You might also like
- I Can Make A DifferenceDocument25 pagesI Can Make A DifferenceTiên Cá Tập BơiNo ratings yet
- The Trees of Florida - A Reference and Field Guide - Gil Nelson (1994) PDFDocument296 pagesThe Trees of Florida - A Reference and Field Guide - Gil Nelson (1994) PDFTruco El Martinez100% (1)
- Political Ideologies An Introdudsdsction by Andrew Heywoodklkkl (001-394)Document394 pagesPolitical Ideologies An Introdudsdsction by Andrew Heywoodklkkl (001-394)railibconNo ratings yet
- 1989Document200 pages1989Dallas County R-I Schools100% (2)
- W H Lester's Application To The Guion Miller Roll, Application No. 32363Document41 pagesW H Lester's Application To The Guion Miller Roll, Application No. 32363ksmith_3434100% (2)
- Traveller Elementary Student BookDocument178 pagesTraveller Elementary Student BookBriza Paulina CordovaNo ratings yet
- Kinds of ForestsDocument6 pagesKinds of Forestsamrit singhNo ratings yet
- Geography by Kartick Chandra MondalDocument481 pagesGeography by Kartick Chandra MondalUjjwal NandiNo ratings yet
- 1917 The Ideal Bartender by Tom Bullock 1Document66 pages1917 The Ideal Bartender by Tom Bullock 1Alex YuJiNo ratings yet
- Usborne - Baby - S Book of RhymesDocument37 pagesUsborne - Baby - S Book of Rhymessugest270383815No ratings yet
- Nursing Work PatternsDocument2 pagesNursing Work Patterns송란다No ratings yet
- Getting Started Knitting Socks PDFDocument137 pagesGetting Started Knitting Socks PDFploky00100% (3)
- Green Prison, Pt. 1Document8 pagesGreen Prison, Pt. 1Robert HaiderNo ratings yet
- The Legend of Zelda Breath of The Wild - Creating A Champion PDFDocument433 pagesThe Legend of Zelda Breath of The Wild - Creating A Champion PDFIván García Quirce97% (30)
- CERAMICS - Porciline Catalog Based On Design.Document34 pagesCERAMICS - Porciline Catalog Based On Design.Kazi Abdullah All MamunNo ratings yet
- Top 100 Global Innovators 2022 Report v9 RGB SIN - ACDocument15 pagesTop 100 Global Innovators 2022 Report v9 RGB SIN - ACeduardomoresiNo ratings yet
- Nathaniel LambinoDocument8 pagesNathaniel LambinoMarkrafael LongayNo ratings yet
- Academic Telegram9Document148 pagesAcademic Telegram9harmansodhi0% (1)
- Alvarez Tapia Leibnizt - Fascilla de Schmidt-FallasDocument5 pagesAlvarez Tapia Leibnizt - Fascilla de Schmidt-Fallasjhossep David Curtihunaca LimaNo ratings yet
- I Irving DavidsonDocument127 pagesI Irving DavidsonAlan Jules Weberman100% (1)
- Akai GX-77 Stereo Reel To Reel Tape Recorder Service Manual + Schematics PDFDocument68 pagesAkai GX-77 Stereo Reel To Reel Tape Recorder Service Manual + Schematics PDFErwinNo ratings yet
- Adobe Scan 11 Dec 2023Document1 pageAdobe Scan 11 Dec 2023Kuldeep PindariaNo ratings yet
- Kostya Kimlat - The Joker Game Lecture Notes 2000 PDFDocument32 pagesKostya Kimlat - The Joker Game Lecture Notes 2000 PDFJohn100% (1)
- Sac AssignmentDocument9 pagesSac AssignmentMansaNo ratings yet
- Best DevOps Consulting Services - IAMOPSDocument8 pagesBest DevOps Consulting Services - IAMOPSIAMOPSNo ratings yet
- Scan 16 May 2022Document2 pagesScan 16 May 2022Aarav AroraNo ratings yet
- Optimum TariffDocument3 pagesOptimum TariffOngfaNo ratings yet
- Scan 5Document1 pageScan 5elefantul2005No ratings yet
- 1952 07 7273984 Tremonton Utah 1377 PDFDocument3 pages1952 07 7273984 Tremonton Utah 1377 PDFzalmezeydNo ratings yet
