You might also like
- RCCM 202212-2300ocDocument14 pagesRCCM 202212-2300ocLucas PereiraNo ratings yet
- Airway Pressure Release VentilatiDocument9 pagesAirway Pressure Release VentilatiDavid ParraNo ratings yet
- SDRA ventilacion alta frecuenciaDocument8 pagesSDRA ventilacion alta frecuenciaDavid Davoas A. SolizNo ratings yet
- Dasenbrook higherPEEP 11 PrintedDocument8 pagesDasenbrook higherPEEP 11 PrintedОлег СатишурNo ratings yet
- Peep, Prona e Proteina C ReativaDocument0 pagesPeep, Prona e Proteina C ReativaEduardo SoaresNo ratings yet
- PEEP Titration During Prone Positioning For Acute Respiratory Distress SyndromeDocument6 pagesPEEP Titration During Prone Positioning For Acute Respiratory Distress Syndromedani yan sNo ratings yet
- Antacid Therapy and Disease Progression in Patients With Idiopathic Pulmonary Fibrosis Who Received PirfenidoneDocument9 pagesAntacid Therapy and Disease Progression in Patients With Idiopathic Pulmonary Fibrosis Who Received PirfenidoneAquiles CastroNo ratings yet
- AsmathDocument6 pagesAsmathRido SaputraNo ratings yet
- Estratégias de Ventilação em PacientesDocument10 pagesEstratégias de Ventilação em PacientesAllisson GomesNo ratings yet
- VPP No InvasivaDocument12 pagesVPP No InvasivaItzel AgustínNo ratings yet
- Zampieri 2019Document8 pagesZampieri 2019Peter AgabaNo ratings yet
- 9mechanical Ventilation in Sepsis-Induced Acute LungDocument6 pages9mechanical Ventilation in Sepsis-Induced Acute LungTeodora ZamfirescuNo ratings yet
- Acc 2021 00927Document9 pagesAcc 2021 00927DON TVNo ratings yet
- RCCM 201902-0334ocDocument10 pagesRCCM 201902-0334ocrodolfo riosNo ratings yet
- 3497 PDFDocument22 pages3497 PDFJei CoronelNo ratings yet
- Low 2018Document9 pagesLow 2018Hendri WahyudiNo ratings yet
- The Acute Respiratory Distress Syndrome in 2013: Review Open AccessDocument6 pagesThe Acute Respiratory Distress Syndrome in 2013: Review Open Accessindriyanti natasya ayu utami kottenNo ratings yet
- Journal Homepage: - : IntroductionDocument3 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Invasive Mechanical Ventilation PDFDocument4 pagesInvasive Mechanical Ventilation PDFRaquel AguilarNo ratings yet
- 1 s2.0 S1098301510688778 MainDocument2 pages1 s2.0 S1098301510688778 MainPeter SalimNo ratings yet
- 40Document9 pages40Eduardo SoaresNo ratings yet
- Steroids For Airway EdemaDocument7 pagesSteroids For Airway EdemaDamal An NasherNo ratings yet
- Article - 1Document8 pagesArticle - 1g5j4s76zc4No ratings yet
- HFNCDocument10 pagesHFNCDollenz Maldonado Natalie CamilaNo ratings yet
- A Meta-Analysis On Intravenous Magnesium Sulphate For Treating Acute AsthmaDocument5 pagesA Meta-Analysis On Intravenous Magnesium Sulphate For Treating Acute AsthmayunitadwiherwatiNo ratings yet
- Decrease in Paco2 With Prone Position Is Predictive of Improved Outcome in Acute Respiratory Distress SyndromeDocument7 pagesDecrease in Paco2 With Prone Position Is Predictive of Improved Outcome in Acute Respiratory Distress SyndromedarwigNo ratings yet
- CF Ventilation ManagementDocument10 pagesCF Ventilation ManagementSherry SaidNo ratings yet
- Outcomes For Surgery CPADocument7 pagesOutcomes For Surgery CPAIndah Nur LathifahNo ratings yet
- Mortality in Pediatric Acute Respiratory Distress Syndrome: A Systematic Review and Meta-AnalysisDocument9 pagesMortality in Pediatric Acute Respiratory Distress Syndrome: A Systematic Review and Meta-Analysisesya putrri oktareginaNo ratings yet
- Comment: See Page E218Document2 pagesComment: See Page E218BBD BBDNo ratings yet
- The Association Between BMI and COPD: The Results of Two Population-Based Studies in Guangzhou, ChinaDocument6 pagesThe Association Between BMI and COPD: The Results of Two Population-Based Studies in Guangzhou, ChinaMutia FatinNo ratings yet
- The Relationshep of Tidal Volume and Driving Presure Whit Mortality in Hypoxic Patients Receiving Mechanical VentilationDocument15 pagesThe Relationshep of Tidal Volume and Driving Presure Whit Mortality in Hypoxic Patients Receiving Mechanical VentilationDante Leonardo Garcia MenaNo ratings yet
