You might also like
- Cardiac Surgical Operative AtlasFrom EverandCardiac Surgical Operative AtlasThorsten WahlersNo ratings yet
- Arteriography of Coronary Disease at Clinical Onset Reveals Severe Disease in ManyDocument8 pagesArteriography of Coronary Disease at Clinical Onset Reveals Severe Disease in ManyNova SipahutarNo ratings yet
- Subarachnoid Hemorrhage: Beyond Aneurysms: Carrie P. Marder Vinod Narla James R. Fink Kathleen R. Tozer FinkDocument13 pagesSubarachnoid Hemorrhage: Beyond Aneurysms: Carrie P. Marder Vinod Narla James R. Fink Kathleen R. Tozer FinkClaire FowlNo ratings yet
- 1.2 Med - PE CardioDocument13 pages1.2 Med - PE CardioDan FabrosNo ratings yet
- Arterial Anatomy of The Female Genital Tract - Variations and Relevance To Transcatheter Embolization of The UterusDocument12 pagesArterial Anatomy of The Female Genital Tract - Variations and Relevance To Transcatheter Embolization of The UterusFelipe Wei Ning WangNo ratings yet
- Arterial Line Waveform Interpretation UHL Childrens Intensive Care GuidelineDocument5 pagesArterial Line Waveform Interpretation UHL Childrens Intensive Care GuidelineDhony100% (1)
- ICBA NotesDocument60 pagesICBA NotesAndrew EldeiryNo ratings yet
- ARRYTHMIASDocument3 pagesARRYTHMIASitstheboyjayyNo ratings yet
- PHA 618: Human Physiology and Pathophysiology Cardiovascular ExercisesDocument2 pagesPHA 618: Human Physiology and Pathophysiology Cardiovascular Exerciseskaila lunaNo ratings yet
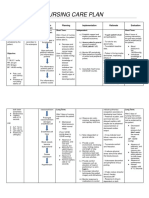
- NCPDocument2 pagesNCPBella SalikNo ratings yet
- Case Apsc 2023 - FdaDocument18 pagesCase Apsc 2023 - FdaFariz DwikyNo ratings yet
- Physiology Revision CVS Part 3Document20 pagesPhysiology Revision CVS Part 3Gauri BendreNo ratings yet
- Ajr 127 1 143Document11 pagesAjr 127 1 143Khalvia KhairinNo ratings yet
- SF1-Lecture-03 - Body Fluids and Circulation - NotesDocument7 pagesSF1-Lecture-03 - Body Fluids and Circulation - Notesdisha shuklaNo ratings yet
- How To Examine The Heart and Blood VesselsDocument62 pagesHow To Examine The Heart and Blood Vesselsapi-3757039No ratings yet
- Evaluate PDFDocument3 pagesEvaluate PDFMc SantosNo ratings yet
- Graphic Organizer-Heart Murmur Elvis Baquero 7mo CDocument3 pagesGraphic Organizer-Heart Murmur Elvis Baquero 7mo CEduardo AcostaNo ratings yet
- BedahDocument1 pageBedahLovely MeNo ratings yet
- Subarachnoid Hemorrhage: Beyond Aneurysms: Carrie P. Marder Vinod Narla James R. Fink Kathleen R. Tozer FinkDocument13 pagesSubarachnoid Hemorrhage: Beyond Aneurysms: Carrie P. Marder Vinod Narla James R. Fink Kathleen R. Tozer FinkDaylamiNo ratings yet
- Cardiovascular SystemDocument13 pagesCardiovascular SystemKatrina Marie MandapNo ratings yet
- Tugas PDDocument59 pagesTugas PDfirmanNo ratings yet
- Blood Pressure MeasurementDocument23 pagesBlood Pressure MeasurementHữu Tài NguyễnNo ratings yet
- Gynaecology History TakingDocument2 pagesGynaecology History TakingSyaza SyedNo ratings yet
- advanced physiology notesDocument4 pagesadvanced physiology notesapi-738816033No ratings yet
- Blood Counting TechniquesDocument12 pagesBlood Counting TechniquesJill ArciagaNo ratings yet
- Diagnosing Dyspnea with a Diagnostic TreeDocument2 pagesDiagnosing Dyspnea with a Diagnostic TreeDiana CarolinaNo ratings yet
- Anatomy Physiology of The CV SystemDocument29 pagesAnatomy Physiology of The CV SystemMaedehNo ratings yet
