You might also like
- NCEA Numeracy Sample Common Assessment ActivityDocument16 pagesNCEA Numeracy Sample Common Assessment ActivityStuff Newsroom20% (5)
- A Contingency View of Porter's "Generic Strategies"Document12 pagesA Contingency View of Porter's "Generic Strategies"Onos Bunny BenjaminNo ratings yet
- Ex Fix Safe Zone For UE by Fahad AJDocument1 pageEx Fix Safe Zone For UE by Fahad AJAlHasaNo ratings yet
- Unit 3Document4 pagesUnit 3Nhi Nhi100% (2)
- Trial of Endovasculr Treatment of Acute Basilar Artery OcclusionDocument12 pagesTrial of Endovasculr Treatment of Acute Basilar Artery OcclusionVictorNo ratings yet
- ATTENTION TrialDocument12 pagesATTENTION TrialmrabhilekhNo ratings yet
- Thrombectomy 6 To 24 Hours After Stroke With Mismatch Between Deficit and InfarctDocument11 pagesThrombectomy 6 To 24 Hours After Stroke With Mismatch Between Deficit and InfarctMELVIN BURTONNo ratings yet
- Thrombectomy 6 To 24 Hours After Stroke With A Mismatch Between Deficit and InfarctDocument11 pagesThrombectomy 6 To 24 Hours After Stroke With A Mismatch Between Deficit and InfarctDaniela GuariniNo ratings yet
- Intracoronary Autologous CD34+ Stem Cell Therapy For Intractable AnginaDocument8 pagesIntracoronary Autologous CD34+ Stem Cell Therapy For Intractable Anginaasep mahmudNo ratings yet
- Predictors and Outcomes of Shunt-Dependent Hydrocephalus in Patients With Aneurysmal Sub-Arachnoid HemorrhageDocument8 pagesPredictors and Outcomes of Shunt-Dependent Hydrocephalus in Patients With Aneurysmal Sub-Arachnoid HemorrhageNovia AyuNo ratings yet
- Liu 2019 IA Rupture Score Risk of Rebleeding Before TreatmentDocument11 pagesLiu 2019 IA Rupture Score Risk of Rebleeding Before TreatmentSplitBrainNo ratings yet
- Trial of Endovascular Thrombectomy For Large Ischemic StrokesDocument13 pagesTrial of Endovascular Thrombectomy For Large Ischemic StrokesMABEL LUCERO OLARTE JURADONo ratings yet
- Trial of Decompressive Craniectomy For Traumatic Intracranial HypertensionDocument12 pagesTrial of Decompressive Craniectomy For Traumatic Intracranial HypertensionV ANo ratings yet
- Nejmoa2309137 1Document12 pagesNejmoa2309137 1maria espinozaNo ratings yet
- Surveillance IchDocument6 pagesSurveillance IchGabriel Septiana CitraNo ratings yet
- New England Journal Medicine: The ofDocument12 pagesNew England Journal Medicine: The ofBill BerilNo ratings yet
- The Barrow Ruptured Aneurysm Trial - 6-Year ResultsDocument9 pagesThe Barrow Ruptured Aneurysm Trial - 6-Year ResultsJulieta PereyraNo ratings yet
- Fana Alemseged Endovascular Thrombectomy For Basil - 231118 - 114208Document8 pagesFana Alemseged Endovascular Thrombectomy For Basil - 231118 - 114208Luis Guilherme ScalianteNo ratings yet
- DjlnknekjecDocument7 pagesDjlnknekjecRafaelNo ratings yet
- Flat-Head Positioning Increases Cerebral Blood Flow in Anterior Circulation Acute Ischemic Stroke. A Cluster Randomized Phase Iib TrialDocument12 pagesFlat-Head Positioning Increases Cerebral Blood Flow in Anterior Circulation Acute Ischemic Stroke. A Cluster Randomized Phase Iib TrialNaufal HilmiNo ratings yet
- Articles: BackgroundDocument12 pagesArticles: BackgroundJoshua BensonNo ratings yet
