You might also like
- Mental DisorderDocument5 pagesMental DisorderHijaz TurohaNo ratings yet
- PNES ClinicalApproachesDocument19 pagesPNES ClinicalApproachesClaudiaNo ratings yet
- ZiffyHealth Pitch DeckDocument32 pagesZiffyHealth Pitch DeckSanjay Kumar100% (1)
- What Is Your Road, Man?Document232 pagesWhat Is Your Road, Man?Oana AndreeaNo ratings yet
- 2023 Catalog Score SummerDocument65 pages2023 Catalog Score Summermadhudasa0% (2)
- Schizophrenia: Psychiatric DisordersDocument33 pagesSchizophrenia: Psychiatric DisordersNdoo NdooNo ratings yet
- MINTZBERGDocument32 pagesMINTZBERGgeezee10004464100% (2)
- Van Os J, Kapur S. Schizophrenia - Lancet 2009 374 635-45 PDFDocument11 pagesVan Os J, Kapur S. Schizophrenia - Lancet 2009 374 635-45 PDFVictorVeroneseNo ratings yet
- Construction Materials and Testing: "WOOD"Document31 pagesConstruction Materials and Testing: "WOOD"Aira Joy AnyayahanNo ratings yet
- 2 Integrated MarketingDocument13 pages2 Integrated MarketingPaula Marin CrespoNo ratings yet
- Review Article: Parkinson's Disease and Cognitive ImpairmentDocument8 pagesReview Article: Parkinson's Disease and Cognitive ImpairmentValentina CiciliaNo ratings yet
- WJP 12 1127Document15 pagesWJP 12 1127C ONo ratings yet
- Management of Psychosis in Parkinson’s DiseaseDocument18 pagesManagement of Psychosis in Parkinson’s DiseaseloloasbNo ratings yet
- Psychiatric Disorders Drug Discovery OverviewDocument10 pagesPsychiatric Disorders Drug Discovery OverviewCarlos Cesar Lopez SuarezNo ratings yet
- Current Treatment of Behavioral and Cognitive Symptoms of Parkinson's DiseaseDocument9 pagesCurrent Treatment of Behavioral and Cognitive Symptoms of Parkinson's DiseasePriska AmeliaNo ratings yet
- Diagnosing and Treating Late-Life PsychosisDocument13 pagesDiagnosing and Treating Late-Life PsychosisNatalia MenottiNo ratings yet
- 1545 FullDocument8 pages1545 FullMuhammad Firman Syarif Al-AsyiNo ratings yet
- 186-Book Chapter-902-2-10-20210323Document24 pages186-Book Chapter-902-2-10-20210323Yelaena AbrauNo ratings yet
- The Neuropsychiatry of Parkinson Disease: A Perfect Storm: SciencedirectDocument21 pagesThe Neuropsychiatry of Parkinson Disease: A Perfect Storm: SciencedirectroxanaNo ratings yet
- Secondary Research Paper - Psychopathology of Parkinson's DiseaseDocument7 pagesSecondary Research Paper - Psychopathology of Parkinson's DiseaseKeyur SharmaNo ratings yet
- AbstractDocument2 pagesAbstractapi-251117545No ratings yet
- Treatment of Psychosis and Dementia in Parkinson 'S Disease: Jennifer G. Goldman, MD, MS Samantha Holden, MDDocument18 pagesTreatment of Psychosis and Dementia in Parkinson 'S Disease: Jennifer G. Goldman, MD, MS Samantha Holden, MDNanda apriliantoNo ratings yet
- Agitation in DementiaDocument9 pagesAgitation in DementiasellaNo ratings yet
- CN 18 277Document11 pagesCN 18 277Fernanda NascimentoNo ratings yet
- Article4 2 CR7Document7 pagesArticle4 2 CR7Anonymous uVrbl31EGONo ratings yet
- Psychiatric aspects of Parkinson's diseaseDocument12 pagesPsychiatric aspects of Parkinson's diseaseEdu SajquimNo ratings yet
- Farmacologia de Los Medicamentos Antipsicoticos en AmDocument9 pagesFarmacologia de Los Medicamentos Antipsicoticos en AmedgarmoncadaNo ratings yet
- Affective Symptoms in SchizophreniaDocument7 pagesAffective Symptoms in SchizophreniaanoodiNo ratings yet
- BDDKPDocument21 pagesBDDKPChidube UkachukwuNo ratings yet
- Schizophrenia For Primary Care Providers PDFDocument8 pagesSchizophrenia For Primary Care Providers PDFmerianaNo ratings yet
- PdhallucinationsDocument10 pagesPdhallucinationslauraalvisNo ratings yet
- Ijms 22 09309Document22 pagesIjms 22 09309John SmithNo ratings yet