- The HeartDocument58 pagesThe HeartJULIUS NAKANYALANo ratings yet
- Motor Vehicular Accident, Extricated W/ Minimal Difficulty After 30 Mins: #1: 27-Year-Old Male, Disoriented & Drowsy #2: 23-Year Old Male, UnresponsiveDocument1 pageMotor Vehicular Accident, Extricated W/ Minimal Difficulty After 30 Mins: #1: 27-Year-Old Male, Disoriented & Drowsy #2: 23-Year Old Male, UnresponsiveMarian Joyce Princess YuqueNo ratings yet
- Blood Pressure: DR Nilesh Kate MBBS, MDDocument58 pagesBlood Pressure: DR Nilesh Kate MBBS, MDHiroj BagdeNo ratings yet
- Nursing Care Plan For HELLP SyndromeDocument17 pagesNursing Care Plan For HELLP SyndromeRosemarie Carpio75% (4)
- Isolated Diffuse Ground-Glass Opacity in Thoracic CTDocument10 pagesIsolated Diffuse Ground-Glass Opacity in Thoracic CTAyşe BanuNo ratings yet
- Echo-Doppler Assessment of Vascular Access for HemodialysisDocument34 pagesEcho-Doppler Assessment of Vascular Access for HemodialysisVio VioNo ratings yet
- CARDIAC TUMORS Approach To ManagementDocument12 pagesCARDIAC TUMORS Approach To ManagementAnkit GulatiNo ratings yet
- CVS-01 Examination & Short CasesDocument9 pagesCVS-01 Examination & Short Casesem khanNo ratings yet
- Rastelli Operation GuideDocument10 pagesRastelli Operation Guidecarvalho.tr4270No ratings yet
- CHAP 10 FORM 4 BiologyDocument8 pagesCHAP 10 FORM 4 BiologyCrescentiaNo ratings yet
- CNS CNS CNSDocument46 pagesCNS CNS CNSqnmx7br6dsNo ratings yet
- 6 Head and Neck Trauma - Thoracic and Cardiovascular TraumaDocument7 pages6 Head and Neck Trauma - Thoracic and Cardiovascular TraumaMyrtle Yvonne RagubNo ratings yet
- Belloni Et Al 2012 Mri of CardiomyopathyDocument11 pagesBelloni Et Al 2012 Mri of CardiomyopathyRadiologyNo ratings yet
- Miller Shah 2012 Isolated Diffuse Ground Glass Opacity in Thoracic CT Causes and Clinical PresentationsDocument10 pagesMiller Shah 2012 Isolated Diffuse Ground Glass Opacity in Thoracic CT Causes and Clinical PresentationsAndrea PescosolidoNo ratings yet
- Blood Flow ImagesDocument86 pagesBlood Flow ImagesDeva ChiruNo ratings yet
- BRONCHO ALVEOLAR CARCINOMA DIFFERENTIAL DIAGNOSISDocument3 pagesBRONCHO ALVEOLAR CARCINOMA DIFFERENTIAL DIAGNOSISmarielleaudreeyNo ratings yet
- Cerebral Circulation in Moyamoya Disease: A Clinical Study Using Transcranial Doppler SonographyDocument8 pagesCerebral Circulation in Moyamoya Disease: A Clinical Study Using Transcranial Doppler SonographyDewi SartikaNo ratings yet
- MBChB Year 5 Surgery: Arterial AneurysmsDocument1 pageMBChB Year 5 Surgery: Arterial AneurysmsJason HarryNo ratings yet
- CARDIAC TUMORS TransDocument12 pagesCARDIAC TUMORS TransjeccomNo ratings yet
- Diagnostic Test FinalDocument5 pagesDiagnostic Test FinalDivynne MadeloNo ratings yet
- Cardiac Troponin and Defining Myocardial Infarction: Thomas E. Kaier, Bashir Alaour, and Michael MarberDocument13 pagesCardiac Troponin and Defining Myocardial Infarction: Thomas E. Kaier, Bashir Alaour, and Michael MarberwiwiNo ratings yet
- Abnormal Circulatory Shock PathophysiologyDocument4 pagesAbnormal Circulatory Shock PathophysiologydonnaNo ratings yet
- 5 Basic EchoDocument64 pages5 Basic Echoola adelNo ratings yet
- Haemorrhoids: Acute PresentationsDocument1 pageHaemorrhoids: Acute PresentationsMuhammad AkhyarNo ratings yet