- Paper 4Document8 pagesPaper 4Ying-Chi ChuNo ratings yet
- Treatment Stroke AkutDocument3 pagesTreatment Stroke AkutDista Faulam PutriNo ratings yet
- Flat-Head Positioning Increases Cerebral Blood Flow in Anterior Circulation Acute Ischemic Stroke. A Cluster Randomized Phase Iib TrialDocument12 pagesFlat-Head Positioning Increases Cerebral Blood Flow in Anterior Circulation Acute Ischemic Stroke. A Cluster Randomized Phase Iib TrialSelvi PurnamasariNo ratings yet
- Jcen 22 2 78Document7 pagesJcen 22 2 78Aik NoeraNo ratings yet
- S126 FullDocument12 pagesS126 FullIago CarvalhoNo ratings yet
- 6 Antithrombotic Therapy in Patients With Infective EndocarditisDocument12 pages6 Antithrombotic Therapy in Patients With Infective Endocarditisabdeali hazariNo ratings yet
- 1 s2.0 S0929664617300487 MainDocument8 pages1 s2.0 S0929664617300487 MainSuryati HusinNo ratings yet
- 4 - 01-03-07 - J Neurosurg 2007 - Decompressive Hemicraniectomy in Malignant MCA InfarctionDocument7 pages4 - 01-03-07 - J Neurosurg 2007 - Decompressive Hemicraniectomy in Malignant MCA InfarctionThiago Scharth MontenegroNo ratings yet
- Thrombectomy For Stroke at 6 To 16 Hours With Selection by Perfusion ImagingDocument11 pagesThrombectomy For Stroke at 6 To 16 Hours With Selection by Perfusion ImagingLia Ruby FariztaNo ratings yet
- 1 s2.0 S0303846722004218 MainDocument7 pages1 s2.0 S0303846722004218 MainYULISSA FLORES RONDONNo ratings yet
- PCI StrategyDocument14 pagesPCI StrategyJason WinathaNo ratings yet
- Stroke CADISSDocument8 pagesStroke CADISSInge Dackrisna DaudNo ratings yet
- Early Versus Later Anticoagulation For Stroke With Atrial FibrillationDocument11 pagesEarly Versus Later Anticoagulation For Stroke With Atrial Fibrillationguille.1492No ratings yet
- Article LCA Mars 2023Document10 pagesArticle LCA Mars 2023Côme JaubertNo ratings yet
- Trial of Thrombectomy For Stroke With A Large Infarct of Unrestricted Size. N Engl J Med 2024Document13 pagesTrial of Thrombectomy For Stroke With A Large Infarct of Unrestricted Size. N Engl J Med 2024FrancescogmcNo ratings yet
- s12872 019 1096 1Document9 pagess12872 019 1096 1sarahNo ratings yet
- PC ASPECTSDocument11 pagesPC ASPECTSNicolás LozanoNo ratings yet
- Nejmoa 2206606Document10 pagesNejmoa 2206606dipan diratuNo ratings yet
- Artigo HGF Neorologia Maio 2021Document11 pagesArtigo HGF Neorologia Maio 2021Daniela MarinhoNo ratings yet
- Nejmoa 2310392Document11 pagesNejmoa 2310392ENRIQUEFREDNo ratings yet
- Association Between Stress Hyperglycemia and OutcomesDocument9 pagesAssociation Between Stress Hyperglycemia and OutcomesResiden Neuro FK UNPAD - RSHSNo ratings yet
- Spontaneous Vertebral Artery Dissection: Report of 16 Cases: Original ArticleDocument7 pagesSpontaneous Vertebral Artery Dissection: Report of 16 Cases: Original ArticleAyu Yoniko CimplukNo ratings yet
- Meroni2017 CompressedDocument8 pagesMeroni2017 Compresseddayllyn iglesiasNo ratings yet
- Han 2018Document32 pagesHan 2018Isabella EspositoNo ratings yet
- Hemorragia Intracerebral No TraumaticaDocument3 pagesHemorragia Intracerebral No TraumaticaSara CNo ratings yet
