You might also like
- Running Head: MIAH ZAVARRO V3 Miah Zavarro V3 Name Course Institution DateDocument4 pagesRunning Head: MIAH ZAVARRO V3 Miah Zavarro V3 Name Course Institution DateSammy Chege100% (1)
- COSHH Assessment TemplateDocument2 pagesCOSHH Assessment TemplaterichardNo ratings yet
- PETRONAS Fuel Oil 80: Safety Data SheetDocument10 pagesPETRONAS Fuel Oil 80: Safety Data SheetJaharudin JuhanNo ratings yet
- Effects of Manual Therapy On Treatment Duration and Motor Development in Infants With Severe Nonsynostotic Plagioceophaly - A Randomised Controlled Pilot StudyDocument7 pagesEffects of Manual Therapy On Treatment Duration and Motor Development in Infants With Severe Nonsynostotic Plagioceophaly - A Randomised Controlled Pilot StudyMarcus Dos Santos100% (2)
- EDUC-5420 - Week 1# Written AssignmentDocument7 pagesEDUC-5420 - Week 1# Written AssignmentShivaniNo ratings yet
- (2010 Weng) Influence of Microgap Location and Configuration On Peri-Implant Bone Morphology in Nonsubmerged Implants - An Experimental Study in DogsDocument8 pages(2010 Weng) Influence of Microgap Location and Configuration On Peri-Implant Bone Morphology in Nonsubmerged Implants - An Experimental Study in Dogsyena1010No ratings yet
- 10 11607@jomi 8122Document8 pages10 11607@jomi 8122Marlene Kasumi Gantier TakanoNo ratings yet
- Ridge Preservation Techniques For Implant Therapy: JO M I 2009 24 :260-271Document12 pagesRidge Preservation Techniques For Implant Therapy: JO M I 2009 24 :260-271Viorel FaneaNo ratings yet
- 2019 Dale RobinsonDocument11 pages2019 Dale Robinson謎超人No ratings yet
- CrestalDocument6 pagesCrestalRik ChatterjeeNo ratings yet
- 2005 Rojas VizcayaDocument14 pages2005 Rojas Vizcayacasto.carpetasmiaNo ratings yet
- Efficacy of Nano-Hydroxyapatite Coating On Osseointegration of Early Loaded Dental ImplantsDocument12 pagesEfficacy of Nano-Hydroxyapatite Coating On Osseointegration of Early Loaded Dental ImplantsIJAR JOURNALNo ratings yet
- Id 0000000000000592Document8 pagesId 0000000000000592phungNo ratings yet
- The Role of Occlusion in Implant Therapy - A Comprehensive Updated ReviewDocument10 pagesThe Role of Occlusion in Implant Therapy - A Comprehensive Updated ReviewFrancisca Dinamarca LamaNo ratings yet
- 10.1016@j.medengphy.2015.02.004 Ja Tem ConferirDocument15 pages10.1016@j.medengphy.2015.02.004 Ja Tem ConferirMr OdontologiaNo ratings yet
- (2007 Verri) Verri - Et - Al - 2007 - Lenght - and - Diameter - ImpDocument11 pages(2007 Verri) Verri - Et - Al - 2007 - Lenght - and - Diameter - Impyena1010No ratings yet
- Scs 0b013e31826b8267Document5 pagesScs 0b013e31826b8267ANGELA ROMERONo ratings yet
- Primary Loading of Palatal Implants For Orthodontic Anchorage e A Pilot Animal StudyDocument7 pagesPrimary Loading of Palatal Implants For Orthodontic Anchorage e A Pilot Animal StudyPaola LoloNo ratings yet
- Takahashi2017 PDFDocument7 pagesTakahashi2017 PDFliliana villamilNo ratings yet
- A Comparative Study On Complete and ImDocument8 pagesA Comparative Study On Complete and ImAbraham Gomez BautistaNo ratings yet
- Tooth-Supported Telescopic Prostheses in Compromised Dentitions - A Clinical ReportDocument4 pagesTooth-Supported Telescopic Prostheses in Compromised Dentitions - A Clinical Reportpothikit100% (1)
