You might also like
- Carbon MonoxideDocument15 pagesCarbon Monoxidevart1992No ratings yet
- Forensic Science Project: Carbon MonoxideDocument16 pagesForensic Science Project: Carbon MonoxideManavNo ratings yet
- Detect Carbon Monoxide (CO) With Gas SensorsDocument9 pagesDetect Carbon Monoxide (CO) With Gas SensorsCambraia MRC Detectores de GásNo ratings yet
- Carbon Monoxide in The WorkplaceDocument30 pagesCarbon Monoxide in The WorkplaceuygunberkayNo ratings yet
- lab 6 BDocument4 pageslab 6 Buzair akramNo ratings yet
- Carbon MonoxideDocument9 pagesCarbon Monoxidezackay GGNo ratings yet
- Forensic ScienceDocument13 pagesForensic ScienceSania KhanNo ratings yet
- Air pollutionDocument20 pagesAir pollutioncarlotarubioperez123No ratings yet
- Toxicology Power PointDocument9 pagesToxicology Power Pointdigibuilders18No ratings yet
- CarbonmonoxideDocument5 pagesCarbonmonoxideXaniaEliNo ratings yet
- EnglishDocument3 pagesEnglishAlana MesquitaNo ratings yet
- The Hidden Killer: Understanding Carbon Monoxide PoisoningDocument2 pagesThe Hidden Killer: Understanding Carbon Monoxide PoisoningMohammed Abdul HakeemNo ratings yet
- Facts about the Silent Killer Carbon MonoxideDocument20 pagesFacts about the Silent Killer Carbon MonoxideSuad BushiNo ratings yet
- Interaction Study of Carbon Monoxide Poisoning TherapiesdrugsDocument8 pagesInteraction Study of Carbon Monoxide Poisoning TherapiesdrugssejalNo ratings yet
- Carbon Monoxide Safety: Marshall University Safety & HealthDocument22 pagesCarbon Monoxide Safety: Marshall University Safety & HealthIr ComplicatedNo ratings yet
- Carbon Monoxide PoisoningDocument9 pagesCarbon Monoxide PoisoningIlyes FerenczNo ratings yet
- Carbon Monoxide Poisoning: A Guide For Gps and Other Medical ProfessionalsDocument4 pagesCarbon Monoxide Poisoning: A Guide For Gps and Other Medical ProfessionalsAchmad Ageng SeloNo ratings yet
- Chemistry ProjectDocument12 pagesChemistry Projects.reeva.jainNo ratings yet
- EVS Unit 1 PDFDocument72 pagesEVS Unit 1 PDFNIPER BNGNo ratings yet
- Experiment # 08: ObjectiveDocument3 pagesExperiment # 08: ObjectiveHamza FaheemNo ratings yet
- Investigation of CO2 Capturing Capacity of Solid Adsorbents (PEIs) Polyethylenimines From Automotive Vehicle Exhausts System For 4-Stroke SI EngineDocument5 pagesInvestigation of CO2 Capturing Capacity of Solid Adsorbents (PEIs) Polyethylenimines From Automotive Vehicle Exhausts System For 4-Stroke SI EngineBONFRINGNo ratings yet
- Environmental Biotechnology (BBT427) Spring 2020: Prepared by Dr. Ishrat JabeenDocument23 pagesEnvironmental Biotechnology (BBT427) Spring 2020: Prepared by Dr. Ishrat JabeenEarfanNo ratings yet
- Fy15 SH 27666 Sh5 CarbonMonoxideInhalationHazardsDocument83 pagesFy15 SH 27666 Sh5 CarbonMonoxideInhalationHazardsAwalJefriNo ratings yet
- Emergency Preparedness and Response For Carbon Monoxide: by - S. G. PatelDocument33 pagesEmergency Preparedness and Response For Carbon Monoxide: by - S. G. PatelNeel VaderaNo ratings yet
- Efficiency Without Destruction: Why Ceramics Has Been Used in Building The Engine?Document4 pagesEfficiency Without Destruction: Why Ceramics Has Been Used in Building The Engine?SoumavoGhoshNo ratings yet
- Air Quality and HealthDocument8 pagesAir Quality and HealthAlexNo ratings yet
- Topic-Carbon Monoxide: Mrs. Deepika SandhuDocument17 pagesTopic-Carbon Monoxide: Mrs. Deepika SandhuPrabhat PrajapatiNo ratings yet
- Air Based HazardsDocument19 pagesAir Based HazardsRushaliNo ratings yet
- AIR POLLUTION: PAN, CFCs & MTBEDocument35 pagesAIR POLLUTION: PAN, CFCs & MTBEAleena NaeemNo ratings yet
- Rijal Maulana HaqimDocument8 pagesRijal Maulana HaqimRijal Maulana HaqimNo ratings yet
- Toxic GasesDocument44 pagesToxic Gasesasmaa100% (1)