- Rhythms of Death MD1TALKDocument1 pageRhythms of Death MD1TALKAmalNo ratings yet
- Laphar AddDocument2 pagesLaphar AddTessa RuliantyNo ratings yet
- Cardiovascular Physical Examination - SyifaDocument66 pagesCardiovascular Physical Examination - SyifaSyifa Mahmud Syukran AkbarNo ratings yet
- Cardiomegaly in CatsDocument2 pagesCardiomegaly in CatspilipNo ratings yet
- Cardiac Science "Arrhythmia"Document16 pagesCardiac Science "Arrhythmia"jimjose antonyNo ratings yet
- MSK W4 Lec 6Document20 pagesMSK W4 Lec 6sharon christieNo ratings yet
- Arterioscler Scopiea: Microscopically, MacrophagesDocument1 pageArterioscler Scopiea: Microscopically, MacrophagesFghu GhujiNo ratings yet
- HypertensionDocument1 pageHypertensionTar digrateNo ratings yet
- Hemodialysis Vascular Access Morbidity1: HaroldDocument13 pagesHemodialysis Vascular Access Morbidity1: Harolderikazoku moNo ratings yet
- Halal Bihalal Obtetri Ginekologi FK UNDIP (Edited 2)Document6 pagesHalal Bihalal Obtetri Ginekologi FK UNDIP (Edited 2)Louis HadiyantoNo ratings yet
- JurnalDocument7 pagesJurnalObgyn Maret 2019No ratings yet
- Maternity Hospital PowerPoint TemplatesDocument48 pagesMaternity Hospital PowerPoint TemplatesweberNo ratings yet
- 0068KJR - KJR 5 39Document8 pages0068KJR - KJR 5 39Louis HadiyantoNo ratings yet
- Asuhan Persalinan NormalDocument18 pagesAsuhan Persalinan NormalLouis HadiyantoNo ratings yet
- Asuhan Persalinan NormalDocument18 pagesAsuhan Persalinan NormalLouis HadiyantoNo ratings yet
- Asuhan Persalinan NormalDocument18 pagesAsuhan Persalinan NormalLouis HadiyantoNo ratings yet
- Cervical Conization Procedure OverviewDocument8 pagesCervical Conization Procedure OverviewLouis HadiyantoNo ratings yet
- Soal Ujian Semester 1Document4 pagesSoal Ujian Semester 1Louis HadiyantoNo ratings yet
- GTG 55Document33 pagesGTG 55Uzairie AnwarNo ratings yet
- HypertensionDocument5 pagesHypertensionLouis HadiyantoNo ratings yet
- Asuhan Persalinan NormalDocument18 pagesAsuhan Persalinan NormalLouis HadiyantoNo ratings yet
- Handout Practical SPSSDocument20 pagesHandout Practical SPSSLouis HadiyantoNo ratings yet
- SOAL-SOAL TEST MASUK OBSGYNDocument3 pagesSOAL-SOAL TEST MASUK OBSGYNLouis HadiyantoNo ratings yet
- Soal 5 ObsDocument9 pagesSoal 5 ObsLouis HadiyantoNo ratings yet
- Soal 8 ObsDocument7 pagesSoal 8 ObsLouis HadiyantoNo ratings yet
- Handout Practical SPSSDocument20 pagesHandout Practical SPSSLouis HadiyantoNo ratings yet
- Soal 7 ObsDocument3 pagesSoal 7 ObsLouis HadiyantoNo ratings yet
- Obs I, 27 Desember 2007 Multiple ChoiceDocument8 pagesObs I, 27 Desember 2007 Multiple ChoiceLouis Hadiyanto100% (1)
- Soal Obs PunyakuDocument1 pageSoal Obs PunyakuFerinaTarizaIINo ratings yet
- Coronary Heart Disease (CHD)Document6 pagesCoronary Heart Disease (CHD)Louis HadiyantoNo ratings yet
- Hemolytic Disease of The Fetus and NewbornDocument24 pagesHemolytic Disease of The Fetus and NewbornLouis HadiyantoNo ratings yet
- Cardiology: Sherif EL Hawary, MDDocument4 pagesCardiology: Sherif EL Hawary, MDMahmoud AbouelsoudNo ratings yet
- Overview of The Evaluation of Stroke - UpToDateDocument57 pagesOverview of The Evaluation of Stroke - UpToDateclarissa suryaNo ratings yet
- Blood Supply of The BrainDocument32 pagesBlood Supply of The BrainShimmering MoonNo ratings yet
- StrokeDocument19 pagesStrokesridhar100% (4)
