Professional Documents
Culture Documents
leg-oedema
Uploaded by
Rafan AddisCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
leg-oedema
Uploaded by
Rafan AddisCopyright:
Available Formats
AD_ 0 2 7 _ _ _ AUG0 1 _ 0 8 .
P DF Pa ge 1 7 / 2 4 / 0 8 , 2 : 3 0 PM
How to treat
Pull-out section w w w. a u s t r a l i a n d o c t o r. c o m . a u
Complete How to Treat quizzes online (www.australiandoctor.com.au/cpd) to earn CPD or PDP points.
inside
Deep venous
thrombosis
Venous
insufficiency
Varicose veins
Lymphoedema
The authors
DR PETER R VALE,
interventional cardiovascular
physician, department of vascular
medicine, St Vincent’s Clinic,
Darlinghurst, and department of
cardiology, Mater Misericordiae
Hospital, Crows Nest, NSW.
Local causes of
LEG OEDEMA
Background
DR RICHARD WARD-HARVEY,
vascular surgery registrar,
Royal Prince Alfred Hospital,
Camperdown, NSW.
LEG oedema, or swelling of the legs, is
Table 1: Causes of leg oedema
common and often presents a difficult diag-
nostic dilemma because of the diverse Systemic ■ Anaemia
nature of its possible causes. Patients seek ■ Cardiac dysfunction: ■ Others:
medical advice for a variety of reasons, — left ventricular systolic impairment: ischaemic heart — hereditary angioneurotic oedema DR STEVEN R DUBENEC,
including pain and inability to walk. disease, valvular disease — pregnancy vascular surgeon, Sydney
The distribution of oedema is an impor- — left ventricular diastolic dysfunction: hypertension — idiopathic Endovascular Specialists, Crows
tant guide to the underlying cause. The — right ventricular dysfunction (pericardial effusion, Local Nest, Camperdown Vascular
most important initial question is whether chronic cardiac failure, end-stage chronic airflow ■ Venous:
Associates and Royal Prince Alfred
the oedema is localised or generalised. Leg limitation) — acute DVT Hospital, Camperdown, and Mater
oedema may be either unilateral or bilat- ■ Fluid overload — post-thrombotic sequelae (eg, venous Misericordiae Hospital, Crows Nest,
eral. Bilateral swelling is more commonly ■ Renal disease: incompetence, venous hypertension) NSW.
due to systemic conditions whereas unilat- — acute renal failure (eg, acute glomerulopnephritis) — varicose veins
eral swelling more often represents local — chronic renal failure — obstruction to venous return (eg, pregnancy, pelvic
pathology. ■ Hypoproteinaemic states: tumours, inferior vena cava obstruction)
Table 1 lists the most common causes — chronic liver disease ■ Lymphatic:
of leg oedema that present to GPs today. — nephrotic syndrome — primary lymphoedema
Local causes are usually related to venous — malnutrition — secondary lymphoedema
or lymphatic disease. Systemic causes — protein-losing enteropathy ■ Stasis:
include heart, liver and kidney dysfunc- — malabsorption — paralysis
tion. ■ Endocrine: — poor mobility
Management is based on the underlying — hypothyroidism — obesity
cause, so an accurate and timely diagnosis — Cushing’s syndrome ■ Inflammation:
is paramount. Investigations should be ■ Drugs: — cellulitis
directed to the postulated aetiology but — calcium-channel antagonists — allergic reactions
should also be geared to excluding other — corticosteroids ■ Trauma
possibilities. This article discusses the man- — NSAIDs ■ Congenital:
agement of common local causes of leg — oestrogens — arteriovenous malformations
oedema.
www.australiandoctor.com.au 1 August 2008 | Australian Doctor | 27
AD_ 0 2 9 _ _ _ AUG0 1 _ 0 8 . P DF Pa ge 1 7 / 2 4 / 0 8 , 2 : 3 4 PM
Deep venous thrombosis
DEEP venous thrombosis Studies have found that the rior vena cava thrombosis. range (2.0-3.0) for two con-
(DVT) is a prominent cause of Up to half of all patients with risk factors for PTS appear to D-dimer assays can be secutive days.
acute DVT may lack any
lower limb swelling. It tends
specific sign or symptom.
be ipsilateral recurrence of useful in diagnosis in certain Calf vein thrombosis
to be unilateral and the extent, DVT, poor quality of initial situations. D-dimers are prod- Isolated calf vein thrombi are
site and number of previous anticoagulation for the treat- ucts of the degradation of usually considered relatively
episodes will determine the ment of DVT, and increased cross-linked fibrin by plasmin. low risk for causing PE. How-
degree of swelling. DVT can BMI. Factors that reduce the When measured by ELISA, ever, this risk is not nil, and
cause two clinical scenarios: risk of development of PTS are sensitivity for the diagnosis of proximal propagation (occur-
acute DVT and post-throm- early thrombolysis, early effec- DVT is as high as 96.8%. ring in up to 30% of patients)
botic syndrome (PTS). tive anticoagulation and the Unfortunately, these measure- significantly increases the risk
long-term wearing of gradu- ments are also quite non-spe- for PE and PTS.
Risk factors ated calf-compression stock- cific (as low as 35.2%) with a Debate still exists on
There are many independent ings. high false-positive rate associ- whether to anticoagulate these
risk factors for DVT and pul- ated with: patients; however, patients
monary embolism (PE); how- Investigations ■ Disseminated intravascular with a calf DVT have been
ever, it is not until there is a involved and include: thrombosis will extend into Unfortunately, the diagnosis coagulation. shown to benefit from 6-12
combination of these that a ■ Pain. proximal veins in 25-33% of of DVT based on clinical signs ■ Malignancy. weeks of anticoagulation. If
3,4
DVT will occur. Risk factors ■ Oedema. cases. and symptoms alone is inac- ■ Postoperative states. anticoagulation is not given,
include: ■ Erythema. The important complica- curate; in up to half of ■ Pre-eclampsia. an antiplatelet agent such as
■ Increasing age. ■ Tenderness. tions of DVT are PE and PTS. patients with classic clinical ■ Infection. low-dose aspirin (100mg
■ Male gender. ■ Fever. Inadequate treatment of prox- findings, a DVT is not con- ■ Recent trauma. daily) should be started and
■ Surgery or trauma. ■ Prominent superficial veins. imal lower-extremity venous firmed by diagnostic testing. The high sensitivity of D- graduated compression stock-
■ Hospital or nursing home ■ Calf pain on passive dorsi- thrombosis is associated with a Furthermore, up to half of all dimer measurements makes ings used. A repeat venous
confinement. flexion of the foot (Homans’ 20-50% risk of clinically sig- patients with acute DVT may it theoretically possible to duplex scan should be ordered
■ Malignancy. sign). nificant PE; however, most PE lack any specific sign or symp- exclude a diagnosis of DVT within 5-7 days to determine
■ Neurological disease with ■ Peripheral cyanosis. is clinically silent. High-proba- tom. on the basis of a negative progression.
extremity paresis. However, these may not bility lung scan results may be Contrast venography has result, as long as the patient
■ Central venous catheter or always be present or obvious obtained in 25-51% of historically been the gold stan- is in a low-risk group (ie, Femoropopliteal venous
transvenous pacemaker. and a high index of clinical patients with documented dard for diagnosing acute outpatients with no previ- thrombosis
■ Prior superficial vein throm- suspicion should always be (treated) DVT in the absence DVT. However, venography ous DVT, no PE symptoms). Anticoagulation is standard
bosis. maintained. of pulmonary symptoms. is inconvenient, expensive and Patients with recurrent therapy but does not dissolve
■ Varicose veins. Complete thrombus resolu- may cause significant discom- DVT or DVTs involving the thrombi. Under circum-
Pregnancy, oral contracep- tion has been reported in 56% The post-thrombotic fort. more than the tibial vessels stances of effective anticoagu-
tives and HRT can all increase of patients monitored for nine syndrome Duplex ultrasonography is should be evaluated for a lation, natural fibrinolysis may
the risk for women. The rela- months.1 However, recanali- PTS is the residual effect in the now the most widely used thrombophilia. at least partially recanalise
tive risk increases progressively sation may continue, albeit at limb from the venous hyper- non-invasive tool for diagnos- occluded veins. Even without
from 2.4 in those with one risk a slower rate, for months to tension caused by residual ing DVT. Evaluating the lower Anticoagulant therapy for recanalisation, morbidity may
factor to more than 20 among years after the acute event. obstruction and resultant extremities includes assessing venous thromboembolism be minimal if thrombosis is
those with three or more risk Among patients with proxi- incompetence from the venous compressibility, intra- The objectives of treatment limited to the femoral vein in
factors. mal DVT, recurrent throm- destruction of venous valves. luminal echoes, venous flow in patients with venous the thigh. This treatment can
Independent predictors for boembolic events have been It typically occurs at least 10 characteristics and luminal thromboembolism (VTE) be for 3-6 months, depending
recurrent DVT, which occurs reported in 5.2% of patients years after the initial episode colour filling. Despite its use- are to prevent death from on the patient’s risk.
within 10 years in up to 30% treated for three months with of DVT. fulness, there are limitations, PE, prevent recurrent VTE
of cases, include increasing standard anticoagulation mea- The symptoms of pain, especially in adequately visu- and prevent PTS. Iliofemoral thrombosis
age, obesity, malignancy and sures, compared with 47% of oedema, hyperpigmentation alising the iliac veins, and there The accepted anticoagu- (proximal thrombosis)
extremity paresis. patients who were inade- and/or ulceration are typical may be considerable operator lant therapy for VTE is Patients with proximal throm-
quately treated with low-dose of PTS, which occurs in 29- variability. either continuous IV heparin bosis are usually symptomatic.