- LATE ONSET PSYCHOSIS – A CASE REPORTDocument5 pagesLATE ONSET PSYCHOSIS – A CASE REPORTJAVED ATHER SIDDIQUINo ratings yet
- Schizophrenia - Practice Essentials, Background, PathophysiologyDocument10 pagesSchizophrenia - Practice Essentials, Background, PathophysiologydilaNo ratings yet
- The Development of Treatment For Parkinson's Disease: Harishankar Prasad Yadav, Yun LiDocument20 pagesThe Development of Treatment For Parkinson's Disease: Harishankar Prasad Yadav, Yun LiTherezia Sonia Gabriella TanggulunganNo ratings yet
- 66ostachowska Archives PP 4-2015Document11 pages66ostachowska Archives PP 4-2015Eva ElsiNo ratings yet
- Cognitive Impairment and Dementia in Parkinson's Disease - Clinical Features, Diagnosis, and ManagementDocument15 pagesCognitive Impairment and Dementia in Parkinson's Disease - Clinical Features, Diagnosis, and ManagementSebastián GallegosNo ratings yet
- Journal of Sleep DisorderDocument7 pagesJournal of Sleep DisorderSiska TeurupunNo ratings yet
- Rupal Arora - Diagnostic Criteria For Neuropychological DisordersDocument21 pagesRupal Arora - Diagnostic Criteria For Neuropychological Disordersrupal aroraNo ratings yet
- Running Head: PARKINSON'S DISEASE 1Document19 pagesRunning Head: PARKINSON'S DISEASE 1haxxxessNo ratings yet
- Parkinson's Disease Symptoms, Causes, Diagnosis and TreatmentDocument22 pagesParkinson's Disease Symptoms, Causes, Diagnosis and Treatmentindry fitriNo ratings yet
- Sleep Disorders in Parkinson’s Disease: Management and Case StudyFrom EverandSleep Disorders in Parkinson’s Disease: Management and Case StudyChun-Feng LiuNo ratings yet
- Epidemiological and Clinical Characterization Following A First Psychotic Episode in Major Depressive Disorder OWOEYE2013Document10 pagesEpidemiological and Clinical Characterization Following A First Psychotic Episode in Major Depressive Disorder OWOEYE2013Tímea OrszághNo ratings yet
- Impulse Control Disorders in Parkinson's Disease: Crossroads Between Neurology, Psychiatry and NeuroscienceDocument11 pagesImpulse Control Disorders in Parkinson's Disease: Crossroads Between Neurology, Psychiatry and NeuroscienceCarmen CiursaşNo ratings yet
- ATPDDocument11 pagesATPDsagar189No ratings yet
- Anxiety and Mood Disorders in Narcolepsy: A Case - Control StudyDocument8 pagesAnxiety and Mood Disorders in Narcolepsy: A Case - Control StudyDesyifa Annisa MursalinNo ratings yet
- Fahr's Disease and Psychiatric Syndromes - A Case SeriesDocument3 pagesFahr's Disease and Psychiatric Syndromes - A Case SeriesubuntumicNo ratings yet
- Parkinson's Disease: EpidemiologyDocument6 pagesParkinson's Disease: EpidemiologyCarlos MichasNo ratings yet
- Schizoaffective Disorder: Continuing Education ActivityDocument10 pagesSchizoaffective Disorder: Continuing Education ActivitymusdalifahNo ratings yet
- Parkinson's Disease: From Bench To BedsideDocument17 pagesParkinson's Disease: From Bench To BedsideSoap 2221No ratings yet
- Trabajo Grupal Del Articulo - S03 - TMDocument5 pagesTrabajo Grupal Del Articulo - S03 - TMClendy Yudith Rimapa GuerreroNo ratings yet
- Kak Mila 3Document25 pagesKak Mila 3Miftahul UlumNo ratings yet
- Insight and Symptom Severity in An Inpatient Psychiatric SampleDocument12 pagesInsight and Symptom Severity in An Inpatient Psychiatric SamplealejandraNo ratings yet
- Schizophrenia Genetic Mutations RiskDocument9 pagesSchizophrenia Genetic Mutations RiskMasyithah TetaNo ratings yet
- Nonmotor Disturbances in Parkinson's Disease: DiseasesDocument14 pagesNonmotor Disturbances in Parkinson's Disease: DiseasesMaria RamosNo ratings yet
- Course of Psychiatric Symptoms and GlobalDocument8 pagesCourse of Psychiatric Symptoms and GloballoloasbNo ratings yet