- Timing of Surgery For Aneurysmal Subarachnoid Hemorrhage - A Systematic Review and Meta-AnalysisDocument9 pagesTiming of Surgery For Aneurysmal Subarachnoid Hemorrhage - A Systematic Review and Meta-AnalysisJulieta PereyraNo ratings yet
- ClairDocument9 pagesClairMuhammad Imran MirzaNo ratings yet
- Identifying Severe StrokeDocument8 pagesIdentifying Severe StrokekunneiNo ratings yet
- Endoscopia en HDADocument10 pagesEndoscopia en HDASMIBA MedicinaNo ratings yet
- J JCMG 2022 06 015Document12 pagesJ JCMG 2022 06 015Jhon Alexis M ArgoteNo ratings yet
- Thrombectomy Within 8 Hours After Symptom Onset in Ischemic StrokeDocument11 pagesThrombectomy Within 8 Hours After Symptom Onset in Ischemic StrokefontzzNo ratings yet
- 62 2020 Article 898Document7 pages62 2020 Article 898sinamirjaniNo ratings yet
- Articles: BackgroundDocument8 pagesArticles: BackgroundrodribeatsNo ratings yet
- Intracerebeller HemorrhageDocument9 pagesIntracerebeller HemorrhageWenny KalamiNo ratings yet
- Decompressive Craniectomy Vs Craniotomy For Acute SDHDocument11 pagesDecompressive Craniectomy Vs Craniotomy For Acute SDHMary Christina ElsaNo ratings yet
- Conventional Craniotomy Open Access Versus Conservative Treatment in Patients With Minor Spontaneous Intracerebral Hemorrhage in The Basal GangliaDocument10 pagesConventional Craniotomy Open Access Versus Conservative Treatment in Patients With Minor Spontaneous Intracerebral Hemorrhage in The Basal Gangliacah bagusNo ratings yet
- Shock Am IDocument5 pagesShock Am ISantosNo ratings yet
- CME Article January 2017 PDFDocument7 pagesCME Article January 2017 PDFsheila dewantyNo ratings yet
- Hemorragia SubaracnoideaDocument6 pagesHemorragia SubaracnoideaGlessin MurilloNo ratings yet
- Pi Is 0140673623008061Document14 pagesPi Is 0140673623008061Edward ElBuenoNo ratings yet
- Left Atrial Appendage Occlusion During Cadiac Surgery To Prevent StrokeDocument11 pagesLeft Atrial Appendage Occlusion During Cadiac Surgery To Prevent Strokengoc tin nguyenNo ratings yet
- Olavarria2016 PDFDocument5 pagesOlavarria2016 PDFNurul AzmiyahNo ratings yet
- Computing and Visualization for Intravascular Imaging and Computer-Assisted StentingFrom EverandComputing and Visualization for Intravascular Imaging and Computer-Assisted StentingSimone BaloccoNo ratings yet
- Interpretable Surface-Based Detection of Focal Crotical Dysplasias.. A Multi-Centre Epilepsy Lesion Detection StudyDocument13 pagesInterpretable Surface-Based Detection of Focal Crotical Dysplasias.. A Multi-Centre Epilepsy Lesion Detection StudyVictorNo ratings yet
- Trial of Endovasculr Treatment of Acute Basilar Artery OcclusionDocument12 pagesTrial of Endovasculr Treatment of Acute Basilar Artery OcclusionVictorNo ratings yet
- Thomalla, G (2013) - WAKE - UP ACVDocument8 pagesThomalla, G (2013) - WAKE - UP ACVVictorNo ratings yet
- Stroke - Heart Sydrome.. Recent Advances and ChanllengesDocument17 pagesStroke - Heart Sydrome.. Recent Advances and ChanllengesVictorNo ratings yet
- ClearPoint-Measure Goal Evaluation Toolkit PDFDocument25 pagesClearPoint-Measure Goal Evaluation Toolkit PDFarie susantoNo ratings yet
- Enforcement Question 3Document2 pagesEnforcement Question 3Tan Chen WuiNo ratings yet