- How-To Reduce VOC-emissionsDocument13 pagesHow-To Reduce VOC-emissionsMaria De La HozNo ratings yet
- Pollutant: Any Substance That Causes Nuisance or Harmful Effects or Uneasiness To The EcosystemDocument56 pagesPollutant: Any Substance That Causes Nuisance or Harmful Effects or Uneasiness To The EcosystemObotigho Richard IwoNo ratings yet
- Air Pollution Week 1Document35 pagesAir Pollution Week 1kumkum bhagyaNo ratings yet
- MHT CET 2023 Question Paper May 19 Shift 2Document7 pagesMHT CET 2023 Question Paper May 19 Shift 2Pranav PatiLNo ratings yet
- Carbon Monoxide White PaperDocument10 pagesCarbon Monoxide White PaperarjmandquestNo ratings yet
- Lecture - 4 - Environmental Studies (BITS-F 225) Smita Raghuvanshi Associate Professor, Dept of Chemical Engineering August 26, 2020Document30 pagesLecture - 4 - Environmental Studies (BITS-F 225) Smita Raghuvanshi Associate Professor, Dept of Chemical Engineering August 26, 2020WX YZNo ratings yet
- Hand Outs - Educ 210Document7 pagesHand Outs - Educ 210Ruel YolagaNo ratings yet
- Unit 2 and Some Parts of Unit 1Document90 pagesUnit 2 and Some Parts of Unit 1Priyanshu KumarNo ratings yet
- Air Pollution - Toxicology Study GuideDocument8 pagesAir Pollution - Toxicology Study GuideCourtney SullivanNo ratings yet
- Missy1235 OriginalDocument20 pagesMissy1235 OriginalMisba KhanNo ratings yet
- AUC Environmental Science - Air Pollution: Causes, Effects and Control MethodsDocument35 pagesAUC Environmental Science - Air Pollution: Causes, Effects and Control MethodsAviects Avie JaroNo ratings yet
- Design of A Gas Detection System Chapter 1Document7 pagesDesign of A Gas Detection System Chapter 1Shady ZillahNo ratings yet
- Emissions From Vehicles and Their Effects On Natural EnvironmentDocument19 pagesEmissions From Vehicles and Their Effects On Natural EnvironmentKarthik VNo ratings yet
- Air PollutionDocument10 pagesAir Pollutionapi-301790589No ratings yet
- Green Chemistry and Alternative Energy Resources: Module - 4Document12 pagesGreen Chemistry and Alternative Energy Resources: Module - 4Eli ShaneNo ratings yet
- CHAPTER IIdDocument5 pagesCHAPTER IIdPaetan, AngelikaNo ratings yet
- Carbon Monoxide Research PaperDocument4 pagesCarbon Monoxide Research Paperfvfmxb2y100% (1)
- US Labor Guide to Carbon Monoxide ExposureDocument8 pagesUS Labor Guide to Carbon Monoxide ExposureNeel VaderaNo ratings yet
- Blue Smoke EmissionsDocument24 pagesBlue Smoke Emissionswilliam alachanNo ratings yet
- Environmental Pollution and ControlDocument56 pagesEnvironmental Pollution and ControlNazrul IzdhamNo ratings yet
- Air Pollution: Causes, Effects and Control MeasuresDocument38 pagesAir Pollution: Causes, Effects and Control Measuressem31No ratings yet
- Periodica AlscovalentcompoundDocument5 pagesPeriodica Alscovalentcompoundapi-287717009No ratings yet
- 1 - Toxic GasesDocument19 pages1 - Toxic GasesxIRONxWOLFxNo ratings yet
- Air Pollutants and Effects: Technological Institute of The PhilippinesDocument38 pagesAir Pollutants and Effects: Technological Institute of The PhilippinesDarkterror KenNo ratings yet
- Air Pollution: Project ReportDocument36 pagesAir Pollution: Project ReportAlok Nayak83% (6)
- Environmental Pollution, Waste Management and Water Chemistry AnalysisDocument22 pagesEnvironmental Pollution, Waste Management and Water Chemistry AnalysisshreyaNo ratings yet
- Volume 3 No6 2010Document9 pagesVolume 3 No6 2010Hanim HusaifNo ratings yet
- Electrofisiologia Cardiaca Guia Viasual 2 PDFDocument82 pagesElectrofisiologia Cardiaca Guia Viasual 2 PDFMiguel LizarragaNo ratings yet
- Haemostasis: 1. Vascular SpasmDocument5 pagesHaemostasis: 1. Vascular SpasmAnurag YadavNo ratings yet