- Review ArticleDocument9 pagesReview ArticleAyu SuwarayuNo ratings yet
- 1 s2.0 S2452247318303200 MainDocument5 pages1 s2.0 S2452247318303200 Mainputujunidtd13No ratings yet
- Korti Ko SteroidDocument7 pagesKorti Ko SteroidSisca AndrianyNo ratings yet
- Pertanyaan 7Document14 pagesPertanyaan 7WicakNo ratings yet
- ArchMedHealthSci52167-1734105 044901Document5 pagesArchMedHealthSci52167-1734105 044901Ahmad NaserNo ratings yet
- The Honeycomb Network: The ASCEND Trial in Idiopathic Pulmonary FibrosisDocument4 pagesThe Honeycomb Network: The ASCEND Trial in Idiopathic Pulmonary FibrosisAnna LiachenkoNo ratings yet
- CESAR - Conventional Ventilatory Support Vs Extracorporeal Membrane Oxygenation For Severe Adult Respiratory FailureDocument13 pagesCESAR - Conventional Ventilatory Support Vs Extracorporeal Membrane Oxygenation For Severe Adult Respiratory FailureSebastian CaimanqueNo ratings yet
- How To Use Article Diagnostic Test PDFDocument3 pagesHow To Use Article Diagnostic Test PDFzahrara90No ratings yet
- PESI Critical Care 2005Document6 pagesPESI Critical Care 2005Rocio Méndez FrancoNo ratings yet
- Zhao - 2023 - The Impact of The New Acute Respiratory Distress SDocument10 pagesZhao - 2023 - The Impact of The New Acute Respiratory Distress Sgavain.ferronsNo ratings yet
- RCCM 201607-1383ocDocument10 pagesRCCM 201607-1383ocLeiniker NavarroNo ratings yet
- EXPRESS Trial 2008Document10 pagesEXPRESS Trial 2008Dr. Sergio Oscar AlunniNo ratings yet
- Ardsnetwork (Nhlbi) Studies: Successesand Challengesinards ClinicalresearchDocument10 pagesArdsnetwork (Nhlbi) Studies: Successesand Challengesinards ClinicalresearchEduardo SoaresNo ratings yet
- Efficacy and Safety of Acupoint Autohemotherapy in PDFDocument5 pagesEfficacy and Safety of Acupoint Autohemotherapy in PDFtizziana carollaNo ratings yet
- Jurnal BTKV DodiDocument10 pagesJurnal BTKV DodiAchmad Dodi MeidiantoNo ratings yet
- 2020 Article 2741Document10 pages2020 Article 2741Roberto Guerrero MonsivaisNo ratings yet
- The Effects of Thoracic Epidural Analgesia On Oxygenation and Pulmonary Shunt Fraction During One-Lung Ventilation: An Meta-AnalysisDocument11 pagesThe Effects of Thoracic Epidural Analgesia On Oxygenation and Pulmonary Shunt Fraction During One-Lung Ventilation: An Meta-AnalysisVignesh VenkatesanNo ratings yet
- Riociguat For The Treatment of Chronic Thromboembolic Pulmonary Hypertension: A Long-Term Extension Study (CHEST-2)Document10 pagesRiociguat For The Treatment of Chronic Thromboembolic Pulmonary Hypertension: A Long-Term Extension Study (CHEST-2)FinaNo ratings yet
- How We Approach Titrating PEEP in Patients With Acute HypoxemicDocument5 pagesHow We Approach Titrating PEEP in Patients With Acute Hypoxemicjasanchez8No ratings yet
- Enteral Versus Parenteral Nutrition in Critically Ill Patients - An Updated Systematic Review and Meta-Analysis of Randomized Controlled TrialsDocument14 pagesEnteral Versus Parenteral Nutrition in Critically Ill Patients - An Updated Systematic Review and Meta-Analysis of Randomized Controlled TrialsLea Bali Ulina SinurayaNo ratings yet
- Predictive Value of Red Blood Cell Distribution Width in ChronicDocument8 pagesPredictive Value of Red Blood Cell Distribution Width in ChronicAndreea MoalesNo ratings yet
- Unraveling The Pathophysiology of The Asthma-COPD Overlap SyndromeDocument8 pagesUnraveling The Pathophysiology of The Asthma-COPD Overlap SyndromeRadhianie DjanNo ratings yet
- Evidence-Based Management of Acute Lung Injury and Acute Respiratory Distress SyndromeDocument17 pagesEvidence-Based Management of Acute Lung Injury and Acute Respiratory Distress SyndromeretNo ratings yet
- Pone 0165942Document15 pagesPone 0165942rastiNo ratings yet
- Jurnal CopdDocument11 pagesJurnal Copdgemarawan abadiNo ratings yet
- 8. Negative-_versus_positive-pressure_ventilation_in_Document11 pages8. Negative-_versus_positive-pressure_ventilation_in_Dwi Putri SekariniNo ratings yet
