You might also like
- Womens Fitness UK 08.2021Document92 pagesWomens Fitness UK 08.2021Diseño ArtisNo ratings yet
- Instant Assessments for Data Tracking, Grade 2: MathFrom EverandInstant Assessments for Data Tracking, Grade 2: MathNo ratings yet
- Sample Questions For HAAD Prometric and DHA For NursesDocument46 pagesSample Questions For HAAD Prometric and DHA For NursesJaezelle Ella Sabale100% (4)
- Chest Physiotherapy ReportDocument8 pagesChest Physiotherapy ReportPatricia G ChiuNo ratings yet
- MCQ PebcDocument7 pagesMCQ Pebcshamram20050% (1)
- 2018 ESMO Handbook of Interpreting Oncological Study PublicationsDocument219 pages2018 ESMO Handbook of Interpreting Oncological Study PublicationsAlex Lugli100% (1)
- SITXWHS004 Assessment 1 - ProjectDocument18 pagesSITXWHS004 Assessment 1 - Projectaarja stha100% (1)
- Modul Dermatovenerologi 2 - DR DeaDocument21 pagesModul Dermatovenerologi 2 - DR DeaDendy AgusNo ratings yet
- Informative Speech OutlineDocument3 pagesInformative Speech Outlineapi-250554127100% (1)
- Iec Obg CareDocument16 pagesIec Obg CareBlessy Madhuri100% (1)
- Guided Home Module: Psychosocial Support Activities For Elementary Learners Cordillera Administrative Region (CAR)Document36 pagesGuided Home Module: Psychosocial Support Activities For Elementary Learners Cordillera Administrative Region (CAR)Jennyhyn cruz75% (4)
- Ortopedie Traumatologie Schite Examen PracticDocument46 pagesOrtopedie Traumatologie Schite Examen PracticMarcela BucicăNo ratings yet
- Arterial Anatomy of The Female Genital Tract - Variations and Relevance To Transcatheter Embolization of The UterusDocument12 pagesArterial Anatomy of The Female Genital Tract - Variations and Relevance To Transcatheter Embolization of The UterusFelipe Wei Ning WangNo ratings yet
- Rheumatic Fever PathophysiologyDocument1 pageRheumatic Fever PathophysiologyAlyssa Mae RadamNo ratings yet
- §Μjf§Μff駥: .Gg#Ffg9Nhhit*..Um=A.WDocument1 page§Μjf§Μff駥: .Gg#Ffg9Nhhit*..Um=A.WNICHAPORN NATTAWUTNo ratings yet
- Cases NotesDocument5 pagesCases NotessofiakeziacabaroNo ratings yet
- Progress NotesDocument3 pagesProgress NotesKISHORE KUMARNo ratings yet
- Cerebrovascular Diseases Harrisons NotesDocument2 pagesCerebrovascular Diseases Harrisons NotesJoanna ValenciaNo ratings yet
- 1 Open House BesokDocument6 pages1 Open House BesokRedigo RahmadhaniNo ratings yet
- Lect13 Weight Bal SlidesDocument4 pagesLect13 Weight Bal Slidesrashed44No ratings yet
- Pathophysiology: ThinningDocument1 pagePathophysiology: ThinningArwaNo ratings yet
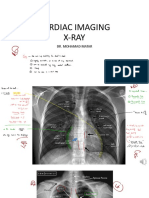
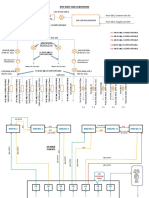
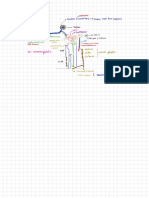
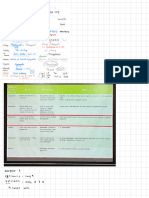
- Cardio 2 - X-RayDocument45 pagesCardio 2 - X-RaySaja SaqerNo ratings yet
- ThalamusDocument4 pagesThalamusi gede ricky jaya purnawarmanNo ratings yet
- Senng - Ch/6Mo) 76Nmlhlmalle8I: MenfalareeDocument5 pagesSenng - Ch/6Mo) 76Nmlhlmalle8I: MenfalareeGachibag IdNo ratings yet
- CH 19 - HeartDocument8 pagesCH 19 - HeartElle QuizonNo ratings yet
- Blood PhysiologyDocument1 pageBlood PhysiologyAnshu SharmaNo ratings yet
- EndocrineDocument19 pagesEndocrineIsabel Bibat DavidNo ratings yet
- KPD West Side SubstationDocument2 pagesKPD West Side SubstationDigraj SinghNo ratings yet
