Accumulation in Anterior Chamber in Cat With Tripanosomiasis and Feline Immunodeficiency VirusDocument7 pagesFeline Immunodeficiency Virus Fibrin Accumulation in Anterior Chamber in Cat With Tripanosomiasis and Feline Immunodeficiency VirusTsania MahiraNo ratings yet
- Cholecystitis: By: Myla Rojas. BalandraDocument5 pagesCholecystitis: By: Myla Rojas. BalandraMyla Rojas BalandraNo ratings yet
- Trends in Intellectual Property RightsDocument22 pagesTrends in Intellectual Property RightsHana HallajNo ratings yet
- San Jiao Chap 12Document3 pagesSan Jiao Chap 12Bolt VoNo ratings yet
- Executive Technical Report SHCC 2023Document44 pagesExecutive Technical Report SHCC 2023abdelrahim basheerNo ratings yet
- Acute Generalized Exanthematous Pustulosis: Sima HalevyDocument18 pagesAcute Generalized Exanthematous Pustulosis: Sima HalevyDody PrasetyaNo ratings yet
- EndoglukinDocument1 pageEndoglukinPrisaca RădășeniNo ratings yet
- Primary Health Care Systems (Primasys) : Case Study From GeorgiaDocument44 pagesPrimary Health Care Systems (Primasys) : Case Study From GeorgiaTengiz VerulavaNo ratings yet
- Nclex Questions For Fundamentals of NursDocument32 pagesNclex Questions For Fundamentals of NursJrBong SemaneroNo ratings yet
- Individualization of Drug Dosage RegimenDocument34 pagesIndividualization of Drug Dosage RegimenPreethi Iyengar86% (7)
- ANSDocument42 pagesANSRakshan T100% (1)
- Type 2 Diabetes MellitusDocument12 pagesType 2 Diabetes Mellitusjumi jumdailNo ratings yet
- Copd 8 439Document13 pagesCopd 8 439alNo ratings yet
- The Theory of Schussler's Biochemic MethodDocument11 pagesThe Theory of Schussler's Biochemic MethodpankajgoelpnpNo ratings yet
- A.offer D. Furniture: HumanDocument5 pagesA.offer D. Furniture: Humansoyeondan bangtanNo ratings yet
- Clinical Diagnostic Criteria For Dementia AssociatDocument20 pagesClinical Diagnostic Criteria For Dementia AssociatAnderson Cassol DozzaNo ratings yet
- Contoh Final Test Dalam Bahasa InggrisDocument3 pagesContoh Final Test Dalam Bahasa InggrisnuramaliaNo ratings yet
- Chapter 15 StreptococciDocument8 pagesChapter 15 Streptococcinonie jacobNo ratings yet
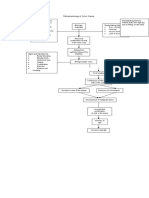
- Pathophysiology of Colon Cancer Predisposing Factors: Etiology: Precipitating Factors: Precipitating FactorsDocument1 pagePathophysiology of Colon Cancer Predisposing Factors: Etiology: Precipitating Factors: Precipitating FactorstatiNo ratings yet
- II-C-1 Gastrointestinal (GI) BleedingDocument4 pagesII-C-1 Gastrointestinal (GI) BleedingDharylle CariñoNo ratings yet
- Medical and Surgical Nursing - IIDocument2 pagesMedical and Surgical Nursing - IIYAMINIPRIYANNo ratings yet
- Policy On Ambulance UseDocument6 pagesPolicy On Ambulance UseMary Jean Gelito89% (9)
- CHN Health Care Process PDFDocument9 pagesCHN Health Care Process PDFKathleen AngNo ratings yet
- Galangal Root: Benefits, Uses, and Side EffectsDocument25 pagesGalangal Root: Benefits, Uses, and Side EffectsEstela BenegildoNo ratings yet
- PRESENTATION ON STI'sDocument52 pagesPRESENTATION ON STI'sEBENEZER OPPONGNo ratings yet