You might also like
- Lactic AcidDocument6 pagesLactic AcidTaha AzNo ratings yet
- The Wound CareDocument51 pagesThe Wound CareIosefina DudeanuNo ratings yet
- BurnsDocument1 pageBurnsasdfghjNo ratings yet
- Colorful Grade 1 Writing Practice English WorksheetDocument9 pagesColorful Grade 1 Writing Practice English WorksheetLeoni Franc100% (1)
- ACS AMI FacilitatorDocument21 pagesACS AMI FacilitatorPaul Zantua57% (7)
- Birthday QuotesDocument24 pagesBirthday QuotesArniel CatubigNo ratings yet
- Chapter 48 - Skin Integrity and Wound CareDocument13 pagesChapter 48 - Skin Integrity and Wound CareHaji Raji100% (1)
- Skin LesionDocument6 pagesSkin LesionDuchess Juliane Jose MirambelNo ratings yet
- Batch Records HandoDocument39 pagesBatch Records HandoNiranjan SinghNo ratings yet
- Pressure Ulcer Guide 8 08Document1 pagePressure Ulcer Guide 8 08MatthiasX12100% (1)
- Fundamentals of Nursing (Midterm Topic 5)Document5 pagesFundamentals of Nursing (Midterm Topic 5)Manuel, Precious Marie B.No ratings yet
- Skin Integrity & Wound CareDocument108 pagesSkin Integrity & Wound CareRon Ar IcaNo ratings yet
- Pressure UlcersDocument1 pagePressure UlcersnanaNo ratings yet
- Skin Care PowerpointDocument52 pagesSkin Care Powerpointisapatrick812667% (3)
- Wound Classification: Presented by Dr. Karen Zulkowski, D.N.S., RN Montana State UniversityDocument41 pagesWound Classification: Presented by Dr. Karen Zulkowski, D.N.S., RN Montana State UniversityDevasyaNo ratings yet
- Skin Integrity and Wound CareDocument6 pagesSkin Integrity and Wound CareAutumn GarofolaNo ratings yet
- Wound Documentation TipsDocument2 pagesWound Documentation TipsDonna Balch Sardina100% (1)
- PilatesDocument65 pagesPilatesAna MariaNo ratings yet
- Policy and Procedures For Hiring, PromotionsDocument2 pagesPolicy and Procedures For Hiring, PromotionsRazel Ann ElagioNo ratings yet
- Burn InjuryDocument1 pageBurn Injuryalyssafairudz21No ratings yet
- Planets in NakshatrasDocument6 pagesPlanets in Nakshatrasmurthyy55% (11)
- API 510 Study GuideDocument3 pagesAPI 510 Study GuidedanikakaNo ratings yet
- Pressure Ulcer Staging CardDocument2 pagesPressure Ulcer Staging CardMary RiveroNo ratings yet
- NPIAP Staging PosterDocument2 pagesNPIAP Staging PosterDr. Hüseyin ŞAHİNNo ratings yet
- Mercaptans Removal From Gases by Absorption Into Amines and CausticDocument8 pagesMercaptans Removal From Gases by Absorption Into Amines and Causticgopal100% (1)
- Types of BurnsDocument5 pagesTypes of BurnsJheanAlphonsineT.Means100% (2)
- Wound Documentation Tips PDFDocument2 pagesWound Documentation Tips PDFWinnie LiNo ratings yet
- Wound Documentation TipsDocument4 pagesWound Documentation TipsLaura Hernandez100% (1)
- Wound Documentation GuidelinesDocument2 pagesWound Documentation GuidelineslumitransNo ratings yet
- PU Grading ChartDocument1 pagePU Grading ChartvanessapriscilliaNo ratings yet
- International PU Classification 2009Document2 pagesInternational PU Classification 2009metabolismeprotein100% (1)
- Pressure UlcersDocument36 pagesPressure UlcershylenshacNo ratings yet
- Wounds Part OneDocument15 pagesWounds Part Onemei robiwidodoNo ratings yet
