You might also like
- Renal Failure in Burn :: الفشل الكلوي لدى مرضى الحروقDocument36 pagesRenal Failure in Burn :: الفشل الكلوي لدى مرضى الحروقDr Mohamed A. El Rouby100% (2)
- Acute RF in ICU (PICUCOURSE)Document45 pagesAcute RF in ICU (PICUCOURSE)surasuarezlopezNo ratings yet
- Topic 32 - Acute Renal FailureDocument4 pagesTopic 32 - Acute Renal FailureAelita RuseelNo ratings yet
- Altered Elimination Multi System ProblemDocument9 pagesAltered Elimination Multi System ProblemCG Patron BamboNo ratings yet
- Acute Renal FailureDocument30 pagesAcute Renal FailureCarmina SalvañaNo ratings yet
- Chapter 1: Introduction To Urinalysis: Urine CompositionDocument74 pagesChapter 1: Introduction To Urinalysis: Urine CompositionMegumi TadokoroNo ratings yet
- Pathophys UrinaryDocument31 pagesPathophys UrinaryDr Anais AsimNo ratings yet
- Clinical Chemistry Renal FunctionDocument20 pagesClinical Chemistry Renal FunctionNida RidzuanNo ratings yet
- Renal FunctionDocument20 pagesRenal FunctionBatrisyia BalqisNo ratings yet
- Acute Renal FailureDocument6 pagesAcute Renal FailureFrancine Kyle SusanoNo ratings yet
- Potassium Disorders: Syeda Shaheera ZaidiDocument60 pagesPotassium Disorders: Syeda Shaheera ZaidiMohammad AliNo ratings yet
- LECTURE Renal DisordersDocument21 pagesLECTURE Renal DisordersAnnie Rose Dorothy MamingNo ratings yet
- Altered Elimination LecDocument7 pagesAltered Elimination LecJean Rynne Barrameda BongaisNo ratings yet
- CC Lec Mod 3Document13 pagesCC Lec Mod 38wgmhh9ks9No ratings yet
- General Characteristics: Acute Kidney InjuryDocument8 pagesGeneral Characteristics: Acute Kidney InjurykhaledNo ratings yet
- Aki NotesDocument10 pagesAki NotesGennel Mae GarovilloNo ratings yet
- Topic 6 Renal Failure - UpdatedDocument12 pagesTopic 6 Renal Failure - Updatedezinne obinna-umaNo ratings yet
- Renal Acute Kidney InjuryDocument41 pagesRenal Acute Kidney InjuryTim SilvaNo ratings yet
- Acute Kidney InjuryDocument32 pagesAcute Kidney InjuryPremKumar ShamugamNo ratings yet
- Urinary System Diseases: PathophysiologyDocument31 pagesUrinary System Diseases: Pathophysiologyai nisa hasnasariNo ratings yet
- Clin Micro - Introduction and UrinalysisDocument2 pagesClin Micro - Introduction and UrinalysisbiancsNo ratings yet
- CCRNPart 2Document164 pagesCCRNPart 2Paolo Vega100% (5)
- CC2 PREMILS To FINALS MERGED PDFDocument65 pagesCC2 PREMILS To FINALS MERGED PDFAlecx LipatanNo ratings yet
- Acute Renal Failure: Dr. Rebecca JacobDocument6 pagesAcute Renal Failure: Dr. Rebecca JacobRevalitha PutriNo ratings yet
- Urinary System Diseases: PathophysiologyDocument31 pagesUrinary System Diseases: PathophysiologyMuhammad Wishal KhanNo ratings yet
- Acute Kidney Injury (AKI) : by Prof Grace Irimu Consultant Pediatrician and NephrologistDocument43 pagesAcute Kidney Injury (AKI) : by Prof Grace Irimu Consultant Pediatrician and Nephrologistokwadha simionNo ratings yet
- MS - Fluids and ElectrolytesDocument6 pagesMS - Fluids and ElectrolytesJOHN LOYD CASTILLONo ratings yet
- Acute Kidney Injury: Syakib BakriDocument46 pagesAcute Kidney Injury: Syakib BakriBhisma D. SyaputraNo ratings yet
- Better Indicator of Renal Disease 2. Less Affected by Diet 3. Depends Upon Muscle Mass (E.g. Low in Infants and Elderly Small Women)Document2 pagesBetter Indicator of Renal Disease 2. Less Affected by Diet 3. Depends Upon Muscle Mass (E.g. Low in Infants and Elderly Small Women)ahsanNo ratings yet
- Dr. Vineet ChaturvediDocument69 pagesDr. Vineet ChaturvediVinay PatilNo ratings yet