2
Acute DVT subcutaneous heparin. 79% of patients with a history CT venography may be or subcutaneous (SC) Characteristically these
Venous obstruction is the Proximal propagation may of DVT. There is no clear rela- used as a second-line investi- enoxaparin (Clexane) then patients have thigh and calf
cause of symptoms and signs also complicate isolated calf tionship between the extent of gation or when an experi- changing to oral warfarin. oedema and pain on both rest
in the acute setting. Signs vein thrombosis in up to 23- thrombus or symptoms on ini- enced vascular laboratory is Heparin or enoxaparin is and ambulation. PE from
and symptoms vary with the 30% of untreated patients. tial presentation and ultimate unavailable. It is also helpful continued until the INR has these large veins may be fatal.
extent of the venous tree Left untreated, calf vein clinical outcome. to identify iliac vein and infe- been within the therapeutic cont’d next page
One Australian life is lost
to heart disease every 20 minutes1,2
1 in 7 patients with a history of CAD* will suffer a major event
(heart attack, stroke or CV death) or hospitalisation within 1 year. 3
*CAD refers to coronary artery disease.
For PBS Information refer to primary advertisement.
BEFORE PRESCRIBING PLEASE REVIEW PRODUCT INFORMATION IN THE PRIMARY ADVERTISEMENT IN THIS PUBLICATION. Plavix (clopidogrel 75 mg). References: 1. www.heartfoundation.com.au (accessed
Nov 2007), media release date 14/9/07. 2. The Shifting Burden of Cardiovascular Disease in Australia. Access Economics; 2005. Downloaded from www.heartfoundation.org.au; 1 April 2008. 3. Steg PG, et al. JAMA 2007;
297(11):1197-1206. sanofi-aventis australia pty ltd ABN 31 008 558 807, Talavera Corporate Centre, Building D, 12-24 Talavera Road, Macquarie Park, NSW 2113. Plavix is a registered trademark of sanofi-aventis. HSX0364/AD/1
www.australiandoctor.com.au 1 August 2008 | Australian Doctor | 29
AD_ 0 3 0 _ _ _ AUG0 1 _ 0 8 . P DF Pa ge 1 7 / 2 4 / 0 8 , 2 : 3 4 PM
How to treat – leg oedema
from previous page tors such as cancer, cava. The devices can be per- Table 2: Indications for insertion of a vena caval filter ■ Ensure adequate hydration.
These patients need immedi- antithrombin deficiency or manent or temporary, depend- ■ Mobilise before, during and
ate anticoagulation with IV the antiphospholipid syn- ing on the indication. Absolute indications after the flight.
heparin, followed by warfarin drome should be treated The main indications for ■ Deep venous thrombosis or documented thromboembolism ■ Avoid combining sedatives
for at least 12 months. indefinitely with warfarin vena caval filters are con- in a patient with a contraindication to anticoagulation with excess alcohol.
The young physically active (unless contraindicated). traindications to anticoagu- ■ Complications of anticoagulation that have forced therapy to ■ Wear non-restrictive cloth-
patient with proximal venous Patients with activated lants (including complications be discontinued ing.
thrombosis should be consid- protein C resistance (factor of anticoagulation that have ■ Recurrent pulmonary embolism despite adequate
ered for catheter-based throm- V Leiden mutation) should mandated therapy be discon- anticoagulation Treatment of oedema
bolytic therapy followed by probably receive indefinite tinued), recurrent PE despite ■ Prophylactic placement in high-risk patients caused by DVT
anticoagulation to lessen the treatment if they have recur- adequate anticoagulation, and Relative indications Lower-limb oedema can be
long-term morbidity of DVT. rent disease, are homozy- for prophylactic placement in ■ Demonstrated free-floating iliofemoral thrombus treated in the acute DVT set-
It has been demonstrated that gous for the gene or have high-risk patients (table 2). ■ A propagating iliofemoral thrombus despite adequate ting with graduated compres-
early clot clearance by either multiple thrombophilic con- anticoagulation sion stockings and appropri-
thrombectomy or catheter- ditions. Prophylaxis in air travel ■ Septic pulmonary embolism ate treatment of the DVT with
directed thrombolysis has The risk of DVT in air travel is ■ Chronic pulmonary embolism in a patient with pulmonary anticoagulants. The acute
better long-term outcomes Inferior vena caval filters in fact very low — one in one hypertension and cor pulmonale swelling tends to settle over 1-
than anticoagulation alone. Vena caval filters are metal million in short flights, increas- ■ A patient with >50% occlusion of the pulmonary vascular bed 2 months, and use of gradu-
devices that are placed in the ing to one in 70,000 for jour- and who would not tolerate any additional thrombus ated compression stockings
Long-term treatment of inferior vena cava under flu- neys longer than 12 hours. ■ Severe ataxia and risk of falling should be continued until the
VTE oroscopic guidance. These There is a higher risk of thrombus load has been docu-
In addition to local manage- devices are designed to DVT in patients with previous icant medical illness. These and SC enoxaparin or heparin. mented as almost resolved.
ment, patients with recurrent ‘catch’ life-threatening DVT or PE, pro-thrombotic patients should use both grad- For all other patients, advice This reduces the risk of devel-
VTE or continuing risk fac- emboli in the inferior vena states, recent surgery or signif- uated compression stockings should be to: oping PTS later in life.
Venous insufficiency
Pathophysiology ■ Chronic venous obstruction due to Table 3: Differential diagnosis supine, is almost completely accepted of a lesser degree of compression.
BETWEEN 10% and 35% of adults previous DVT. of chronic venous ulcers* as effective treatment for venous Another frequent problem is the
have some form of chronic venous ulceration. However, it is impracti- difficulty many weak, elderly, or
disorder, ranging from spider veins Investigation of CVI ■ Arterial disease cal for most patients as anything but arthritic patients experience applying
and simple varicosities to venous The clinical history should include ■ Mixed arterial and venous a short-term solution to a refractory the stockings. Commercially available
ulcers, the last of which affect 4% of questions about: disease or enlarging ulcer. devices can assist these patients, such
people aged over 65. ■ Pain or discomfort. as silk or plastic inner sleeves, or wire-
■ Arteriovenous shunting
Venous reflux is seen when valvu- ■ Visible veins. Compression therapy frame devices.
lar destruction or dysfunction occurs. ■ Itch.
■ Peripheral neuropathies Compression therapy remains the pri- Arterial disease should also be con-
Valvular reflux causes a rise in ambu- ■ Skin pigmentation. ■ Malignancies mary treatment for CVI. It promotes sidered before proceeding with com-
latory venous pressure and a cascade ■ Ulceration. ■ Blood dyscrasias fluid resorption and resolution of pression therapy, as this may aggra-
of pathological events that manifest ■ Bleeding from superficial veins. oedema, with improved diffusion of vate the ulcer or cause further
■ Vasculitides
clinically as: ■ Whether the swelling is unilateral nutrients to the skin and subcuta- lower-limb ischaemia. This may be
■ Varicose veins. or bilateral, and if it worsens during ■ Metabolic diseases: gout, neous tissues. done by performing an ankle brachial
■ Lower extremity oedema. the day. myxoedema Provided there is no cellulitis, index or, if concerned, arranging fur-
■ Pain. ■ Family history. ■ Chronic infectious patients are usually fitted with below- ther assessment by a vascular special-
■ Itching. ■ Previous DVTs. diseases: osteomyelitis, TB, knee, grade-2 graduated compression ist.