- Principles of Occlusion in Implant Dentistry PDFDocument7 pagesPrinciples of Occlusion in Implant Dentistry PDFnakul wareNo ratings yet
- Mandibular Arch DistalizationDocument33 pagesMandibular Arch DistalizationRohini TondaNo ratings yet
- Splinted Fixed Partial DentureDocument7 pagesSplinted Fixed Partial DenturebradbiancaionelaNo ratings yet
- Ammar 2011Document13 pagesAmmar 2011manju deviNo ratings yet
- Çakir OzkanDocument5 pagesÇakir OzkanAntonio LoureiroNo ratings yet
- Biomechanical Comparison of Axial and Tilted Implants For Mandibular Full-Arch Fixed ProsthesesDocument9 pagesBiomechanical Comparison of Axial and Tilted Implants For Mandibular Full-Arch Fixed ProsthesesTeresa BeltranNo ratings yet
- HKGFDDocument4 pagesHKGFDNovita RNo ratings yet
- Occlusion in Implant Prosthodontics: Radhika B Parekh, Omkar Shetty, Rubina TabassumDocument4 pagesOcclusion in Implant Prosthodontics: Radhika B Parekh, Omkar Shetty, Rubina TabassumTung Thanh NguyenNo ratings yet
- Correlation Between Miniscrew Stability and Bone Mineral Density in Orthodontic PatientsDocument8 pagesCorrelation Between Miniscrew Stability and Bone Mineral Density in Orthodontic PatientsLaura Juarez navejasNo ratings yet
- Zona Neutra Maxilofacial PacienteDocument6 pagesZona Neutra Maxilofacial Pacientemargarita de montenegroNo ratings yet
- Implant Design PDFDocument9 pagesImplant Design PDFnatan XxNo ratings yet
- The Platform Switching Concept-A Myth or Fact: A Literature ReviewDocument5 pagesThe Platform Switching Concept-A Myth or Fact: A Literature ReviewChifa MusrataNo ratings yet
- Inward-Inclined Implant Platform For The Amplified Platform-Switching Concept: 18-Month Follow-Up Report of A Prospective Randomized Matched-Pair Controlled TrialDocument9 pagesInward-Inclined Implant Platform For The Amplified Platform-Switching Concept: 18-Month Follow-Up Report of A Prospective Randomized Matched-Pair Controlled TrialdivyaNo ratings yet
- Occlusion For Implant Suppported CD PDFDocument4 pagesOcclusion For Implant Suppported CD PDFFabián SajamaNo ratings yet
- The Fate of The Distal Papilla Around Tooth-Bound Implant-Supported Restorations in Maxillary Central Incisor SitesDocument7 pagesThe Fate of The Distal Papilla Around Tooth-Bound Implant-Supported Restorations in Maxillary Central Incisor SitesValentinaNo ratings yet
- Use of Implants in The Pterygoid RegionDocument4 pagesUse of Implants in The Pterygoid RegionManjulika TysgiNo ratings yet
- Use of Implants in The Pterygoid Region For Prosthodontic TreatmentDocument4 pagesUse of Implants in The Pterygoid Region For Prosthodontic TreatmentSidhartha KumarNo ratings yet
- Immediate Versus Conventional Loading of Implant-Supported Maxillary Overdentures: A Finite Element Stress AnalysisDocument7 pagesImmediate Versus Conventional Loading of Implant-Supported Maxillary Overdentures: A Finite Element Stress AnalysisMr OdontologiaNo ratings yet
- 06.Long-Term Follow-Up On Soft and Hard TissueDocument8 pages06.Long-Term Follow-Up On Soft and Hard Tissue친절No ratings yet
- 1 s2.0 S1991790219308700 MainDocument6 pages1 s2.0 S1991790219308700 MainRonin ZxxNo ratings yet