- Renal FailureDocument27 pagesRenal FailureMae DacerNo ratings yet
- Chronic Renal Failure: PathophysiologyDocument1 pageChronic Renal Failure: PathophysiologyCindy Mae Dela Torre100% (2)
- Drugs Therapy For Kidney: Budi RaharjoDocument33 pagesDrugs Therapy For Kidney: Budi RaharjoNurul MasyithahNo ratings yet
- Renal FailureDocument61 pagesRenal FailureEdward XiamNo ratings yet
- Kidney Function and DiseasesDocument70 pagesKidney Function and DiseasesGovind SharmaNo ratings yet
- Chronic Renal Failure 2Document66 pagesChronic Renal Failure 2Octaviani ElparesiNo ratings yet
- Renal Function TestsDocument23 pagesRenal Function TestsKer YehunNo ratings yet
- Anatomi Dan Fisiologi GinjalDocument6 pagesAnatomi Dan Fisiologi GinjalAndy F MonroeNo ratings yet
- 12a. Kuliah Aki 2017Document36 pages12a. Kuliah Aki 2017yussikafernandaNo ratings yet
- HY RenalDocument50 pagesHY RenalJeniNo ratings yet
- 3 AntihypertensiveDocument33 pages3 AntihypertensiveJericho De GuzmanNo ratings yet
- Fisiologi DiuresisDocument26 pagesFisiologi DiuresisYuliasminde SofyanaNo ratings yet
- Nephrology DR ZeinabDocument101 pagesNephrology DR ZeinabZeinab Muhammad100% (1)
- A. B. C. A. B. C. D.: Clinical Chemistry II - Prelims (Bandala)Document19 pagesA. B. C. A. B. C. D.: Clinical Chemistry II - Prelims (Bandala)IceNo ratings yet
- The Physiology of The Urine Production (2021)Document80 pagesThe Physiology of The Urine Production (2021)Shelly NobelNo ratings yet
- Acute Renal Failure Lecture 1 Critical Care NursingDocument52 pagesAcute Renal Failure Lecture 1 Critical Care NursingDina Rasmita100% (2)
- Presentation I PC II RENALDocument58 pagesPresentation I PC II RENALSuhayb CumarNo ratings yet
- Genitourinary System: Billy Ray A. Marcelo, RNDocument35 pagesGenitourinary System: Billy Ray A. Marcelo, RNDarell M. BookNo ratings yet
- 2long Term Regulation of Blood PressureDocument21 pages2long Term Regulation of Blood PressureamrendraNo ratings yet
- By: Yzobelle RedondoDocument4 pagesBy: Yzobelle RedondoArabelle GONo ratings yet
- General Principles of Tubular ReabsorptionDocument54 pagesGeneral Principles of Tubular ReabsorptionRalph JacintoNo ratings yet
- Kidney AG-1Document170 pagesKidney AG-1aleenashibu993No ratings yet
- Renal Urinary Assessment2Document13 pagesRenal Urinary Assessment2Ana GonzalezNo ratings yet
- AKI, CKD SummaryDocument4 pagesAKI, CKD SummaryMuathNo ratings yet
- HY RenalDocument50 pagesHY RenalA R HasanNo ratings yet
- Genitourinary System: Renal FailureDocument6 pagesGenitourinary System: Renal FailureEn ConejosNo ratings yet
- Mechanism of Urine Production. Urine Composition in Health and Pathologies. Biochemistry of Water and Salts TurnoverDocument73 pagesMechanism of Urine Production. Urine Composition in Health and Pathologies. Biochemistry of Water and Salts TurnoverRAJA RAJANNo ratings yet
- Acute Kidney InjuryDocument62 pagesAcute Kidney InjuryApidha KartinasariNo ratings yet
- Renal FailureDocument11 pagesRenal FailureLindsey MeimbanNo ratings yet
- Urinary Stones: Medical and Surgical ManagementFrom EverandUrinary Stones: Medical and Surgical ManagementMichael GrassoNo ratings yet
- Developmental Milestones 1Document2 pagesDevelopmental Milestones 1HazelGraceNo ratings yet
- Developmental Milestones 2Document3 pagesDevelopmental Milestones 2HazelGraceNo ratings yet
- Mother and Neonatal ChangesDocument2 pagesMother and Neonatal ChangesHazelGraceNo ratings yet
- Fetal DevelopmentDocument5 pagesFetal DevelopmentHazelGraceNo ratings yet