■ Skin discolouration. The examination begins with leprosy, syphilis stockings. Patients should obtain two
■ Venous ulceration (in the most observation of each limb in both the pairs to allow laundering, and wear Pharmacological therapy
■ Tropical ulcer
severe form). supine and standing positions. The the stockings at all times while ambu- Despite the oedema, diuretics have
*Source: Padberg 20055
Symptoms and signs specific to distributions of visible large and small latory and remove them at bedtime. no role in the treatment of CVI.
abnormal venous function arise from venous tributaries are noted. When Wound care of ulcers can still Zinc has been found to be of bene-
chronic ambulatory venous hyper- standing, the long and short saphe- biopsy with local anaesthesia. occur under the compression bandage fit in the healing of venous ulcers, but
tension, and are known as chronic nous veins are palpated, and tested Investigation of CVI should include or stocking. After the ulcer has only if pre-treatment zinc levels are
venous insufficiency (CVI). CVI is for a cough impulse, suggesting stress a venous duplex scan of the deep, healed, the patient is instructed to low, and not in all studies.
now thought of as a disease of incompetence. Pigmentation (espe- superficial and perforating veins. The continue ambulatory compression Oxpentifylline (Trental 400)
chronic inflammation due to a sus- cially lipodermatosclerosis), oedema, examination identifies patency, com- therapy indefinitely. Failure to comply reduces blood viscosity, white blood
tained injury secondary to venous induration, cellulitis, lymphangitis or petency and whether there is normal with perpetual compression therapy cell adhesiveness and neutrophil acti-
hypertension. ulceration should be noted. venous anatomy. This information increases the ulcer recurrence rate vation and degranulation. In a meta-
The primary injury is extravasa- Failure to consider other medical linked with the clinical symptoms from about 20% to 60-100%. analysis, oxpentifylline in combina-
tion of macromolecules and ery- illnesses and differential diagnoses helps direct therapeutic options. The most difficult problem is poor tion with compression therapy was
throcytes into the dermal intersti- (table 3) may result in serious misdi- Invasive investigations such as patient compliance, due to discom- more effective than placebo and com-
tium. Erythrocyte degradation agnosis (malignancy), frequent recur- venography or ambulatory venous fort in warm weather, or because pression in complete ulcer healing.6,7
products and interstitial proteins are rence (ulcerative colitis or collagen pressures may be (rarely) requested some patients have hypersensitive Aspirin 300mg/day has also been
potent chemoattractants and pre- vascular disease) and non-healing when the findings of clinical and non- skin in the lipodermatosclerotic area show to speed ulcer healing, most
sumably represent the inflammatory (obesity). invasive examinations are insufficient adjacent to the ulcer or at the site of a likely due to its anti-inflammatory
signal responsible for leucocyte It must be noted that venous ulcers to provide complete diagnosis or as a previously healed ulcer. When begin- and antiplatelet effects.
recruitment. can transform into malignant ulcers part of a therapeutic endeavour such ning therapy, patients should be Topical antibiotics have been advo-
Causes of persistent venous hyper- — either squamous cell carcinoma or as thrombolysis and stenting. instructed to wear elastic compres- cated as a treatment of venous ulcer-
tension are: basal cell carcinoma. Suggestions of sion stockings for only as long as tol- ation for many years. However,
■ Primary valvular incompetence of malignancy include raised edges, an Non-operative treatment of CVI erable (perhaps only 10-15 minutes at unless an ulcer is actively infected,
the macrocirculation veins. irregular appearance, bleeding and Elevation of the lower extremities, first) and to gradually lengthen this topical or systematic antibiotics are
■ Secondary valvular incompetence prolonged failure to heal. Malignan- with the feet above the thighs when time. Occasionally, patients may ini- unnecessary, as bacterial colonisation
due to valve destruction in PTS. cies can be easily diagnosed through sitting and above the heart when tially need to be fitted with stockings of ulcers has little impact on healing.
Varicose veins
VARICOSE veins, or super- Ultrasound demonstrating mally high pulses of hydro- pressure on the more distal
ficial venous incompetence, incompetence at the dynamic pressure to be veins, venous dilation and
can lead to CVI. Patients saphenofemoral junction transmitted from the deep further venous incompe-
with lower-limb oedema and (significant being greater than system to the relatively tence, in a progressive fash-
superficial venous incompe- 0.5 seconds duration of unsupported superficial ion. When the hydrostatic
tence can be treated by sur- reflux). veins. The best-recognised forces of gravitational reflux
gical or endovenous laser connections between the are added to the hydrody-
therapies. superficial and the deep namic forces of muscular
venous systems are the contraction, they produce
Pathophysiology and saphenofemoral and localised blowouts, or vari-
clinical features saphenopopliteal junctions. cosities.
When the valves of the per- Incompetence of the check Varicose veins, telang-
forator veins become incom- valves at their termination iectatic blemishes, and
petent they permit abnor- causes increased hydrostatic dilated, tortuous, flat, blue-
30 | Australian Doctor | 1 August 2008 www.australiandoctor.com.au
AD_ 0 3 1 _ _ _ AUG0 1 _ 0 8 . P DF Pa ge 1 7 / 2 4 / 0 8 , 2 : 4 9 PM
green reticular veins are not Table 4: Varicose veins: from ablation of the saphe-
normal physical findings. indications for nous vein are as good as
They are evidence of venous intervention* those from conventional sur-
dysfunction. Telangiectasias gical treatment, and clinical
are defined as a confluence ■ Venous ulceration observations suggest that
of permanently dilated intra- ■ Pain and aching patients are much more
dermal venules of <1mm in comfortable after saphenous
■ Swelling secondary to
diameter. Reticular veins are ablation than after stripping.
superficial venous
defined as permanently
hypertension
dilated, bluish intradermal Surgical treatment of
veins, usually 1mm to <3mm ■ Bleeding chronic occlusions of the
in diameter. ■ Superficial iliac veins and the inferior
Longstanding venous dys- thrombophlebitis vena cava
function causes marked skin ■ Cosmetic Apart from DVTs, venous
changes, from woodiness occlusion may also develop
*Source: Bergan 20058
and fibrosis to lipoder- because of trauma or irradi-
matosclerosis (from ation, or as a result of exter-
haemosiderin deposition) nal compression of deep
and atrophie blanche (a con- veins by:
fluence of scarring from ■ Retroperitoneal fibrosis.
multiple episodes of skin ■ Tumours.
breakdown and poor heal- ■ Cysts.
ing occuring in severe dis- ■ Aneurysms.
ease). ■ Abnormally inserted
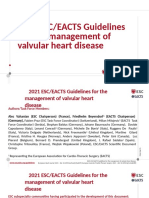
The aching pain is related An ablated long saphenous vein after endovascular laser treatment (lack of blue demonstrates no muscle (popliteal vein
to pressure of the dilated blood flow in that area). entrapment).
vessels on a network of ■ Fibrous bands or ligaments
somatic nerve fibres in adja- sclerotherapy are used to (soleal arch syndrome,
cent subcutaneous tissues remove other clusters of femoral vein compression
and the oedema caused by a varicose veins. Sclerotherapy by the inguinal ligament).
fluid shift from venous to without addressing the May-Thurner syndrome
interstitial compartments by saphenofemoral or (compression of the left
venous hypertension. saphenopopliteal reflux will common iliac vein by the
fail. overriding right common
Treatment Recent developments in iliac artery) is a rare but fre-
Extensive availability of treatment of the long quently overlooked cause of
duplex ultrasonography has saphenous vein have left iliofemoral venous
revealed another reason for focused on attempting to thrombosis.
intervening in varicose veins, minimise postoperative dis- The approach to any of
in addition to those listed in comfort while maintaining the above causes of proxi-
table 4 — deep venous func- the benefits of saphenous mal venous occlusion is to
tion is improved by superfi- vein ablation. Endovascu- consider endovascular tech-
cial venous surgery. lar laser treatment can be niques first, as the advances
Doppler evaluation and performed using local being made in this field are
duplex scanning have shown anaesthesia only, without a significantly decreasing the
that saphenofemoral junction groin incision. It causes number of patients requir-
reflux is present in 70% of rapid thermal electrocoag- ing open surgical recon-
symptomatic limbs selected for ulation of the vein wall and struction. Endovascular
surgery. In such limbs the its valves, which in turn techniques involve relatively
saphenous vein at the femoral causes total loss of vessel low-risk angioplasty and
junction must be treated. wall architecture, disinte- stenting to reopen a
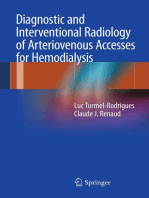
About 15% of patients are Varicose veins can lead to chronic venous insufficiency. gration and carbonisation. stenosed or occluded seg-
found to have short saphenous There is now level I evi- ment, whereas the open
vein incompetence, which Surgical removal of the or laser ablation of the vein dence indicating that such techniques of vein or syn-
9
requires flush ligation and long saphenous vein is now from the groin to the knee. treatment is beneficial. At thetic grafting bypass the
removal of some of the vein. performed by the stripping Supplement avulsions or 1-3 years, reported results affected vein.
Plavix + aspirin gives ACS †
patients added protection
against future CV events1–3 *
†ACS refers to acute coronary syndrome: UA/NSTEMI/STEMI. *Compared to aspirin alone.
For PBS Information refer to primary advertisement.