- Strokeaha 123 042874Document2 pagesStrokeaha 123 042874Shivam TiwariNo ratings yet
- SECTION 6: Spleen: and OverviewDocument38 pagesSECTION 6: Spleen: and Overviewtudoranluciana1No ratings yet
- Ala 3Document30 pagesAla 3Alaz NellyNo ratings yet
- Congenital Heart Diseases (Board Preparation)Document15 pagesCongenital Heart Diseases (Board Preparation)HÉCTOR ULISES AGUILAR ARIASNo ratings yet
- The Heart Activity 3 PDFDocument4 pagesThe Heart Activity 3 PDFbiancaNo ratings yet
- The StomachDocument1 pageThe StomachNicole CabahugNo ratings yet
- Angioplasty and Vascular StentingDocument8 pagesAngioplasty and Vascular Stentingrajnishpathak648No ratings yet
- Understanding Thrombosis: Causes, Types, Prevention & TreatmentDocument11 pagesUnderstanding Thrombosis: Causes, Types, Prevention & TreatmentIrum RafeeqNo ratings yet
- Effect of warm water foot bath therapy on blood pressure reductionDocument8 pagesEffect of warm water foot bath therapy on blood pressure reductionPutraNo ratings yet
- Junetta Cooper Vsim Prep 2Document5 pagesJunetta Cooper Vsim Prep 2Michelle Pinkhasova100% (2)
- Circulatory System QuestionsDocument4 pagesCirculatory System QuestionsJohn Vincent Gonzales50% (2)
- The circulatory system and blood cellsDocument3 pagesThe circulatory system and blood cellsMo GamerNo ratings yet
- The Language of Medicine: Cardiovascular SystemDocument33 pagesThe Language of Medicine: Cardiovascular SystemCPD MASNo ratings yet
- How Long Do Partial Thickness Burns Typically Take To Heal?Document49 pagesHow Long Do Partial Thickness Burns Typically Take To Heal?Farah FarahNo ratings yet
- Interpretation Chest X RayDocument127 pagesInterpretation Chest X RayVimal NishadNo ratings yet
- 02 Integrated Organ Based Course I (Cardiovascular System) Anatomy of The Heart HandoutDocument40 pages02 Integrated Organ Based Course I (Cardiovascular System) Anatomy of The Heart HandoutLan NguyenNo ratings yet
- Coronary Heart Disease: Angina Pectoris: Assistant Professor Department of Internal Medicine #1Document48 pagesCoronary Heart Disease: Angina Pectoris: Assistant Professor Department of Internal Medicine #1nadhirahfauzi100% (1)
- Measuring Blood Pressure with a SphygmomanometerDocument23 pagesMeasuring Blood Pressure with a SphygmomanometerAbdulaziz AHNo ratings yet
- Coronary Artery Bypass Graft Cabg SurgeryDocument26 pagesCoronary Artery Bypass Graft Cabg SurgeryNogra CarlNo ratings yet
- MPAS540 2019 PA Medicine I SyllabusDocument6 pagesMPAS540 2019 PA Medicine I SyllabusSteven CongressNo ratings yet
- Arterial PulsesDocument14 pagesArterial PulsesPrajwal Rao KNo ratings yet
- Intraoperative Management of Shock in Adults - UpToDateDocument36 pagesIntraoperative Management of Shock in Adults - UpToDateYessica RivasNo ratings yet
- Sindromul Coronarian Acut: UMF VB Timisoara Departamentul VI Medicina Interna de AmbulatorDocument78 pagesSindromul Coronarian Acut: UMF VB Timisoara Departamentul VI Medicina Interna de AmbulatorIulia CeveiNo ratings yet
- Plus Plastic Tubes Instructions Venipuncture VS5730Document2 pagesPlus Plastic Tubes Instructions Venipuncture VS5730jawadkhan_5No ratings yet
- Acute Coronary SyndromeDocument9 pagesAcute Coronary Syndromekimchi girlNo ratings yet
- Janeth Cardiovascular ExamDocument10 pagesJaneth Cardiovascular ExammatthewandmaverickjeNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)