- Abnormal PsychologyDocument20 pagesAbnormal PsychologyvinodininadhaNo ratings yet
- Cabas GulayDocument44 pagesCabas GulayJamaicah CabasNo ratings yet
- Parkinson's Depression Onset Tied to Dementia RiskDocument5 pagesParkinson's Depression Onset Tied to Dementia RiskdaliaNo ratings yet
- Ventilator Vol 1 No 3 September 2023 Hal 66-78Document13 pagesVentilator Vol 1 No 3 September 2023 Hal 66-78nelyanthi2021No ratings yet
- Journal of Depression in ParkinsonDocument5 pagesJournal of Depression in ParkinsondaliaNo ratings yet
- Depresi Pada LansiaDocument8 pagesDepresi Pada LansiasasadaraNo ratings yet
- A Guide To The Management of Psychotic Disorders and Neuropsychiatricsymptoms of Dementia in Older AdultsDocument9 pagesA Guide To The Management of Psychotic Disorders and Neuropsychiatricsymptoms of Dementia in Older AdultsPablo RamirezNo ratings yet
- Delusional Disorder - UpToDateDocument21 pagesDelusional Disorder - UpToDateEric GabroNo ratings yet
- Fast Facts: Psychosis in Parkinson's Disease: Finding the right therapeutic balanceFrom EverandFast Facts: Psychosis in Parkinson's Disease: Finding the right therapeutic balanceNo ratings yet
- Finding Clarity: Empowering Patients and Families Facing Schizoaffective DisorderFrom EverandFinding Clarity: Empowering Patients and Families Facing Schizoaffective DisorderNo ratings yet
- 10.1177_13524585211031128Document10 pages10.1177_13524585211031128loloasbNo ratings yet
- 1-s2.0-S2772408522006408-mainDocument2 pages1-s2.0-S2772408522006408-mainloloasbNo ratings yet
- ManagementofParkinsonsDisorderPsychosis11Document20 pagesManagementofParkinsonsDisorderPsychosis11loloasbNo ratings yet
- Acute-Alcohol-Withdrawal-CA2074-v8Document35 pagesAcute-Alcohol-Withdrawal-CA2074-v8loloasbNo ratings yet
- ManagementofParkinsonsDisorderPsychosis11Document20 pagesManagementofParkinsonsDisorderPsychosis11loloasbNo ratings yet
- dnb_vol33_Suppl 4_480Document6 pagesdnb_vol33_Suppl 4_480loloasbNo ratings yet
- carta2018Document9 pagescarta2018loloasbNo ratings yet
- TemplateDocument1 pageTemplateNghĩa PhạmNo ratings yet
- Management of Psychiatric and CognitiveDocument21 pagesManagement of Psychiatric and CognitiveloloasbNo ratings yet
- 30214-ArticleText-56620-2-10-202209071 (1)Document15 pages30214-ArticleText-56620-2-10-202209071 (1)loloasbNo ratings yet
- ManagementofParkinsonsDisorderPsychosis11Document20 pagesManagementofParkinsonsDisorderPsychosis11loloasbNo ratings yet
- The Role of SocioculturalDocument24 pagesThe Role of SocioculturalloloasbNo ratings yet
- 30214-ArticleText-56620-2-10-202209071 (1)Document15 pages30214-ArticleText-56620-2-10-202209071 (1)loloasbNo ratings yet
- Update On Binge EatingDocument12 pagesUpdate On Binge EatingloloasbNo ratings yet
- Confirmation Status Early Career ScientistDocument1 pageConfirmation Status Early Career ScientistloloasbNo ratings yet
- Article Bulimia NervosaDocument10 pagesArticle Bulimia Nervosaallkhusairy6tuansiNo ratings yet
- Pharmacological Treatment of ED, Comorbid Mental Health Problems, Malnutrition and Physical Health Consequences (Himmerich Et Al. 2020)Document16 pagesPharmacological Treatment of ED, Comorbid Mental Health Problems, Malnutrition and Physical Health Consequences (Himmerich Et Al. 2020)Agustín AgassoNo ratings yet
- Recent Research AnDocument9 pagesRecent Research AnloloasbNo ratings yet
- Binge Eating Disorder ANNADocument12 pagesBinge Eating Disorder ANNAloloasbNo ratings yet
- Psychotherapy and Medications For Eating Disorders BTDocument23 pagesPsychotherapy and Medications For Eating Disorders BTloloasbNo ratings yet
- Review of The Burden of Eating DisordersmortalityDocument7 pagesReview of The Burden of Eating DisordersmortalityloloasbNo ratings yet