BEFORE PRESCRIBING PLEASE REVIEW PRODUCT INFORMATION IN THE PRIMARY ADVERTISEMENT IN THIS PUBLICATION. Plavix (clopidogrel 75 mg). References: 1. CURE Trial Investigators. N Engl J Med
2001;345(7): 494-502. 2. Sabatine MS, et al, for the CLARITY-TIMI 28 Investigators. N Engl J Med 2005; 352:1179-1189. 3. COMMIT (Clopidogrel and Metoprolol in Myocardial Infarction Trial) collaborative group. Lancet 2005;
366:1607-1621. sanofi-aventis australia pty ltd ABN 31 008 558 807, Talavera Corporate Centre, Building D, 12-24 Talavera Road, Macquarie Park, NSW 2113. Plavix is a registered trademark of sanofi-aventis.HSX0364/AD/2
www.australiandoctor.com.au 1 August 2008 | Australian Doctor | 31
AD_ 0 3 2 _ _ _ AUG0 1 _ 0 8 . P DF Pa ge 1 7 / 2 4 / 0 8 , 2 : 3 5 PM
How to treat – leg oedema
Lymphoedema
THE lymphatic vasculature Table 5: Classification one with limb swelling after with elevation.
consists of initial lymphatics, of lymphoedema apparent curative cancer treat- Pain is generally absent, but
the lymphatic pre-collectors, ment. in the presence of lymphangi-
lymphatic ducts and lymph Primary lymphoedema tis the limb may be acutely
nodes. The superficial system ■ Congenital lymphoedema: Postsurgical painful, with a diffuse, super-
collects lymph from the skin Lymph node dissection in the ficial burning sensation.
— autosomal dominant:
and subcutaneous tissue and setting of cancer therapy, and In advanced stages, skin
familial (Milroy’s
the deeper system drains sub- vascular surgery, particularly changes are characterised by
disease, lymphoedema-
fascial structures. femoral artery endarterectomy marked thickening and
distichiasis syndrome)
When lymphatic vessels are or lower-limb bypass surgery, coarseness. The limb is grossly
absent, underdeveloped or — autosomal recessive: may cause secondary lym- enlarged, skin creases become
obstructed, lymphatic flow syndrome associated phatic obstruction. enhanced, the limb takes on a
from the extremities is — sporadic mossy, cobblestone appear-
impeded and lymph accumu- ■ Lymphoedema praecox: Filariasis ance with a warty texture
lates. The resultant clinical pre- — familial (Meige disease) A nematode infection, filariasis (hyperkeratosis) and papillo-
sentation, lymphoedema, can accounts for the most cases of matosis develops.
— sporadic
affect any part of the body but secondary lymphoedema Lichenification of the toes
tends to target the arms and ■ Lymphoedema tarda worldwide. It should be con- develops and intermittent bac-
legs. About 300,000 Aus- sidered in any patient with terial infection occurs at sites
tralians have lymphoedema at Secondary lymphoedema lymphoedema who has trav- of skin fissures, minor trauma
any given time. elled or lived in an endemic or breakdown induced by
■ Post-surgical — lymph
area. interdigital fungal infection.
node dissection, vascular
Classification The skin may become broken
surgery
The simplest classification Chronic venous insufficiency and the lymph fluid can leak
requires differentiation ■ Neoplastic — intrinsic or Lymphoedema may compli- out onto the surface (lymph-
between primary and sec- extrinsic obstruction cate CVI that has resulted in orrhoea).
ondary causes. Impedence to ■ Parasitic — filariasis marked venous hypertension. Infections in the form of cel-
lymphatic flow may be due to ■ Post-infectious lulitis, lymphangitis and lym-
an inborn defect (primary) or Other causes phadenitis are common and
■ Post-traumatic
an acquired loss of lymphatic Other causes associated with ulceration may occur in
patency (secondary) (table 5). ■ Complicating chronic obstruction of lymphatic advanced stages, usually
venous insufficiency channels include: resulting from concomitant
Primary lymphoedema ■ Trauma. venous hypertension. In addi-
Primary lymphoedema can be ■ Tuberculosis. tion to their inherent danger,
Table 6: Differential
classified either according to ■ Contact dermatitis. infections further damage the
diagnosis of
the age of the patient when the ■ Rheumatoid arthritis. lymphatic system. Very rarely,
lymphoedema
oedema first appears, or by its ■ Pregnancy. in certain exceptionally severe
lymphangiographic appear- ■ Chronic venous ■ Subcutaneous injections of cases, lymphoedema untreated
ance. insufficiency drugs. over many years can lead to a
■ Post-phlebitic syndrome Autoimmune destruction form of cancer known as lym-
Patterns of lymphatic remains a controversial aeti- phangiosarcoma.
■ Reflex sympathetic
dysfunction ology. Lymphoedema manifesting
dystrophy
There are four patterns of lym- with sudden onset of swelling
phatic dysfunction: ■ Myxoedema Clinical features of one whole leg suggests
■ Hypoplasia (or obstruction) ■ Lipoedema Lymphoedema manifesting with sudden onset of swelling of one Typical clinical findings proximal obstruction, and a
of lymphatics distal to the ■ Malignant lymphoedema whole leg suggests proximal obstruction, and secondary causes include concentric calf oedema search is made for a secondary
inguinal nodes. such as a tumour must be excluded. with a loss of normal contour, cause. Pelvic causes of lym-
■ Obstruction of pelvic vessels, sparing at the level of the phatic obstruction such as
with or without obliteration predominance. There is pri- Milroy’s disease. The term of the draining lymph nodes. It ankle joint and significant tumour must be excluded.
of distal vessels. mary lymphatic valvular Meige disease is applied to the is almost always due to strep- hind-foot oedema relative to
■ Hyperplasia of lymphatic incompetence and an increased praecox familial form, also tococci (predominantly beta- the forefoot, yielding a ‘buf- Differential diagnosis
vessels. number of lymphatic channels, autosomal dominant. Autoso- haemolytic strains) although falo hump’ profile. The toes Table 6 lists the differential
■ Incompetent, dilated lym- with varicosities of the major mal recessive forms can some- Staphylococcus aureus and take on a ‘sausage’, or diagnoses of lymphoedema.
phatic channels (megalym- collecting vessels. Megalym- times occur. Gram-negative anaerobes have ‘squared-off’, appearance, CVI and PTS resulting in
phatics). phatics are associated with a Primary lymphoedema is also been implicated. In addi- accompanied by tense chronic venous hypertension
About one-third of cases are greater extent of involvement also associated with Turner tion, recurrent lymphangitis is oedema. are most readily confused
related to aplasia (absence of and a worse prognosis. syndrome, Noonan’s syn- a common complication of The unique changes of with lymphoedema. However,
lymphatic trunks), hypoplasia drome, yellow-nail syndrome, lymphoedema. Repeated bouts dermal and subdermal fibrosis the fluid distribution in CVI
(reduced number or calibre of Age of first appearance intestinal lymphangiectasia, of cellulitis may also exacer- (peau d’orange) and Stem- and PTS is different, being
lymphatic channels) or Congenital lymphoedema is lymphangiomyomatosis and bate the chronic oedema seen mer’s sign (an inability of the greatest in the ankle area and
obstruction of the distal lym- apparent at birth or becomes arteriovenous malformations. in CVI. soft tissues to tent the skin of least over the toes. Chronic
phatics, with relatively normal recognised during the first two Limb swelling may be the the interdigital webs) also venous hypertension is typi-
proximal vessels. Swelling is years of life. It represents presenting and major manifes- Tumour serve to distinguish lym- cally associated with:
usually bilateral and mild and about 15% of primary lymph- tation of congenital lymphatic Malignant cells may obstruct phoedema from other causes ■ Aching discomfort.
women are affected more fre- oedema cases. There is typi- malformations, either in a pure lymphatic vessels, inducing of chronic lower-limb ■ Chronic pruritus.
quently. The prognosis is cally aplasia or hypoplasia of form (eg, diffuse lymphan- lymphoedema directly or pre- oedema. ■ Hyperpigmentation.
good; after the first year of lymphatic structures. In rare gioma) or in combination with disposing the patient to bacte- Initially there is pitting ■ Dusky discolouration,
symptoms there is little exten- cases involvement of multiple a congenital vascular syn- rial lymphangitis. The most oedema, which may decrease with dependency, lipoder-
sion in the same limb or to limbs, genitalia or facial struc- drome, such as Klippel-Tré- common causes of lower- or disappear with elevation. matosclerosis and subcuta-
uninvolved extremities. How- tures may be seen. naunay syndrome (varicose extremity malignant lym- Increased fluid retention con- neous fat necrosis (panni-
ever, in about 40% of patients, Lymphoedema praecox is veins, excessive long bone phoedema are prostate cancer tributes to a sense of heavi- culitis).
affected limb girth continues most commonly first detected growth and vascular birth- in men and lymphoma in ness, and early fatigue of the ■ Ulceration (if advanced).