- Digestive (DONE)Document1 pageDigestive (DONE)Aoun Sial60No ratings yet
- Types of Muscles and Their MovementsDocument2 pagesTypes of Muscles and Their Movementsfunny video all indiaNo ratings yet
- Simple: EntersDocument4 pagesSimple: EntersScienceStudsNo ratings yet
- Immunoglobulin: GlanglionDocument1 pageImmunoglobulin: Glanglionธีรนัย เสารางทอยNo ratings yet
- PHA 618: Human Physiology and Pathophysiology Cardiovascular ExercisesDocument2 pagesPHA 618: Human Physiology and Pathophysiology Cardiovascular Exerciseskaila lunaNo ratings yet
- DahoDocument29 pagesDahofodiy49587No ratings yet
- CNS Tumor Map 2020 FullDocument1 pageCNS Tumor Map 2020 FullAlves de MeloNo ratings yet
- Im NotesDocument1 pageIm NotesNicole GayetaNo ratings yet
- Forensic MedicineDocument60 pagesForensic MedicineKoushal Sharma, JammuNo ratings yet
- Centos: NamenDocument1 pageCentos: NamenMr. ACDCNo ratings yet
- 095 Neurology Physiology Descending Tracts Corticospinal TractDocument1 page095 Neurology Physiology Descending Tracts Corticospinal TractxcqzprnfkrNo ratings yet
- Proliferation Lymphatic: Leading ?Document6 pagesProliferation Lymphatic: Leading ?flzhathrhNo ratings yet
- ETAP Direct2D PrintingDocument1 pageETAP Direct2D PrintingDarshit VyasNo ratings yet
- OSLD With Time GradingDocument1 pageOSLD With Time GradingDarshit VyasNo ratings yet
- Fortalecimento de Relações Entre Brasil e EUADocument1 pageFortalecimento de Relações Entre Brasil e EUAAna LetíciaNo ratings yet
- Digestion - 6Document11 pagesDigestion - 6aaravrshah14No ratings yet
- Patho 1aDocument3 pagesPatho 1aaaaalliah2No ratings yet
- 19.R. Pancreas - Cai BiliareDocument10 pages19.R. Pancreas - Cai BiliareAna MîndrilăNo ratings yet
- Neurology Physiology 25 Spinal Cord Ascending Tracts SpinothalamicDocument1 pageNeurology Physiology 25 Spinal Cord Ascending Tracts SpinothalamicxcqzprnfkrNo ratings yet
- Tugas 7 - Pik - Pefd Pabrik Nitrobenzena - Yohanes Nico Prabowo - Kelas A - 8Document1 pageTugas 7 - Pik - Pefd Pabrik Nitrobenzena - Yohanes Nico Prabowo - Kelas A - 8Nico MarpaungNo ratings yet
- Wcm46!38!39 Business HRDocument1 pageWcm46!38!39 Business HRSonja AndelkovicNo ratings yet
- Routes of Administration PDFDocument1 pageRoutes of Administration PDFnazbeen.ahmadiNo ratings yet
- Burns PathophysiologyDocument1 pageBurns PathophysiologyChiara FajardoNo ratings yet
- PathologyDocument64 pagesPathology2021004207.garimaNo ratings yet
- Ndumndum Ps SDPDocument1 pageNdumndum Ps SDPKaka KuxNo ratings yet
- 7.01 ClosingDocument1 page7.01 ClosingSyaza SyedNo ratings yet
- Chapter 4Document1 pageChapter 4Shaurya JainNo ratings yet
- Lek 16 104265 PX 2365 00214 0001 1aDocument1 pageLek 16 104265 PX 2365 00214 0001 1aAhsan Nawax GoGoNo ratings yet
- ARRYTHMIASDocument3 pagesARRYTHMIASitstheboyjayyNo ratings yet
- Head and NeckDocument291 pagesHead and NeckBabatundeNo ratings yet
- HypertensionDocument1 pageHypertensionvictor.garcia4080No ratings yet
- Lewy Body Dementias Dementia With Lewy Bodies And.9Document29 pagesLewy Body Dementias Dementia With Lewy Bodies And.9Cristina GhizdavetNo ratings yet
- 3 PDFDocument1 page3 PDFSim Pei YingNo ratings yet
- BSP1702 NotesDocument7 pagesBSP1702 NotesliyangwongNo ratings yet
- Biology Matters 3rd EditionDocument272 pagesBiology Matters 3rd Editionotakukat763No ratings yet