- Psychotropic Medication For Children and Adolescents With EDocument10 pagesPsychotropic Medication For Children and Adolescents With EloloasbNo ratings yet
- Psychotherapy and Medications For Eating Disorders BTDocument23 pagesPsychotherapy and Medications For Eating Disorders BTloloasbNo ratings yet
- An Update On The Prevalence of Eating Disorders in The GeneralDocument14 pagesAn Update On The Prevalence of Eating Disorders in The GeneralTrâm AnhNo ratings yet
- Al-Adawisetal.2013Revision of ICD Status Update On FeedingDocument12 pagesAl-Adawisetal.2013Revision of ICD Status Update On FeedingloloasbNo ratings yet
- A Placebo-Controlled Pilot Study of Adjunctive OlanzapineDocument6 pagesA Placebo-Controlled Pilot Study of Adjunctive OlanzapineloloasbNo ratings yet
- Lancet Psychiatry AnDocument13 pagesLancet Psychiatry AnmicaelabellaNo ratings yet
- Westmoreland 2016Document49 pagesWestmoreland 2016jsoeNo ratings yet
- An Atlas of Genetic Correlations Across Human DiseasesDocument9 pagesAn Atlas of Genetic Correlations Across Human DiseasesloloasbNo ratings yet
- Unit 1Document50 pagesUnit 1vaniphd3No ratings yet
- Adms OneAdms One ClassDocument9 pagesAdms OneAdms One ClasssafwatNo ratings yet
- Crashing Pert Networks: A Simulation ApproachDocument15 pagesCrashing Pert Networks: A Simulation ApproachRavindra BharathiNo ratings yet
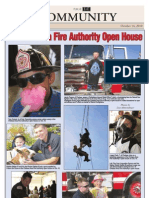
- CAFA Open House HighlightsDocument1 pageCAFA Open House HighlightsDaniel LaiNo ratings yet
- Cyrustek ES51966 (Appa 505)Document25 pagesCyrustek ES51966 (Appa 505)budi0251No ratings yet
- Radio Codes and ConventionsDocument2 pagesRadio Codes and Conventionsapi-570661298No ratings yet
- NST 021 Orientation SASDocument5 pagesNST 021 Orientation SASLady Mae AguilarNo ratings yet
- Lecture Euler EquationDocument33 pagesLecture Euler EquationYash RajNo ratings yet
- Phy Worksheet IG 3 Phase 2Document6 pagesPhy Worksheet IG 3 Phase 2Umair RazaNo ratings yet
- M.Sc. Agriculture (Agronomy)Document23 pagesM.Sc. Agriculture (Agronomy)Abhishek MauryaNo ratings yet
- Training Report On Machine LearningDocument27 pagesTraining Report On Machine LearningBhavesh yadavNo ratings yet
- Basketball 2011: Johnson CountyDocument25 pagesBasketball 2011: Johnson CountyctrnewsNo ratings yet
- CHM131 Presentation - Oxidation of MetalsDocument11 pagesCHM131 Presentation - Oxidation of MetalsNazrul ShahNo ratings yet
- Coffee TestDocument6 pagesCoffee TestAmit Satyen RaviNo ratings yet
- Rg213 Rgflex Coax Braided Cable: Product Data Sheet RG213-50JFDocument1 pageRg213 Rgflex Coax Braided Cable: Product Data Sheet RG213-50JFPancho BerríosNo ratings yet
- Satisfaction ExtraDocument2 pagesSatisfaction ExtraFazir AzlanNo ratings yet
- 2.2valves, Alarm - Ul Product IqDocument1 page2.2valves, Alarm - Ul Product Iqbhima irabattiNo ratings yet
- DOJ OIG Issues 'Fast and Furious' ReportDocument512 pagesDOJ OIG Issues 'Fast and Furious' ReportFoxNewsInsiderNo ratings yet
- Cubic Spline Tutorial v3Document6 pagesCubic Spline Tutorial v3Praveen SrivastavaNo ratings yet
- Chapter 25 (10) Capital Investment Analysis: ObjectivesDocument40 pagesChapter 25 (10) Capital Investment Analysis: ObjectivesJames BarzoNo ratings yet
- 3343 - C-Data-EPON-OLT-FD1108S-CLI-User-Manual-V1-3Document82 pages3343 - C-Data-EPON-OLT-FD1108S-CLI-User-Manual-V1-3Roar ZoneNo ratings yet
- Etherpad Text-Based TutorialDocument5 pagesEtherpad Text-Based Tutorialapi-437836861No ratings yet
- St. Anthony College Calapan City Syllabus: Course DescriptionDocument6 pagesSt. Anthony College Calapan City Syllabus: Course DescriptionAce HorladorNo ratings yet
- Ap4955 PDFDocument4 pagesAp4955 PDFGilvan HenriqueNo ratings yet