to increase gradually. at puberty but its appearance mark). women. limb is common. The skin Myxoedema may occur in
In more than 50% of cases may be delayed until the third Therapy against malignancy retains its normal texture but relation to thyroid dysfunc-
the defect primarily involves decade. It comprises about Secondary lymphoedema may also result in lym- may appear flushed, and tion when abnormal deposits
obstruction of the proximal 75% of cases and is typified Secondary lymphoedema phoedema. Oedema of the leg increased skin blood flow will of mucinous material accu-
lymphatics or nodes. There is by a hypolastic lymphangio- results from disruption or is comparatively common after result in an increased temper- mulate in the skin. In thyro-
possibly a slight female pre- graphic pattern, usually begin- obstruction of previously treatment of pelvic or genital ature of the limb. These fea- toxicosis, the process is focal,
dominance. Swelling tends to ning with foot and ankle normal lymphatic pathways cancer that involves pelvic or tures are quite typical of mild whereas in hypothyroidism,
be unilateral and severe, and swelling. by other disease processes or inguinal lymph node dissection disease. myxoedema is more gener-
the extent and degree is more Lymphoedema tarda typi- as a consequence of surgery or with or without adjuvant Over a period of years, or alised and is accompanied by:
likely to progress, with subse- cally manifests after age 35- radiotherapy. It is much more radiotherapy. Cancer itself with more moderate disease, ■ Roughening of the skin
quent involvement of the distal 40. The lymphatic channels common than primary lym- rarely presents with lym- there is thickening of the skin (palms, soles, elbows and
lymphatics. may be hypoplastic or hyper- phoedema. phoedema except in advanced and the limb may take on a knees).
A minority of patients have plastic. cases presenting late, such as woody (classic peau d’orange) ■ Brittle nails.
bilateral hyperplasia of the A family history is evident Infection prostate cancer, where venous appearance. Pitting is no ■ Dull thinning hair.
lymphatics or tortuous dilated in a minority of cases. The Recurrent episodes of bacterial obstruction may coexist. longer apparent. The oedema ■ Yellow-orange discoloura-
incompetent lymphatics congenital autosomal domi- lymphangitis cause obliteration Relapsed tumour should may extend more proximally tion of the skin.
(megalymphatics), with a male nant form is known as of the lymphatics and fibrosis always be considered in some- and may not diminish at night ■ Reduced sweat production.
32 | Australian Doctor | 1 August 2008 www.australiandoctor.com.au
AD_ 0 3 3 _ _ _ AUG0 1 _ 0 8 . P DF Pa ge 1 7 / 2 4 / 0 8 , 2 : 3 6 PM
Lipoedema is the accumu- tored using a gamma camera. Table 7: Treatment of cutaneous tissue. component of complete broad-spectrum antibiotics
lation of fluid and fat deposits Measurement of tracer uptake lymphoedema ■ Prevent infection. decongestive therapy. Gentle followed by more prolonged
under the skin, generally in within the lymph nodes after a The most common and cleansing followed by mois- courses of oral antibiotics.
the legs. It almost exclusively defined interval will distin- Non-surgical accepted treatments for lym- turising prevents cracking Lifelong prophylaxis may be
occurs in females and nor- guish lymphoedema from ■ Proper skin care — topical phoedema are sequential and fissuring. required in patients with
mally appears during puberty oedema of non-lymphatic emollients gradient pump therapy and Elevating the affected recurrent infections.
or pregnancy. The size of the origin. complete decongestive ther- limb lowers venous pressure
■ Manual lymphatic therapy
extremities cannot be reduced In primary lymphoedema, apy. Such combination ther- and therefore filtration, Surgery
by losing weight. The legs the channels are obliterated ■ Multi-layer, short-stretch apy results in the greatest allowing better lymph Surgical therapy is reserved for
may be very tender and ache or absent; in 10% they are bandaging overall reduction in limb drainage. those few patients who con-
around the knees. It charac- ectatic and incompetent. In ■ Exercise volume. Complete deconges- Intermittent biocompression tinue to experience unaccept-
teristically spares the feet and secondary lymphoedema the ■ Well-fitted compression tive therapy comprises skin can be accomplished with able function despite maximi-
does not change the appear- channels are dilated and the garments care, manual lymphatic mechanical pumps, but it is sation of conservative
ance of the skin, which distin- level of obstruction can be drainage, multilayer bandag- recommended that it be approaches. It comprises exci-
■ Intermittent, multi-
guishes it from lymphoedema. determined. In any form of ing, compressive garments applied at low pressures for sional or physiological tech-
compartmental pneumatic
People with lipoedema also lymphoedema, the appear- and exercise. no longer than 30-60 minutes. niques as well as liposuction.
compression pump
bruise easily. ance of tracer outside the Manual lymphatic Newer compression pump Excisional techniques
Malignancy can cause the main lymph routes, particu- Surgical drainage consists of gentle, garments provide compression include:
appearance or worsening of larly in the skin (dermal back- ■ Lymphatico-venous rhythmic massaging of the well into the trunk and/or ■ Circumferential excision of
lymphoedema. There is a ten- flow), indicates lymph reflux anastomosis skin to stimulate lymph abdomen and groin areas. the lymphoedematous tissue,
dency for rapid development and suggests proximal pro- ■ Excisional procedures flow. A typical session will Compression pump therapy followed by skin grafting.
and relentless progression, gression is delayed. Poor tran- involve drainage of the neck, should always be accompa- ■ Longitudinal removal of the
■ Liposuction
and pain may be a feature. sit of isotope from the injec- trunk and involved extrem- nied by effective manual lym- affected segment of skin and
tion site suggests hypoplasia ity (in that order). phatic drainage. subcutaneous tissue and pri-
Diagnosis/investigations of the peripheral lymphatic is not. The beneficial aspect Compression bandaging mary closure.
In the patient with an oede- system. of MRI or CT is in deter- involves applying several Drug treatment ■ Excision of subcutaneous
matous extremity in which mining the cause of sec- layers of padding and short- Diuretics are of little benefit tissue and tunnelling of a
lymphoedema is suspected, Direct contrast X-ray lympho- ondary lymphoedema. stretch bandages to the in lymphoedema because their dermal flap through the
diagnostic studies are used to graphy (lymphangiography) involved areas, which, main action is to limit capil- fascia into a muscular com-
establish the diagnosis, assess After the lymph vessels have Assessing the degree of during activity, enhances the lary filtration. Improvement partment of the leg.
lymphatic function and doc- been identified with a vital lymphoedema pumping action of the lymph in patients taking diuretics Physiological techniques
ument the degree or severity dye, a contrast medium is The two standard methods vessels, encourages lym- suggests that the predominant include:
of lymphoedema. administered directly into a for assessing the degree of phatic flow and softens cause of the oedema is not ■ Lympholymphatic anasto-
When the physical exami- peripheral lymphatic vessel. lymphoedema are measure- fluid-swollen areas. Short- lymphatic. mosis (autologous lymphatic
nation does not conclusively This form of investigation is ment of limb circumference stretch bandages are pre- The benefit of benzopy- grafts to bridge obstructed
support the diagnosis of lym- used rarely. and measurement of limb ferred over long-stretch ban- rones, such as coumarin or lymphatic segments).
phoedema (typically in mild volume displacement. The dages (such as those flavonoids, that theoretically ■ Lymphovenous shunt (anas-
cases), additional objective evi- CT and MRI latter, also known as water normally used to treat help remove excess proteins tomosis of lymphatic chan-
dence is required to confirm Both CT and MRI detect a displacement volumetry, sprains) to prevent a tourni- and associated fluid from the nels to veins).
lymphatic dysfunction. Initial characteristic ‘honeycomb’ involves placing the limb in quet effect. tissues remains unproved. ■ Lymphangioplasty with
investigators relied on lym- pattern in the subcutaneous a known volume of water; Regular exercise should enteromesenteric flap
phangiography but this pro- compartment that is not seen the volume of water that always accompany compres- Prevention of infection omental transfer (pedicled
cedure has now been largely with other causes of oedema. overflows is measured then sion bandaging. Dynamic Prevention of cellulitis or lym- portion of omentum trans-
replaced. In addition, there is the char- converted to mass. muscle contractions encour- phangitis is crucial to prevent posed to the affected limb).
acteristic absence of muscle age both passive and active deterioration in oedema.
Isotopic lymphoscintigraphy involvement in lym- Treatment drainage. Fungicidal agents between the
Isotopic lymphoscintigraphy phoedema. MRI is more Therapy for lymphoedema is Compression stockings can digits to control tinea pedis, References,
is now the investigation of informative than CT because best achieved by multiple be used initially for mild lym- and careful antiseptic dress- further reading and
choice for identifying oedema it can detect water. CT interrelated strategies (table 7). phoedema or substituted for ings after minor wounds, are online resources
of lymphatic origin. Radio- cannot localise the level of The goals of therapy are to: bandaging in advanced cases mandatory. Available on request from
labelled colloid or protein is obstruction or differentiate ■ Reduce limb size. after lymph volume has Bacterial infections should julian.mcallan@reedbusiness.
injected into the first web surgically correctable lym- ■ Preserve and improve the decreased. be aggressively treated, often com.au
space of each foot and moni- phoedema from that which quality of the skin and sub- Skin care is an important initially with an IV course of
Add Plavix early and continue long term so ACS 1
patients can enjoy rewarding events.