- Inscopix NVista Product BrochureDocument8 pagesInscopix NVista Product BrochureSEO NeuroscienceNo ratings yet
- APPENDIX C: MONSTROUS GRAFTSDocument5 pagesAPPENDIX C: MONSTROUS GRAFTSLeonardoGuliaNo ratings yet
- Igcse Questions Placenta and Umbilical CordDocument3 pagesIgcse Questions Placenta and Umbilical CordFabriV9No ratings yet
- ELSC2111 Earth and Life Science Q2 Long Quiz 2 (19) 3Document6 pagesELSC2111 Earth and Life Science Q2 Long Quiz 2 (19) 3Christian TeroNo ratings yet
- Neuro-Oncology Explained Through Multiple Choice Questions: Joe M DasDocument243 pagesNeuro-Oncology Explained Through Multiple Choice Questions: Joe M Dasalistair90100% (1)
- EAR MCQdoneDocument71 pagesEAR MCQdoneAbdur Raheem QureshiNo ratings yet
- Lesson 2 - Muscular SystemDocument7 pagesLesson 2 - Muscular SystemCherubim GimaranganNo ratings yet
- Larval Stages of Trematoda and CestodaDocument41 pagesLarval Stages of Trematoda and CestodaSneha ManjulNo ratings yet
- Hickman Zoology 18e PDFDocument4 pagesHickman Zoology 18e PDFSalsabila Tasyari0% (1)
- NEET CUMULATIVE TEST -2 Biology QuestionsDocument24 pagesNEET CUMULATIVE TEST -2 Biology Questionsbal_thakreNo ratings yet
- The Blue Brain Project and Whole Brain SimulationDocument3 pagesThe Blue Brain Project and Whole Brain Simulationchevlin44No ratings yet
- PHM 3471 Merged Week (1-6)Document303 pagesPHM 3471 Merged Week (1-6)Lisa MuthiniNo ratings yet
- Anemia of Abnormal Iron MetabolismDocument17 pagesAnemia of Abnormal Iron MetabolismJoezer Gumangan VeranoNo ratings yet
- C:/Users/Prima Agung Laksono/Pictures/tugas DR NP/Philips-Goldway-G30E-G40E-preconfigured-Patient - Monitors PDFDocument10 pagesC:/Users/Prima Agung Laksono/Pictures/tugas DR NP/Philips-Goldway-G30E-G40E-preconfigured-Patient - Monitors PDFPrima Agung LNo ratings yet
- Invertebrates: Arthropods CharacteristicsDocument4 pagesInvertebrates: Arthropods Characteristicsfaith dicdicanNo ratings yet
- Neetpg LRR Pathology Part 2 PDFDocument92 pagesNeetpg LRR Pathology Part 2 PDFMaheshNo ratings yet
- Science WorksheetDocument3 pagesScience WorksheetvienergresourcesNo ratings yet
- Diagnostics: Rare Causes of Arterial Hypertension and Thoracic Aortic Aneurysms-A Case-Based ReviewDocument16 pagesDiagnostics: Rare Causes of Arterial Hypertension and Thoracic Aortic Aneurysms-A Case-Based ReviewBreeze ChloeNo ratings yet
- Hypersensitivity Reactions: Type III and Type IV HypersensitivityDocument36 pagesHypersensitivity Reactions: Type III and Type IV HypersensitivityDil NavabNo ratings yet
- What Is General Adaptation SyndromeDocument3 pagesWhat Is General Adaptation SyndromeCARLOS, Ryan CholoNo ratings yet
- 3.6.induced Breeding of Indian Major CarpsDocument14 pages3.6.induced Breeding of Indian Major CarpsAlivia Roy100% (1)
- Pregnancy Induced Hypertension Nursing Care PlanDocument5 pagesPregnancy Induced Hypertension Nursing Care Planjohncarlo ramosNo ratings yet
- (1479683X - European Journal of Endocrinology) Testosterone and Cognitive Function - Current Clinical Evidence of A RelationshipDocument9 pages(1479683X - European Journal of Endocrinology) Testosterone and Cognitive Function - Current Clinical Evidence of A RelationshipAlan LuiNo ratings yet
- ISBB Immunology ReviewDocument9 pagesISBB Immunology ReviewNathan DrakeNo ratings yet
- Life Processes Notes (Yashvi Modi)Document15 pagesLife Processes Notes (Yashvi Modi)YASHVI MODI60% (5)
- Laguna Kosmetik Lutronic Aesthetic Encurve™Document4 pagesLaguna Kosmetik Lutronic Aesthetic Encurve™kberenangNo ratings yet
- Pulse Oximetry ExplainedDocument32 pagesPulse Oximetry Explainedابتسـامه العنزي100% (1)
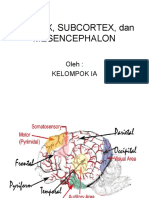
- Korteks DoneDocument16 pagesKorteks DoneNur WahyudiNo ratings yet