- Arianne Bernardo BSN-3B1: Erythema Pain Epidermis Sunburns Blistering Nerve DermisDocument5 pagesArianne Bernardo BSN-3B1: Erythema Pain Epidermis Sunburns Blistering Nerve DermisArianne BernardoNo ratings yet
- I. Skin, Hair and Nails Assessment Skin Assessment Assessment Procedure Normal Findings Abnormal Findings A. InspectionDocument40 pagesI. Skin, Hair and Nails Assessment Skin Assessment Assessment Procedure Normal Findings Abnormal Findings A. InspectionLili M.No ratings yet
- Degree of Burns: CharacteristicsDocument2 pagesDegree of Burns: CharacteristicsAnu TripathiNo ratings yet
- Different UlcersDocument1 pageDifferent UlcersRonilyn Mae AlvarezNo ratings yet
- Bed Sores WoundsDocument2 pagesBed Sores Woundspavni_rao6773No ratings yet
- WOUNDDocument6 pagesWOUNDLouie ParillaNo ratings yet
- Name: Score:: Tomas Claudio Memorial College College of NursingDocument31 pagesName: Score:: Tomas Claudio Memorial College College of NursingOng, IvanNo ratings yet
- Luka Bakar Nov 2017 BanjarmasinDocument52 pagesLuka Bakar Nov 2017 BanjarmasinNovita RidhaNo ratings yet
- Abnormal Findings Part 1Document7 pagesAbnormal Findings Part 1jeaminepalencia23No ratings yet
- Photographs and Descriptions of Pressure UlcersDocument1 pagePhotographs and Descriptions of Pressure UlcersClaire GidoNo ratings yet
- Skin, Hair, Nails & ScalpDocument3 pagesSkin, Hair, Nails & ScalpDanah RosalesNo ratings yet
- Skinhairnail Ass 1Document43 pagesSkinhairnail Ass 1Airene Aquino BusaniaNo ratings yet
- Dela Cruz, J. M4Document8 pagesDela Cruz, J. M4Nelly CruzNo ratings yet
- 4 StagesDocument2 pages4 StagesCandice Maureen Riconalla-ChanNo ratings yet
- NCM101 Assignment SecretarioDocument2 pagesNCM101 Assignment SecretariobeaNo ratings yet
- Decubitus UlcerDocument1 pageDecubitus UlcerAkbarNo ratings yet
- A Wound With Coagulative Necrosis Is Called Burn. A Burn Is A Wound in Which There Is Coagulative Necrosis of The TissueDocument17 pagesA Wound With Coagulative Necrosis Is Called Burn. A Burn Is A Wound in Which There Is Coagulative Necrosis of The Tissuewww nambisons comNo ratings yet
- Pressure Ulcer StagesDocument3 pagesPressure Ulcer Stagesfreemind323No ratings yet
- Burns: Picture of Wound Wound Indicator/descriptor Management Aims Recommended Products Relevant LinksDocument3 pagesBurns: Picture of Wound Wound Indicator/descriptor Management Aims Recommended Products Relevant Linksfrenzie_velocityNo ratings yet
- Skin - AssessmentDocument2 pagesSkin - AssessmentRizaxine LachNo ratings yet
- Kulit-Perubahan Dasar Histologis PrintDocument38 pagesKulit-Perubahan Dasar Histologis PrintWirman RamadhanNo ratings yet
- Bedsores: Eligrace F. Fabian, RNDocument22 pagesBedsores: Eligrace F. Fabian, RNsweetsai05No ratings yet
- Wound Assessment & CareDocument32 pagesWound Assessment & Caresami siddiqNo ratings yet
- Pressure UlcerDocument66 pagesPressure UlcerSwarnkar JayeshNo ratings yet
- Wound Classification and Care 2022 KD LEDGEDocument35 pagesWound Classification and Care 2022 KD LEDGEamandaNo ratings yet
- Pressure Sores & ManagementDocument15 pagesPressure Sores & Managementmupt77No ratings yet
- Decubitus Ulcer / Pressure SoresDocument1 pageDecubitus Ulcer / Pressure SoresMabesNo ratings yet