For PBS Information refer to primary advertisement.
BEFORE PRESCRIBING PLEASE REVIEW PRODUCT INFORMATION IN THE PRIMARY ADVERTISEMENT IN THIS PUBLICATION. Reference:
1. Plavix Approved Product Information, August 2007. sanofi-aventis australia pty ltd. ABN 31 008 558 807, Talavera Corporate Centre, Building D, 12-24
Talavera Road, Macquarie Park, NSW 2113. Plavix is a registered trademark of sanofi-aventis. AU.CL0.08.05.03 Saatchi & Saatchi Healthcare HSX0364/AD/3 1
www.australiandoctor.com.au 1 August 2008 | Australian Doctor | 33
AD_ 0 3 4 _ _ _ AUG0 1 _ 0 8 . P DF Pa ge 1 7 / 2 4 / 0 8 , 2 : 3 6 PM
How to treat – leg oedema
GP’s contribution
moderate pitting oedema to for clinical features specific to the above conditions were What investigations should be
knee level, with loss of calf lymphoedema (involvement excluded. Lymphoedema is performed, and in what
contour, and more hind- of the feet and toes, peau d’o- typically non-pitting order?
foot swelling compared range, inguinal lym- (although may be pitting in The initial investigation
with ankle swelling. The phadenopathy) are also indi- the early stage) and age pre- should be a venous incompe-
calf is non-tender, with a cated. cludes a primary cause of tence scan and a venous
flushed appearance of the lymphoedema. duplex ultrasound scan to
skin and a circumference What are the diagnostic A secondary obstructive exclude venous incompetence
DR DAMIEN BRAY
3cm greater than the right. possibilities with Wendy’s cause typically involves the and prior or current deep
Cronulla, NSW
two-week history of leg entire leg. and/or superficial vein throm-
Questions for the author oedema? A subclinical leak or even bosis, because these conditions
Case study What further physical The finding of a unilateral rupture of a Baker’s cyst or a are far more common than
WENDY, 64, attends your examination should be per- swollen leg more commonly minor calf muscle tear lymphoedema. Ultrasound
surgery with a two-week formed today? implicates a local cause such should also be considered. will also exclude a Baker’s
history of a swollen left leg. A general physical exam- as venous incompetence or Uncontrolled systemic cyst or calf muscle tear.
She is a non-smoker and ination should always be venous hypertension. The hypertension will also pro- Blood tests to exclude renal,
takes raloxifene for osteo- performed. Clinical assess- ease as well as thyroid history of puffy ankles in hot mote lower limb swelling, liver and thyroid disease
porosis and ramipril for ment of general causes examination should be per- weather or with prolonged occasionally in an asymmet- should also be performed. A
hypertension. Her leg is not focuses on blood pressure formed. standing suggests a degree of rical fashion, particularly if protein electrophoretogram is
painful and has never been and heart rate, cardiovas- It is always important to venous incompetence. It is there is unilateral venous dis- also helpful.
very swollen before, cular examination looking evaluate the lower-limb pulses also important to exclude a ease such as varicose veins. Lymphoedema is best
although both ankles can for signs of ventricular (normal arterial circulation venous thrombotic event, as One should also consider excluded by performing
get “a bit puffy” in hot (right and/or left) dysfunc- will allow compression to be this is an acute medical general causes such as car- nuclear lymphoscintigraphy.
weather or with prolonged tion and valvular disease. used safely). Local assessment emergency. diac dysfunction, liver and If positive, an abdomino-
standing. Examination to exclude for signs of venous hyperten- Lymphoedema would also renal disease, and thyroid pelvic CT scan for obstructive
Examination reveals chronic liver or renal dis- sion and varicose veins and need to be considered after disease. causes is the next step.
INSTRUCTIONS
How to Treat Quiz Complete this quiz online and fill in the GP evaluation form to earn 2 CPD or PDP points. We no longer accept quizzes
by post or fax.
The mark required to obtain points is 80%. Please note that some questions have more than one correct
answer.
Leg oedema — 1 August 2008 ONLINE ONLY
www.australiandoctor.com.au/cpd/ for immediate feedback
1. Linda, 45, presents with pain and swelling stockings and appropriate treatment of the DVT decade of life and is typified by a
of the left calf for the past few days. She has with anticoagulants 6. Which TWO statements regarding hyperplasia of the lymphatic vessels
been in a below-knee cast for a left ankle b) Accepted anticoagulant therapy for venous management of CVI are correct? d) In lymphoedema tarda, which typically
fracture up until one week ago. Which TWO thromboembolism is either continuous IV a) Compression therapy remains the primary manifests after age 35-40, the lymphatic
statements regarding the clinical heparin or subcutaneous (SC) enoxaparin, then treatment for CVI channels may be hypoplastic or hyperplastic
presentation of DVT are correct? changing to oral warfarin b) Diuretics are very helpful in reducing the
a) The diagnosis of DVT based on clinical signs c) Patients with proximal thrombosis need IV or oedema of CVI 9. Which THREE statements about
and symptoms alone is highly accurate SC heparin followed by warfarin for up to six c) Arterial disease should be considered before assessing lymphoedema are correct?
b) Up to half of patients with acute DVT may months proceeding with compression therapy for CVI a) Typical clinical findings in lymphoedema
lack any specific sign or symptom d) Indications for vena caval filters include d) Topical antibiotics are useful in the treatment include concentric calf oedema with a loss of
c) Signs of DVT include pain with passive recurrent pulmonary embolism despite of venous ulceration to prevent development of normal contour, significant hind-foot oedema
plantar-flexion of the foot, known as Homans’ adequate anticoagulation infection relative to the forefoot and a ‘sausage’
sign appearance of the toes
d) Many pulmonary emboli may be clinically 4. Which TWO statements regarding the 7. Dolores, a 55-year-old teacher, consults b) Lymphoedema can be confused with
silent post-thrombotic syndrome (PTS) are you regarding long-standing bilateral oedema due to CVI or PTS; however, the fluid
correct? varicose veins. She is troubled by aching distribution in CVI and PTS is different, being
2. After further history and examination you a) PTS typically occurs within the first two years legs and is also concerned about their greatest over the ankles and least over the toes
suspect Linda has a DVT. Which TWO of the initial episode of DVT cosmetic appearance. Which TWO c) In lymphoedema manifesting with sudden
statements about investigating DVT are b) Risk factors for PTS appear to include statements regarding superficial venous onset of swelling of one whole leg, pelvic
correct? increased BMI incompetence are correct? causes of lymphatic obstruction must be
a) Duplex ultrasonography is highly accurate in c) PTS typically presents with pain, oedema, a) Telangiectatic blemishes and dilated, excluded
detecting DVT of the iliac veins as well as of the hyperpigmentation and/or ulceration tortuous, flat, blue-green reticular veins are d) Direct-contrast X-ray lymphography is the
lower-limb veins d) Wearing compression stockings long term normal physical findings investigation of choice for identifying
b) D-dimer assays are highly specific as well as has not been found to reduce the risk of b) Reticular veins are defined as permanently lymphoedema of lymphatic origin
highly sensitive for DVT development of PTS dilated, bluish intradermal veins, usually 1mm
c) The high sensitivity of D-dimer to <3mm in diameter 10. Which TWO statements regarding the
measurements makes it theoretically possible to 5. Which THREE statements about chronic c) Varicose veins, while a significant cosmetic treatment of lymphoedema are correct?
exclude a DVT on the basis of a negative result, venous insufficiency (CVI) are correct? issue, do not lead to CVI a) Combination therapy with sequential-
as long as the patient is in a low-risk group a) CVI is now thought of as a disease of chronic d) Deep venous function may be improved by gradient pump therapy and complete
d) Patients with recurrent DVT or DVTs involving inflammation superficial venous surgery decongestive therapy results in the greatest
more than the tibial vessels should be b) When examining the patient with CVI the overall reduction in limb volume
evaluated for a thrombophilia long and short saphenous veins should be 8. Which TWO statements regarding b) Long-stretch bandages are preferred over
palpated and tested for a cough impulse lymphoedema are correct? short-stretch bandages in compression
3. Duplex ultrasonography confirms that c) Investigation of CVI is best performed with a) Primary lymphoedema is much more therapy for lymphoedema
Linda has an isolated calf DVT. Which venography common than secondary lymphoedema c) Bacterial infections need to be treated
THREE statements about managing DVT are d) Raised edges, an irregular appearance, b) In congenital lymphoedema there is typically aggressively in patients with lymphoedema
correct? bleeding, and prolonged failure of a venous aplasia or hypoplasia of lymphatic structures d) Benzopyrones, such as coumarin or
a) In the acute DVT setting, lower-limb oedema ulcer to heal raise the suspicion of a malignant c) Lymphoedema praecox is most flavonoids, have been proven to be of benefit
can be treated with graduated compression ulcer commonly first detected in the third in lymphoedema
CPD QUIZ UPDATE
The RACGP now requires that a brief GP evaluation form be completed with every quiz to obtain category 2 CPD or PDP points for the 2008-10 triennium. You
HOW TO TREAT Editor: Dr Wendy Morgan
can complete this online along with the quiz at www.australiandoctor.com.au. Because this is a requirement, we are no longer able to accept the quiz by post
Co-ordinator: Julian McAllan
or fax. However, we have included the quiz questions here for those who like to prepare the answers before completing the quiz online.