- Wee Neutral ZoneDocument7 pagesWee Neutral ZoneGeby JeonNo ratings yet
- Expansion Maxilar Con Miniimplantes Monocorticales y BicorticalesDocument15 pagesExpansion Maxilar Con Miniimplantes Monocorticales y BicorticalesLiliana Rojas CarlottoNo ratings yet
- Avoiding Errors and Complications Related To Immediate Implant Placement in The Esthetic Area With A Mucogingival ApproachDocument11 pagesAvoiding Errors and Complications Related To Immediate Implant Placement in The Esthetic Area With A Mucogingival ApproachL1FonsecaNo ratings yet
- Occlusion For Implant Suppported CDDocument4 pagesOcclusion For Implant Suppported CDpopat78No ratings yet
- Wilmes 2019Document8 pagesWilmes 2019Vinicius RechNo ratings yet
- Mesialslider AJO-DODocument9 pagesMesialslider AJO-DOAlexander SurikovNo ratings yet
- Palaska 2014Document10 pagesPalaska 2014Marco TeixeiraNo ratings yet
- Fixed Prosthetic Implant Restoration of The Edentulous Maxilla A Systematic Pretreatment Evaluation Method - Jan - 2008Document11 pagesFixed Prosthetic Implant Restoration of The Edentulous Maxilla A Systematic Pretreatment Evaluation Method - Jan - 2008Nathawat PleumsamranNo ratings yet
- Koutouzisetal 2013IJOMIAbutmentdisconnectionClinicalDocument8 pagesKoutouzisetal 2013IJOMIAbutmentdisconnectionClinicalKyoko CPNo ratings yet
- Lee2016 Usar EsseDocument9 pagesLee2016 Usar EsseMr OdontologiaNo ratings yet
- ImplantesDocument10 pagesImplantesDiana MadridNo ratings yet
- Socket Shield Otto Zuhr Hurzeler PDFDocument12 pagesSocket Shield Otto Zuhr Hurzeler PDFLozovan GregoryNo ratings yet
- Implant-Retained Auricular Prosthesis: A Case Report: January 2010 - Vol.4Document4 pagesImplant-Retained Auricular Prosthesis: A Case Report: January 2010 - Vol.4noranNo ratings yet
- 1 s2.0 S0278239107016424 MainDocument11 pages1 s2.0 S0278239107016424 MainDANTE DELEGUERYNo ratings yet
- Pi Is 0889540615013311Document5 pagesPi Is 0889540615013311msoaresmirandaNo ratings yet
- Single Center Retrospective Analisys of 1001 Consecutevely Placed NobelActive Implants BABBUSH Et AlDocument8 pagesSingle Center Retrospective Analisys of 1001 Consecutevely Placed NobelActive Implants BABBUSH Et AlDr. Rafael OrroNo ratings yet
- JIAP January 2010 - Summers' Technique Modification For Sinus Floor Elevation Using A Connective Tissue Graft. A Case Report.Document4 pagesJIAP January 2010 - Summers' Technique Modification For Sinus Floor Elevation Using A Connective Tissue Graft. A Case Report.Dr. Silviu Andrei ConstantinescuNo ratings yet
- Clin Implant Dent Rel Res - 2021 - Alexopoulou - Immediate Implant in The Posterior Region Combined With Alveolar RidgeDocument12 pagesClin Implant Dent Rel Res - 2021 - Alexopoulou - Immediate Implant in The Posterior Region Combined With Alveolar Ridgecr.bustamantes3481No ratings yet
- 2021 Salim OngunDocument9 pages2021 Salim Ongun謎超人No ratings yet
- Oh 2010Document5 pagesOh 2010gbaez.88No ratings yet
- Effect of Mandibular First Molar Mesialization On Alveolar Bone Height: A Split Mouth StudyDocument7 pagesEffect of Mandibular First Molar Mesialization On Alveolar Bone Height: A Split Mouth StudyRockey ShrivastavaNo ratings yet