- Uncl - Assifjeu: R.T TyDocument15 pagesUncl - Assifjeu: R.T TyJohn the PirateNo ratings yet
- 456° Bombing Group Combat MissionDocument276 pages456° Bombing Group Combat MissionFrancescoNo ratings yet
- Casting Question and SolutionsDocument2 pagesCasting Question and SolutionsSriharsha SarmaNo ratings yet
- Final Compil City D&D 3.5Document15 pagesFinal Compil City D&D 3.5Etienne L100% (1)
- Analysis RavishankarDocument196 pagesAnalysis RavishankarKavya sriNo ratings yet
- Economics - Project Digital IndiaDocument3 pagesEconomics - Project Digital IndiaAshutosh SharmaNo ratings yet
- John Lubbock-Prehistoric TimesDocument560 pagesJohn Lubbock-Prehistoric Timesmiracpsl8.1No ratings yet
- Etextbook PDF For Personal Nutrition 10th Edition by Marie A BoyleDocument61 pagesEtextbook PDF For Personal Nutrition 10th Edition by Marie A Boylekarla.woodruff22798% (44)
- Card A Pio GeralDocument50 pagesCard A Pio GeralkathelymluanaNo ratings yet
- Prepositions Homework-DanielDocument2 pagesPrepositions Homework-DanielTony NavaNo ratings yet
- HEP Ultra Relativistic Heavy Ion Collisions by Ramona VogtDocument480 pagesHEP Ultra Relativistic Heavy Ion Collisions by Ramona VogtMusa Rahim Khan100% (2)
- Chris DLDocument1 pageChris DLShilpa DuttaNo ratings yet
- Audited Financial Results March 31, 2019 Reliance Jio Infocomm LimitedDocument9 pagesAudited Financial Results March 31, 2019 Reliance Jio Infocomm Limitedaishwarya raikarNo ratings yet
- Work Magazine 008 1889Document16 pagesWork Magazine 008 1889justanothergunnutNo ratings yet
- Kyk Over Al June - 1948 vl2 n7Document60 pagesKyk Over Al June - 1948 vl2 n7Armando Vázquez CarrilloNo ratings yet
- A 8 Histological Slides (Stomach, SI, Kidney, Liver, Pancreas)Document6 pagesA 8 Histological Slides (Stomach, SI, Kidney, Liver, Pancreas)Aditi MishraNo ratings yet
- MindDocument391 pagesMindatyanta wibhawaNo ratings yet
- Contact Person Leaflet - RemovedDocument9 pagesContact Person Leaflet - RemovedLens ProjectNo ratings yet
- Compendium of Spencerian or Semi-Angular Penmanship SpencerDocument60 pagesCompendium of Spencerian or Semi-Angular Penmanship SpencerTRAN NGOC100% (1)
- Chapter 10Document14 pagesChapter 10Jesper PetersenNo ratings yet
- ST CoolegemDocument14 pagesST CoolegemSimsoneNo ratings yet
- ΜΠΑ 158/2019Document6 pagesΜΠΑ 158/2019Λεωνίδας Στάμος100% (2)
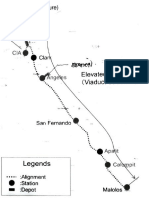
- Sa Fernando: Elevated Works Viaduct StructureDocument1 pageSa Fernando: Elevated Works Viaduct StructureEricia GomezNo ratings yet
- Guide To Darbar Sahib 1903Document49 pagesGuide To Darbar Sahib 1903Uday SinghNo ratings yet
- The Landowners of Ireland BurghDocument513 pagesThe Landowners of Ireland BurghJohn MulleeNo ratings yet
- Legendary Abs II PDFDocument48 pagesLegendary Abs II PDFSatyan Wadhwa100% (1)
- Hayman - How To Read PlayDocument96 pagesHayman - How To Read PlayBilal Yiğit İnalNo ratings yet
- Ar Final WorksheetDocument4 pagesAr Final WorksheetdujalshahNo ratings yet
- Ompu Ai Cma: Eliza A Computer Program For The Study of Natural Language Communication Between Man and MachineDocument10 pagesOmpu Ai Cma: Eliza A Computer Program For The Study of Natural Language Communication Between Man and Machinerpimenta30No ratings yet
- Summa S One Series Product PresentationDocument32 pagesSumma S One Series Product PresentationPU PUNo ratings yet