Quiz: Dr Wendy Morgan
NEXT WEEK Newer, more sensitive tests and recent population-based studies suggest the prevalence of coeliac disease is 10 times more common than previously thought, and ‘silent’ coeliac disease about
seven times more common than symptomatic coeliac disease. With potential sequelae for undiagnosed/untreated disease, including a 20-fold increased risk of solid malignancies and an 80-fold increased risk
of intestinal lymphoma, it’s time to revisit the diagnosis and management of this condition with next week’s How to Treat on this topic. The authors are Associate Professor Warwick Selby, senior visiting
gastroenterologist, AW Morrow Gastroenterology and Liver Centre, Royal Prince Alfred Hospital, Camperdown, NSW; and clinical associate professor, central clinical school, faculty of medicine, University of
Sydney, NSW; and Dr John Darke, senior medical registrar and gastroenterology advanced trainee at Hornsby Hospital, Hornsby, NSW.
34 | Australian Doctor | 1 August 2008 www.australiandoctor.com.au
You might also like
- Rastelli Operation GuideDocument10 pagesRastelli Operation Guidecarvalho.tr4270No ratings yet
- Aki 3Document10 pagesAki 3Verghese GeorgeNo ratings yet
- 18 - CHD ICU Management - Shunt LesionsDocument15 pages18 - CHD ICU Management - Shunt LesionsRAM SOFTWARENo ratings yet
- Perioperative and Anesthetic Considerations On Total Anomalous Pulmonary Venous ConnectionDocument7 pagesPerioperative and Anesthetic Considerations On Total Anomalous Pulmonary Venous ConnectionBeatriz Itzel RománNo ratings yet
- Ehab 607Document3 pagesEhab 607陈诗哲No ratings yet
- HDO Leaflet PTDocument12 pagesHDO Leaflet PTErickson Fabian CastilloNo ratings yet
- 1 s2.0 S2590093522000224 MainDocument9 pages1 s2.0 S2590093522000224 MainSara TeixeiraNo ratings yet
- Cirsoid Aneurysm OF THE Uterus: Specific Arteriographic: Read As I8o/oo Mm. HG But Fellto Io/8o MMDocument7 pagesCirsoid Aneurysm OF THE Uterus: Specific Arteriographic: Read As I8o/oo Mm. HG But Fellto Io/8o MMLouis HadiyantoNo ratings yet
- Minimally Invasive Cardiac Surgery in Lucknow - Dr. Gauranga MajumdarDocument3 pagesMinimally Invasive Cardiac Surgery in Lucknow - Dr. Gauranga MajumdarBest Heart Bypass Surgery Dr. Gauranga MajumdarNo ratings yet
- Hemodialysis Vascular Access Morbidity1: HaroldDocument13 pagesHemodialysis Vascular Access Morbidity1: Harolderikazoku moNo ratings yet
- HeartViews224249-5914153 162541Document7 pagesHeartViews224249-5914153 162541hosameldin ahmedNo ratings yet
- Drill of The Month: Developed by Michael LindsayDocument52 pagesDrill of The Month: Developed by Michael LindsayanjanbsNo ratings yet
- CNS CNS CNSDocument46 pagesCNS CNS CNSqnmx7br6dsNo ratings yet
- Gastric and Gallbladder DiseasesDocument1 pageGastric and Gallbladder DiseasesHarsha Vardhan Reddy AlaNo ratings yet
- RDW Levels Associated With Venous Thrombosis RiskDocument6 pagesRDW Levels Associated With Venous Thrombosis RiskJicko Street HooligansNo ratings yet
- Drill of The Month: An Overview of Ventricular Assist Devices & Pre Hospital ManagementDocument52 pagesDrill of The Month: An Overview of Ventricular Assist Devices & Pre Hospital ManagementRina Iriany ZakariaNo ratings yet
- Leg Ischemia Post VaricocelectomyDocument4 pagesLeg Ischemia Post VaricocelectomyAn DiKa Bado PNo ratings yet
- Step-by-Step Guide to DVT Ultrasound Exam of Lower ExtremitiesDocument37 pagesStep-by-Step Guide to DVT Ultrasound Exam of Lower ExtremitiesEL SHITANo ratings yet
- EACVI expert consensus on adult transthoracic echo reportingDocument10 pagesEACVI expert consensus on adult transthoracic echo reportingEghet SilviuNo ratings yet
- Mindray Epiphany 12 Lead ECG Partnership - 7030revaDocument2 pagesMindray Epiphany 12 Lead ECG Partnership - 7030revaKatia DominguezNo ratings yet
- J JCHF 2017 06 012 FullDocument10 pagesJ JCHF 2017 06 012 FullDiana HyltonNo ratings yet
- VSDDocument34 pagesVSDMerlina Wijayawati100% (2)
- Homework #2: What Is Civ?Document5 pagesHomework #2: What Is Civ?api-702934667No ratings yet
- (Journal of Cardiovascular Emergencies) JCE - A New Perspective For Cardiovascular EmergenciesDocument2 pages(Journal of Cardiovascular Emergencies) JCE - A New Perspective For Cardiovascular EmergenciesVeronika AtaNo ratings yet
- Pi Is 0022522314001962Document4 pagesPi Is 0022522314001962Yosephus GorisNo ratings yet
- Vascular MalformationsDocument28 pagesVascular MalformationsMhinory Oct100% (1)
- Our Lady of Fatima University College of Medicine Clinical Clerkship Summary of Learning ExperiencesDocument3 pagesOur Lady of Fatima University College of Medicine Clinical Clerkship Summary of Learning ExperiencesrenzNo ratings yet
- The HeartDocument58 pagesThe HeartJULIUS NAKANYALANo ratings yet
- Ventricular Assist Devices: K. Nirmala SSN College of EngineeringDocument40 pagesVentricular Assist Devices: K. Nirmala SSN College of EngineeringNivetha RavikumarNo ratings yet
- Alvarez2007 Veine de GalienDocument18 pagesAlvarez2007 Veine de GalienModou NianeNo ratings yet
- Complete Atrioventricular Canal (CAVC)Document4 pagesComplete Atrioventricular Canal (CAVC)vivid1980No ratings yet
- Tumor Kanker TiroidDocument9 pagesTumor Kanker TiroidyuliantoNo ratings yet
- Soleclerkshiplong 2Document3 pagesSoleclerkshiplong 2Jovcel ObcenaNo ratings yet
- AV Fistula ExamDocument5 pagesAV Fistula Examsantosh subediNo ratings yet
- Doppler-Atlas VasospasmDocument5 pagesDoppler-Atlas VasospasmdanielNo ratings yet
- 10 10 19 Heart Failure-Lvad Cardiomems Topic DiscussionDocument4 pages10 10 19 Heart Failure-Lvad Cardiomems Topic Discussionapi-493355126No ratings yet
- Varises Internasional JurnalDocument18 pagesVarises Internasional JurnalAyu WulandariNo ratings yet
- Deep Vein Thrombosis (DVT): Causes, Symptoms and TreatmentDocument12 pagesDeep Vein Thrombosis (DVT): Causes, Symptoms and TreatmentJohn Jacob100% (1)
- s13089 022 00286 2Document11 pagess13089 022 00286 2Maudiel BrionesNo ratings yet
- Congenital Cardiac Surgery CutDocument4 pagesCongenital Cardiac Surgery CutNasrullah UllahNo ratings yet
- PeripheralDocument7 pagesPeripheralerdynNo ratings yet
- Edwards SVV HandoutDocument2 pagesEdwards SVV HandoutossinNo ratings yet
- Diagnostic Test LeukimaDocument8 pagesDiagnostic Test LeukimaIshmael SolamilloNo ratings yet
- Zwab 128Document9 pagesZwab 128William ChokNo ratings yet
- 2019 Lvad Echo BouchezDocument10 pages2019 Lvad Echo Bouchezsimoncalle1No ratings yet
- Podlesnikar2018 Article CardiovascularMagneticResonancDocument16 pagesPodlesnikar2018 Article CardiovascularMagneticResonancAhmer Yesi FebrianaNo ratings yet
- Computer-Assisted Transcatheter Heart Valve Implantation in Valve-in-Valve ProceduresDocument8 pagesComputer-Assisted Transcatheter Heart Valve Implantation in Valve-in-Valve ProceduresrédaNo ratings yet
- Indications For Hemodynamic MonitoringDocument6 pagesIndications For Hemodynamic Monitoringmerin sunilNo ratings yet