- ePDQ DirectLink en OriginalDocument24 pagesePDQ DirectLink en Originalsoleone9378No ratings yet
- FE - (D) - Assignment 2Document14 pagesFE - (D) - Assignment 2LAVIN TITARENo ratings yet
- Employment AgreementDocument4 pagesEmployment AgreementRocketLawyer80% (5)
- Diagram Injector (DD) DependenciesDocument21 pagesDiagram Injector (DD) DependenciesHoangNo ratings yet
- Family and Friends G5 - Intensive - LessonPlan - Review - and - Test - 1Document4 pagesFamily and Friends G5 - Intensive - LessonPlan - Review - and - Test - 1Ching OngNo ratings yet
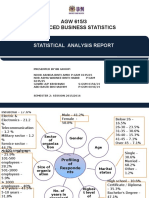
- AGW 615/3 Advanced Business Statistics: Statistical Analysis ReportDocument10 pagesAGW 615/3 Advanced Business Statistics: Statistical Analysis ReportNida AmriNo ratings yet
- ACFrOgBKAsAYs7d-WHbcLJUFPcHKlSnCicVOJdikK-hxHqT K1P-f3EqirdVXGF6hjQNGyEosoB1gRrsKBSmxyFEGItyqjQqKqGUTHdbNuhTGP62PDWEqc1Mi1usKTjGg8IW Xg2y eQUkkWnKIwDocument18 pagesACFrOgBKAsAYs7d-WHbcLJUFPcHKlSnCicVOJdikK-hxHqT K1P-f3EqirdVXGF6hjQNGyEosoB1gRrsKBSmxyFEGItyqjQqKqGUTHdbNuhTGP62PDWEqc1Mi1usKTjGg8IW Xg2y eQUkkWnKIwmarilou schenieferNo ratings yet
- 010 773 Catalogue 22 4 SeparatorsDocument32 pages010 773 Catalogue 22 4 SeparatorskragheorgheNo ratings yet
- Compensation Management & Job EvaluationDocument20 pagesCompensation Management & Job EvaluationSunil Patnaik100% (1)
- Foundry ManualDocument89 pagesFoundry ManualChris LeuteritzNo ratings yet
- Drowning PDFDocument7 pagesDrowning PDFAditya Chandra ForestaNo ratings yet
- FullPaperPublishedine Book OnlineLearningDocument13 pagesFullPaperPublishedine Book OnlineLearningALIF FITRI BIN MOHD JASMINo ratings yet
- Leo Lastimosa ProfileDocument3 pagesLeo Lastimosa ProfileTrey JakosalemNo ratings yet
- FD LMR CatalogoDocument6 pagesFD LMR CatalogoKaren VásconezNo ratings yet
- Wax Patterns in FPDDocument39 pagesWax Patterns in FPDMihaela VasiliuNo ratings yet
- Oracle OBIEE 12c Tuning Guide - v2 PDFDocument60 pagesOracle OBIEE 12c Tuning Guide - v2 PDFnareshreddyguntakaNo ratings yet
- Strategic Management BBSMDocument28 pagesStrategic Management BBSMBasanta Bhetwal33% (3)
- Partnerships: Formation, Operation, and Changes in MembershipDocument39 pagesPartnerships: Formation, Operation, and Changes in MembershipVino VillegasNo ratings yet
- Radiodermatitis India TransDocument14 pagesRadiodermatitis India TransNaufal Fadhil Mufid LazuardiNo ratings yet
- Social Media and Youth Wellbeing ReportDocument33 pagesSocial Media and Youth Wellbeing ReportRayleen WangNo ratings yet
- Dynamic Performance Analysis of Permanent Magnet Hybrid Stepper Motor by Transfer Function Model For Different Design TopologiesDocument7 pagesDynamic Performance Analysis of Permanent Magnet Hybrid Stepper Motor by Transfer Function Model For Different Design TopologiesEEEENo ratings yet
- Printing Inks - Issues, Guidance and RegulationsDocument93 pagesPrinting Inks - Issues, Guidance and RegulationsDinesh RajputNo ratings yet
- Physics Project ON: Full Wave RectifierDocument14 pagesPhysics Project ON: Full Wave RectifierSachin MuruganNo ratings yet
- 2014.03.27 Volume 2 Design ENDocument134 pages2014.03.27 Volume 2 Design ENSalman KaziNo ratings yet