- Mind Maps MD: (© 2020 American Academy of Ophthalmology)Document1 pageMind Maps MD: (© 2020 American Academy of Ophthalmology)Mido KimoNo ratings yet
- FiebreDocument1 pageFiebreJENNIFER DIANA MORENO PRECIADONo ratings yet
- It Impact Zone: Technical Security: Featured Technology SolutionsDocument5 pagesIt Impact Zone: Technical Security: Featured Technology SolutionsSapaNo ratings yet
- ANS DrugsDocument9 pagesANS DrugsHarly E. DeniegaNo ratings yet
- Timeline: Kristabella Gianina1, Jenivia Thiono1, Erwinsyah Harahap2, Shinta V Hutajulu3Document1 pageTimeline: Kristabella Gianina1, Jenivia Thiono1, Erwinsyah Harahap2, Shinta V Hutajulu3Kristabella GianinaNo ratings yet
- La Casa de La CalidadDocument8 pagesLa Casa de La CalidadEdison EscalanteNo ratings yet
- A. Classification and Characteristics of Diabetes MellitusDocument6 pagesA. Classification and Characteristics of Diabetes MellitusNicole Villanueva, BSN - Level 3ANo ratings yet
- Seminar: Sameer Jauhar, Mandy Johnstone, Peter J MckennaDocument14 pagesSeminar: Sameer Jauhar, Mandy Johnstone, Peter J MckennaMagdalena Zepeda MarambioNo ratings yet
- Gynae Training ManualDocument30 pagesGynae Training ManualKhushi Husna100% (1)
- Drug Formulary HospitalDocument98 pagesDrug Formulary HospitalahmshmNo ratings yet
- f2 Home-Sci Simplified Notes SPDocument20 pagesf2 Home-Sci Simplified Notes SPmicah isabokeNo ratings yet
- Cultural Perspectives in ChildbearingDocument4 pagesCultural Perspectives in ChildbearingdulceRNNo ratings yet
- Brad Blanton - Radical HonestyDocument10 pagesBrad Blanton - Radical HonestyraduNo ratings yet
- Behcet DiseaseDocument6 pagesBehcet DiseasejbahalkehNo ratings yet
- Product Brochure 2023-2024 en LRDocument23 pagesProduct Brochure 2023-2024 en LRaf8009035No ratings yet
- Voice Therapy Does Science Support The ArtDocument5 pagesVoice Therapy Does Science Support The ArtYurleidys ZapaNo ratings yet
- Module 7 Lesson 4Document31 pagesModule 7 Lesson 4MA EDYLYN NOGUERRANo ratings yet
- 1 TTP Mozambique - STE EIS Vol - I - Submitted - For - Disclosure - 0Document227 pages1 TTP Mozambique - STE EIS Vol - I - Submitted - For - Disclosure - 0Luciana MirandaNo ratings yet
- Student Copy Conti - Intrapartal Week8Document25 pagesStudent Copy Conti - Intrapartal Week8Toyour EternityNo ratings yet
- Use of Alcohol Containing Caps ForDocument6 pagesUse of Alcohol Containing Caps ForGaby FernandezNo ratings yet
- Ethical Considerations in Transcultural Nursing.Document1 pageEthical Considerations in Transcultural Nursing.Maddy LaraNo ratings yet
- Brucellosis - DR Esayas Kebede GudinaDocument44 pagesBrucellosis - DR Esayas Kebede GudinaEsayas KebedeNo ratings yet
- Pharmacy As A Profession Rev1Document34 pagesPharmacy As A Profession Rev1Gloria dela CruzNo ratings yet
- A Last Resort?Document942 pagesA Last Resort?SBS_NewsNo ratings yet
- Evolution of Spaces With Respect To Child PsychologyDocument28 pagesEvolution of Spaces With Respect To Child PsychologyDevvrat ChowdharyNo ratings yet
- 3390 3396 PDFDocument7 pages3390 3396 PDFXavier Alexandro Ríos SalinasNo ratings yet
- Suchita Srivastava & Anr Vs Chandigarh Administration On 28 August 2009Document11 pagesSuchita Srivastava & Anr Vs Chandigarh Administration On 28 August 2009Disability Rights AllianceNo ratings yet