- Acute Respiratory Distress Syndrome: Diagnosis and Management p730Document9 pagesAcute Respiratory Distress Syndrome: Diagnosis and Management p730Ahmed AlhalwajiNo ratings yet
- MR Second Za PredevanjeDocument32 pagesMR Second Za Predevanjedeni2razmoskiNo ratings yet
- Venous ThromboembolismDocument28 pagesVenous ThromboembolismValeria MolinaNo ratings yet
- Echocardiography & Color Doppler Report Measurements Absolute Value Normals Absolute / MDocument3 pagesEchocardiography & Color Doppler Report Measurements Absolute Value Normals Absolute / MAmol PandeyNo ratings yet
- Valvulopatii Конвертирован Конвертирован 1Document129 pagesValvulopatii Конвертирован Конвертирован 1Ina CazacliuNo ratings yet
- Tavi VS Valvula Rapida ImplanteDocument13 pagesTavi VS Valvula Rapida ImplanteUTI CRUZ AZULNo ratings yet
- Swelling in LegDocument3 pagesSwelling in LegNeeraj SethiNo ratings yet
- A Comparative Review of The Outcomes of Using.5Document6 pagesA Comparative Review of The Outcomes of Using.5Harish SubramanianNo ratings yet
- Diagnostic and Interventional Radiology of Arteriovenous Accesses for HemodialysisFrom EverandDiagnostic and Interventional Radiology of Arteriovenous Accesses for HemodialysisNo ratings yet
- AmyloidosisDocument15 pagesAmyloidosisNicoletta OrphanouNo ratings yet
- Cirrhosis 2008. LANCETDocument14 pagesCirrhosis 2008. LANCETMaría José Klinger Del VillarNo ratings yet
- Schiller ABPM - BR-102 PLUS PWADocument4 pagesSchiller ABPM - BR-102 PLUS PWAMirko BoticaNo ratings yet
- Caused by Regional Abnormalities: Edema PrimarilyDocument8 pagesCaused by Regional Abnormalities: Edema PrimarilyEgorSazhaevNo ratings yet
- HowtoDiagnoseLegEdemafamily_physician_sept2008Document8 pagesHowtoDiagnoseLegEdemafamily_physician_sept2008Rafan AddisNo ratings yet
- LEGS-MATTER-PATIENTS-SWOLLEN-LEGS-FEET-A4Document2 pagesLEGS-MATTER-PATIENTS-SWOLLEN-LEGS-FEET-A4Rafan AddisNo ratings yet
- Lower Extremity Edema – Causes, Treatment, and PreventionDocument10 pagesLower Extremity Edema – Causes, Treatment, and PreventionRafan AddisNo ratings yet
- Oedema Assessment - PhysiopediaDocument12 pagesOedema Assessment - PhysiopediaRafan AddisNo ratings yet
- LEEdemaDocument2 pagesLEEdemaRafan AddisNo ratings yet
- Selected Differential Diagnosis of Bilateral Lower Extremity EdemaDocument1 pageSelected Differential Diagnosis of Bilateral Lower Extremity EdemaRafan AddisNo ratings yet
- Leg edema assessment and management - articleDocument11 pagesLeg edema assessment and management - articleRafan AddisNo ratings yet
- Edema_ Types, causes, symptoms, and treatment (1)Document13 pagesEdema_ Types, causes, symptoms, and treatment (1)Rafan AddisNo ratings yet
- Clinical manifestations and evaluation of edema in adultsDocument9 pagesClinical manifestations and evaluation of edema in adultsRafan AddisNo ratings yet
- Approach to leg edema _ Italian Journal of MedicineDocument1 pageApproach to leg edema _ Italian Journal of MedicineRafan AddisNo ratings yet
- Edema - Symptoms and causes - Mayo Clinic (2)Document2 pagesEdema - Symptoms and causes - Mayo Clinic (2)Rafan AddisNo ratings yet
- Postpartum Head To Toe Assessment/ Bubble HeDocument2 pagesPostpartum Head To Toe Assessment/ Bubble HeJariel CatacutanNo ratings yet
- Komplikasi - Compartment Syndrome-A Very Rare Complication Where The Fluid That Is Used To Irrigate TheDocument3 pagesKomplikasi - Compartment Syndrome-A Very Rare Complication Where The Fluid That Is Used To Irrigate TheNanang YuliantoNo ratings yet
- Vulvectomy: Patient Information Patient InformationDocument11 pagesVulvectomy: Patient Information Patient InformationMega FebrianaNo ratings yet
- DVT NotesDocument3 pagesDVT NotesTodd EvansNo ratings yet
- Standard precautions nurse colleagueDocument22 pagesStandard precautions nurse colleagueMary Hiromi MizushimaNo ratings yet
- Fragmin PIDocument17 pagesFragmin PIgclisantiNo ratings yet
- Creating Intuitive Interactive Dashboards With The Adf Data Visualization ComponentsDocument74 pagesCreating Intuitive Interactive Dashboards With The Adf Data Visualization ComponentsnandhulnNo ratings yet
- Koran Pasien PJT LT4 2 Feb 2023Document9 pagesKoran Pasien PJT LT4 2 Feb 2023maspul lamuruprintNo ratings yet
- D Di2Document5 pagesD Di2ARIF AHAMMED P100% (1)
- Latihan Nclex 5Document4 pagesLatihan Nclex 5Whina IndrianaNo ratings yet
- Clinical Trial Details (PDF Generation Date:-Thu, 16 Jun 2022 08:33:57 GMT)Document11 pagesClinical Trial Details (PDF Generation Date:-Thu, 16 Jun 2022 08:33:57 GMT)Dr Meenakshi ParwaniNo ratings yet
- MS General Surgery Question BankDocument98 pagesMS General Surgery Question BankPrashant Singh100% (10)
- Skeletal TractionDocument11 pagesSkeletal Tractionpolarbear121212No ratings yet
- NCM 112 EvalDocument16 pagesNCM 112 EvalMartin T ManuelNo ratings yet
- Post-Operative Care: DR - Tehreem Nasir MBBS, RMPDocument58 pagesPost-Operative Care: DR - Tehreem Nasir MBBS, RMPAhmed SaeedNo ratings yet
- Nizatul Mumtazah - 1706013371 - Remedial Jurnal DVTDocument13 pagesNizatul Mumtazah - 1706013371 - Remedial Jurnal DVTnizaNo ratings yet
- Erythema Marginatum Chorea: Migratory Polyarthritis Cardiac Involvement Subcutaneous NodulesDocument27 pagesErythema Marginatum Chorea: Migratory Polyarthritis Cardiac Involvement Subcutaneous NodulesMisbah KaleemNo ratings yet
- Amboss:CardioDocument18 pagesAmboss:CardioNicole Juliette CCNo ratings yet
- Rundown ISMI Hotti 2016Document5 pagesRundown ISMI Hotti 2016Wahyu PurnomoNo ratings yet
- Venous Thromboembolic DiseaseDocument262 pagesVenous Thromboembolic DiseasesamNo ratings yet
- Coercive MeasuresDocument1 pageCoercive Measuresapi-543558169No ratings yet
- DIVITI Slide Prophylaxis VTE SPPD Ringkas-1Document11 pagesDIVITI Slide Prophylaxis VTE SPPD Ringkas-1Fera NurrizaNo ratings yet
- Nursing Care Plan in CVADocument5 pagesNursing Care Plan in CVAdiahayumustikaNo ratings yet
- The Purpose of This Manual: VP 500 DescriptionDocument11 pagesThe Purpose of This Manual: VP 500 DescriptionCarlos JuniorNo ratings yet
- Venous Thromboembolism Disease Risks, Symptoms and TreatmentDocument25 pagesVenous Thromboembolism Disease Risks, Symptoms and TreatmentOmar AbdillahiNo ratings yet
- LP Vulnus Laceratum PDFDocument8 pagesLP Vulnus Laceratum PDFAlfrida Ade BunapaNo ratings yet
- Varicose VeinsDocument8 pagesVaricose VeinshalesNo ratings yet
- Pathology Mnemonics - Medical Students Wonder - Medical Powerpoint Presentations Videos Ebooks and OthersDocument7 pagesPathology Mnemonics - Medical Students Wonder - Medical Powerpoint Presentations Videos Ebooks and OthersBhopesh KadianNo ratings yet
- Varicose Vein ExaminationDocument9 pagesVaricose Vein ExaminationYS NateNo ratings yet
- Deep Vein Thrombosis in Pediatric PatientsDocument9 pagesDeep Vein Thrombosis in Pediatric Patientsemilce beltran100% (1)