- Burn IntroDocument2 pagesBurn IntroAllis RubioNo ratings yet
- Skin Care and Management of Pressure UlcerDocument24 pagesSkin Care and Management of Pressure UlcerchellczyNo ratings yet
- Skin Checklist ProcedureDocument6 pagesSkin Checklist ProcedureKristine Angie RamosNo ratings yet
- Chapter 3 - WoundDocument37 pagesChapter 3 - Woundwp6mq5bb25No ratings yet
- Pressure Injuries: RLE Group 4: Iris Khan April Labrador Erika Lorenzana Blaise Lozano JM MatadosDocument17 pagesPressure Injuries: RLE Group 4: Iris Khan April Labrador Erika Lorenzana Blaise Lozano JM MatadosApril Mae Magos LabradorNo ratings yet
- SkinDocument2 pagesSkingwendieNo ratings yet
- Lecture 4 WoundDocument54 pagesLecture 4 WoundVet IrfanNo ratings yet
- Terminologi Lesi KulitDocument4 pagesTerminologi Lesi KulitMariyatul QibthiyyahNo ratings yet
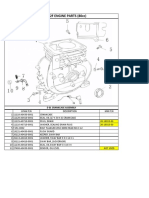
- Lifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblyDocument13 pagesLifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblySean MurrayNo ratings yet
- SRP (305 320) 6MB - MX - enDocument2 pagesSRP (305 320) 6MB - MX - enShamli AmirNo ratings yet
- Anexate IVsolnDocument7 pagesAnexate IVsolnJelena Obrenovic StankovicNo ratings yet
- Executive Compensation: A Presentation OnDocument9 pagesExecutive Compensation: A Presentation On9986212378No ratings yet
- Animal Death Unknown 2010Document57 pagesAnimal Death Unknown 2010Vincent J. CataldiNo ratings yet
- Lab 5 - ReportDocument9 pagesLab 5 - ReportScarlet ErzaNo ratings yet
- Bronce C90700Document2 pagesBronce C90700Luis Enrique CarranzaNo ratings yet
- Dr. Ashraf Sayeed: Department of OphthalmologyDocument49 pagesDr. Ashraf Sayeed: Department of Ophthalmologysaiful haque100% (1)
- Midterm Requirement-Green BuildingDocument7 pagesMidterm Requirement-Green BuildingJo-anne RiveraNo ratings yet
- Interpretacion Curso Cat CoolantDocument39 pagesInterpretacion Curso Cat Coolanthouston machacaNo ratings yet
- Elecsys T4: Cobas e 411 Cobas e 601 Cobas e 602 English System InformationDocument5 pagesElecsys T4: Cobas e 411 Cobas e 601 Cobas e 602 English System InformationIsmael CulquiNo ratings yet
- Method For Emission Spectrometric Analysis of Plain Carbon and Low Alloy Steels Point To Plane Technique (Document8 pagesMethod For Emission Spectrometric Analysis of Plain Carbon and Low Alloy Steels Point To Plane Technique (DiptiNo ratings yet
- DAFTARRUJUKANDocument4 pagesDAFTARRUJUKANIndahNo ratings yet
- Zoology Practical 4Document13 pagesZoology Practical 4Asraful IslamNo ratings yet
- MBBS Cafeteria TEST 1Document7 pagesMBBS Cafeteria TEST 1aalishba6a2b9cNo ratings yet
- Access To JusticeDocument9 pagesAccess To JusticeprimeNo ratings yet
- Blood Stasis and What Does That MeanDocument2 pagesBlood Stasis and What Does That MeanCarl MacCordNo ratings yet
- 1000 Câu Word FormDocument36 pages1000 Câu Word FormThùy Linh LêNo ratings yet
- Up & Up LyricDocument2 pagesUp & Up LyricMuhammad Ali MahdiNo ratings yet
- Jeremiah's Law, Introduced by Assemblywoman Rodneyse BichotteDocument2 pagesJeremiah's Law, Introduced by Assemblywoman Rodneyse BichotteCity & State NYNo ratings yet