- Short ImplantsFrom EverandShort ImplantsBoyd J. TomasettiNo ratings yet
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentFrom EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
- 2579 7925 3 PBDocument7 pages2579 7925 3 PBIntan JesitaNo ratings yet
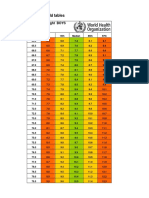
- Boys Simplified Field Tables Weight For Length 2 To 5 Years (Percentiles)Document4 pagesBoys Simplified Field Tables Weight For Length 2 To 5 Years (Percentiles)Gabrielly LopesNo ratings yet
- Blood TransfusionDocument29 pagesBlood TransfusionNonu Kims100% (1)
- Multi-Mechanism Skin Brightening Sabi WhiteDocument6 pagesMulti-Mechanism Skin Brightening Sabi WhiteMuhammad Akhyar RosyidiNo ratings yet
- Surgical Position Supino DecubbitusDocument4 pagesSurgical Position Supino DecubbitusMariana AmayaNo ratings yet
- Gov. Youngkin's Final Budget Presentation Dec 15Document21 pagesGov. Youngkin's Final Budget Presentation Dec 15ABC7NewsNo ratings yet
- Tatalaksana Oftalmia Neonatorum Ec Infeksi Gonokokal Dengan Ikterik Neonatorum - Viora Rianda PiscalokaDocument12 pagesTatalaksana Oftalmia Neonatorum Ec Infeksi Gonokokal Dengan Ikterik Neonatorum - Viora Rianda Piscalokasupaidi97No ratings yet
- Module B - Lesson 3Document14 pagesModule B - Lesson 3Melanie CortezNo ratings yet
- NJSHA NJABA Collaborative Practice GroupDocument4 pagesNJSHA NJABA Collaborative Practice GroupBruno PontesNo ratings yet
- Covid 19 Daily Reporting DasDocument6 pagesCovid 19 Daily Reporting DasRuhayati88gmail.com EyeshieldNo ratings yet
- June 21 NB Underwriting Tips S 58Document24 pagesJune 21 NB Underwriting Tips S 58BGMI NEW 3No ratings yet
- Resin BondedDocument7 pagesResin BondedSalma RafiqNo ratings yet
- D2 0905 Paediatric Reference Intervals - An Update - Tina YenDocument25 pagesD2 0905 Paediatric Reference Intervals - An Update - Tina YenkamalNo ratings yet
- QuestionDocument5 pagesQuestionJavy mae masbateNo ratings yet
- Swim Training Plan 5k ImproverDocument8 pagesSwim Training Plan 5k Improver8b6hjzhqwtNo ratings yet
- Group Assignment RAP SWOT&TOWS HongeditDocument10 pagesGroup Assignment RAP SWOT&TOWS HongeditBùi Thị Thu HồngNo ratings yet
- Revised PPAR-Q Aug. 2022Document2 pagesRevised PPAR-Q Aug. 2022RAY LORENZO LAGASCANo ratings yet
- AVTC 5 - 09 - Group 3 - Business PlanDocument9 pagesAVTC 5 - 09 - Group 3 - Business Planda zelNo ratings yet
- 5 - Sample Invitation Letter-J-1Scholar141218Document2 pages5 - Sample Invitation Letter-J-1Scholar141218saimaNo ratings yet
- Nursing Interview Guide To Collect Subjective Data From The ClientDocument10 pagesNursing Interview Guide To Collect Subjective Data From The ClientDawn EncarnacionNo ratings yet
- School of Medical Sciences Kathmandu UniversityDocument6 pagesSchool of Medical Sciences Kathmandu Universitysuyog raj gautamNo ratings yet
- Research Paper FinalDocument12 pagesResearch Paper Finalapi-609577576No ratings yet
- Summer and Winter VacationsDocument5 pagesSummer and Winter VacationsYahia IdressNo ratings yet
- REMON Article v1Document10 pagesREMON Article v1Aldren R. RemonNo ratings yet
- LIFESCI 2N03: Human: Nutrition For Life ScienceDocument40 pagesLIFESCI 2N03: Human: Nutrition For Life ScienceAnnalisa NguyenNo ratings yet