- Into A Wealthy PlaceDocument2 pagesInto A Wealthy PlaceJohn Reve GamboaNo ratings yet
- March, 2023 Domestic: Customer Number: Billing Month: Tariff/Customer Class: Bill ID: 158856022712Document1 pageMarch, 2023 Domestic: Customer Number: Billing Month: Tariff/Customer Class: Bill ID: 158856022712Yasir KhanNo ratings yet
- Tanuj Ghimire - CVDocument4 pagesTanuj Ghimire - CVsujankhanal10No ratings yet
- Black 1950 PDFDocument10 pagesBlack 1950 PDFcis freteNo ratings yet
- ComantDocument134 pagesComantsoniaxNo ratings yet
- Breed A Monster RubricDocument1 pageBreed A Monster Rubricapi-495151215No ratings yet
- Test 5-11-2019 Excretory System - Pharmacist Zaheer AbbasDocument3 pagesTest 5-11-2019 Excretory System - Pharmacist Zaheer AbbasabbaszaheerNo ratings yet
- ISRAEL PowerpointDocument86 pagesISRAEL PowerpointRamprasad AkshantulaNo ratings yet
- Construction Quality Control Plan DraftDocument24 pagesConstruction Quality Control Plan Draftmozartjr22No ratings yet
- Snoo Wilson Adaptation of The BedbugDocument49 pagesSnoo Wilson Adaptation of The BedbugMike Vanden HeuvelNo ratings yet
- Electrical Systems Instructions Manual Sames DRT6364 UkDocument26 pagesElectrical Systems Instructions Manual Sames DRT6364 UkGermando NUNESNo ratings yet
- ECOS Data Report 3063Document13 pagesECOS Data Report 3063Sarra Chouchene0% (1)
- ILVODocument2 pagesILVOAna-Maria RamazanNo ratings yet
- Spa 20008080VDocument1 pageSpa 20008080Vmichele DSNo ratings yet
- Answer Key-Worksheet Booklet - Good Health PG 41-48Document8 pagesAnswer Key-Worksheet Booklet - Good Health PG 41-48Random VideosNo ratings yet
- The Pahari School AssignmentDocument3 pagesThe Pahari School AssignmentKushagra HaritNo ratings yet
- Type Abz PDFDocument15 pagesType Abz PDFle khánhNo ratings yet
- SAE AS4059F Table1Document2 pagesSAE AS4059F Table1CherryNo ratings yet
- Manalaysay JPT Thesis With Approval PDFDocument103 pagesManalaysay JPT Thesis With Approval PDFTheresa Marie PrestoNo ratings yet
- The Calculation of The Mean Radiant Temperature of A Subject Exposed To The Solar Radiation-A Generalised AlgorithmDocument9 pagesThe Calculation of The Mean Radiant Temperature of A Subject Exposed To The Solar Radiation-A Generalised AlgorithmGiulia SantoroNo ratings yet
- The Said and The UnsaidDocument19 pagesThe Said and The UnsaidOzana BudauNo ratings yet
- Scenema M88 EngineDocument1 pageScenema M88 EngineDrSomnath999No ratings yet
- CSCHE 2017 Program 1020Document31 pagesCSCHE 2017 Program 1020danielairyNo ratings yet
- Non Destructive TestingDocument9 pagesNon Destructive TestingAhmed KhanNo ratings yet
- Atmel 11121 32 Bit Cortex A5 Microcontroller SAMA5D3 DatasheetDocument1,710 pagesAtmel 11121 32 Bit Cortex A5 Microcontroller SAMA5D3 DatasheetCan CerberusNo ratings yet
- Ebook Physics of Cryogenics An Ultralow Temperature Phenomenon PDF Full Chapter PDFDocument67 pagesEbook Physics of Cryogenics An Ultralow Temperature Phenomenon PDF Full Chapter PDFlouise.fleming716100% (25)
- Beacon Atlantic Short Spec R1 141118 NBDocument4 pagesBeacon Atlantic Short Spec R1 141118 NBRayodcNo ratings yet
- Cambridge International Advanced Subsidiary and Advanced LevelDocument12 pagesCambridge International Advanced Subsidiary and Advanced LevelTerTalks ChikweyaNo ratings yet