- Labor and DeliveryDocument6 pagesLabor and DeliveryHazelGraceNo ratings yet
- Postpartum CareDocument4 pagesPostpartum CareHazelGraceNo ratings yet
- The Sequence of Events That Occur in The Heart During Cardiac CycleDocument13 pagesThe Sequence of Events That Occur in The Heart During Cardiac CycleADITYAROOP PATHAKNo ratings yet
- Human Physiology LecturesDocument171 pagesHuman Physiology LecturesPhysiology by Dr Raghuveer57% (7)
- Clinical Pharmacology Made Ridiculously Simple MedicalstudyzoneDocument190 pagesClinical Pharmacology Made Ridiculously Simple MedicalstudyzoneVenniilaaSaravananNo ratings yet
- Renal EmergenciesDocument93 pagesRenal EmergenciesShubham gaurNo ratings yet
- Chapter No. 15 - Homeostasis (By Faisal Zada Khan)Document36 pagesChapter No. 15 - Homeostasis (By Faisal Zada Khan)Pubg Killer15No ratings yet
- Geriatric RehabilitationDocument16 pagesGeriatric RehabilitationAjay DherwaniNo ratings yet
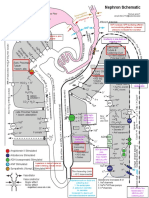
- NephronMap Copy2Document1 pageNephronMap Copy2Anonymous KxwaMDhANo ratings yet
- QP Code: 1075: Rajiv Gandhi University of Health Sciences, KarnatakaDocument5 pagesQP Code: 1075: Rajiv Gandhi University of Health Sciences, KarnatakaDyan Dixith DcNo ratings yet
- Drugs That Affect The Urinary System: PharmacologyDocument96 pagesDrugs That Affect The Urinary System: PharmacologyKameh Dani Adrian Wadzon'sNo ratings yet
- Zoology II (Em) BLM 21-22Document99 pagesZoology II (Em) BLM 21-22GANESH KANDAGATLANo ratings yet
- Case of Fluid and Electrolyte Balance & Acid BaseDocument7 pagesCase of Fluid and Electrolyte Balance & Acid BaseVia ArianiNo ratings yet
- A Note Pre MedDocument24 pagesA Note Pre Medwan amiera wan malekNo ratings yet
- Nursing Q and A (Volume 2)Document7 pagesNursing Q and A (Volume 2)Rem Yriz100% (1)
- AQA-synoptic Essay Marking GuidelinesDocument13 pagesAQA-synoptic Essay Marking GuidelinesSarah HarleyNo ratings yet
- PSL301 Midterm 2 ReviewDocument24 pagesPSL301 Midterm 2 Reviewtapi0ca100% (1)
- Gomerged Document 7Document576 pagesGomerged Document 7bizzarobmNo ratings yet
- AUBF Reinforcement ExamDocument67 pagesAUBF Reinforcement ExamVanessa May BlancioNo ratings yet
- Bahasa Inggris 1.13Document5 pagesBahasa Inggris 1.13Rizky AdiNo ratings yet
- IVMS-Gross Pathology, Histopathology, Microbiology and Radiography High Yield Image PlatesDocument151 pagesIVMS-Gross Pathology, Histopathology, Microbiology and Radiography High Yield Image PlatesMarc Imhotep Cray, M.D.100% (2)
- Print PDFDocument16 pagesPrint PDFRobert ChristevenNo ratings yet
- Chemical Examination of UrineDocument17 pagesChemical Examination of Urinekaran kambojNo ratings yet
- 2 Tietz 2012 Kidney Function TestsDocument39 pages2 Tietz 2012 Kidney Function TestsIvana BajunovicNo ratings yet
- Nursing Practice IvDocument38 pagesNursing Practice IvJohn wewNo ratings yet
- Pharma 1,2Document10 pagesPharma 1,2Ahmed KafajiNo ratings yet
- Medical School Renal ReviewDocument32 pagesMedical School Renal ReviewwmtxbbNo ratings yet
- Medical Electronics Unit 3Document64 pagesMedical Electronics Unit 3TamilselvanNo ratings yet
- Acute Renal FailureDocument59 pagesAcute Renal Failurepaul_v_44440% (1)
- ESRD Case Analysis - Group 4Document34 pagesESRD Case Analysis - Group 4Sean Jeffrey J. FentressNo ratings yet
- Soal Kidney CompiledDocument28 pagesSoal Kidney Compiledstella pangestika100% (1)
- % Chapter 1: Regulation of Water ContentDocument39 pages% Chapter 1: Regulation of Water ContentK CNo ratings yet