- PMC4118277 1465 9921 15 80Document7 pagesPMC4118277 1465 9921 15 80Isra Al-KautsarNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 17: OncologyFrom EverandComplementary and Alternative Medical Lab Testing Part 17: OncologyNo ratings yet
- Clinical SupervisionDocument19 pagesClinical Supervisionsrinivasana100% (1)
- CORAD 101, Health and Welfare ProgramsDocument5 pagesCORAD 101, Health and Welfare ProgramsdaybudsvaldezNo ratings yet
- Smart Health Care ReportDocument86 pagesSmart Health Care ReportHEESOO LEENo ratings yet
- Occupational Health and Safety Manual PDFDocument2 pagesOccupational Health and Safety Manual PDFVeronica50% (2)
- Genetic Counselling Seminar for NursesDocument22 pagesGenetic Counselling Seminar for NursesGopika SNo ratings yet
- Impact of Social Media On Nurses Service Delivery - EditedDocument14 pagesImpact of Social Media On Nurses Service Delivery - EditedMaina PeterNo ratings yet
- Ethical Concerns in Family Therapy: Paulette M. Hines and Rachel T. Hare-MustinDocument7 pagesEthical Concerns in Family Therapy: Paulette M. Hines and Rachel T. Hare-MustinPaula CelsieNo ratings yet
- Electronic Medical Record ThesisDocument7 pagesElectronic Medical Record Thesislisanetkowiczerie100% (2)
- Social Security and Labor Welfare (MBA-961) : Q.1 What Is The Concept of Social Security?Document16 pagesSocial Security and Labor Welfare (MBA-961) : Q.1 What Is The Concept of Social Security?Nisha RineshNo ratings yet
- Multiple Pregnancy 2008Document61 pagesMultiple Pregnancy 2008Dagnachew kasayeNo ratings yet
- Jurnal Reading: Sit Dolor AmetDocument20 pagesJurnal Reading: Sit Dolor AmetLiri AndiyaniNo ratings yet
- Brain Tumor - Adults: Contents of This PageDocument5 pagesBrain Tumor - Adults: Contents of This PageSam StancerNo ratings yet
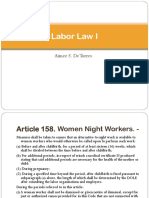
- De Torres Labor Law I ReportDocument11 pagesDe Torres Labor Law I ReportErole John AtienzaNo ratings yet
- Big DataDocument156 pagesBig DatalidieskaNo ratings yet
- 4128i HSRN 192700105 04 000Document18 pages4128i HSRN 192700105 04 000Padma ShivanandaNo ratings yet
- Notre Dame University Home Visit PlanDocument3 pagesNotre Dame University Home Visit PlanMarielle ChuaNo ratings yet
- DRM 503 Final Requirement - Cruzat - Fontilar - Maravilla - Miranda - RelopezDocument12 pagesDRM 503 Final Requirement - Cruzat - Fontilar - Maravilla - Miranda - RelopezEy-ey ChioNo ratings yet
- Tonsillitis Inggris PDFDocument18 pagesTonsillitis Inggris PDFRiris RaudyaNo ratings yet
- How Prolonged Immobilization Negatively Impacts the BodyDocument45 pagesHow Prolonged Immobilization Negatively Impacts the BodyjhnaidillaNo ratings yet
- Job Safety Analysis and Risk AssessmentDocument12 pagesJob Safety Analysis and Risk AssessmentRejib Kibar0% (1)
- Chhattisgarh Company 1Document158 pagesChhattisgarh Company 1Ramagopalan KNo ratings yet
- Sychology of Disability Sport - Participation and PerformanceDocument14 pagesSychology of Disability Sport - Participation and PerformanceCatarina GrandeNo ratings yet
- On Health, Ability and Activity: Comments On Some Basic Notions in The ICFDocument5 pagesOn Health, Ability and Activity: Comments On Some Basic Notions in The ICFGsar Gsar GsarNo ratings yet
- Standard Operating Procedures for Health ProfessionalsDocument89 pagesStandard Operating Procedures for Health ProfessionalsMathivanan Anbazhagan50% (4)
- NCLEX Practice Questions Quiz #4: Fundamentals of NursingDocument12 pagesNCLEX Practice Questions Quiz #4: Fundamentals of NursingRegine Mae Encinada100% (1)
- Date: 9/10/15 Week of 9/07/15Document4 pagesDate: 9/10/15 Week of 9/07/15api-296922357No ratings yet
- Food Safety OfficerDocument5 pagesFood Safety OfficersivaguruaksNo ratings yet
- Intensivist To Patient RatioDocument8 pagesIntensivist To Patient RatioroykelumendekNo ratings yet
- Mini Hifu 4Document9 pagesMini Hifu 4clatrecchienaNo ratings yet
- CHN Notes For MidtermsDocument24 pagesCHN Notes For MidtermsReiner Lopez100% (1)