You might also like
- Incident/Investigation: Rowan County Sheriffs OfficeDocument1 pageIncident/Investigation: Rowan County Sheriffs OfficeAnonymous k3grAlCT1eNo ratings yet
- Application For Trillium Drug BenefitsDocument5 pagesApplication For Trillium Drug BenefitshassanNo ratings yet
- Pertussis Surveillance Worksheet: DETACH HERE and Transmit Only Lower Portion If Sent To CDCDocument2 pagesPertussis Surveillance Worksheet: DETACH HERE and Transmit Only Lower Portion If Sent To CDCNora VirdaNo ratings yet
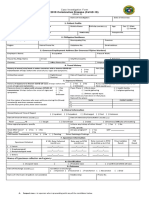
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormJudeLaxNo ratings yet
- Patient'S Full Name Complete AddressDocument3 pagesPatient'S Full Name Complete AddressMirah MonteroNo ratings yet
- Coronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalDocument1 pageCoronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalKarsenley Cal-el Iddig BurigsayNo ratings yet
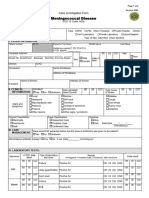
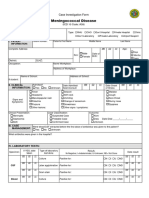
- CIF-Meningococcal DiseaseDocument2 pagesCIF-Meningococcal DiseaseIvy marie BonNo ratings yet
- Human Rabies Case Report: Patient InformationDocument7 pagesHuman Rabies Case Report: Patient Informationdaniel FernandezNo ratings yet
- DOH PIDSR COVID-19 CIF TemplateDocument1 pageDOH PIDSR COVID-19 CIF TemplateMargaux Faith CCNo ratings yet
- Anthrax CifDocument2 pagesAnthrax CifMary Anne Grace GarridoNo ratings yet
- CoViD19-CIF-v6-Fillable QCv3-2Document1 pageCoViD19-CIF-v6-Fillable QCv3-2Patrice De CastroNo ratings yet
- Dengue / Severe Dengue Case Report: Patient InformationDocument6 pagesDengue / Severe Dengue Case Report: Patient InformationShubham SinghNo ratings yet
- Adverse Events Following Immunization: Philippine Integrated DiseaseDocument2 pagesAdverse Events Following Immunization: Philippine Integrated DiseaseRex DoctoNo ratings yet
- CoViD19-Covid Investigation FormDocument1 pageCoViD19-Covid Investigation FormMc Arem PaghunasanNo ratings yet
- Police Report Concerning Vandalism of "Silent Sam" Statue at University of North Carolina-Chapel HillDocument1 pagePolice Report Concerning Vandalism of "Silent Sam" Statue at University of North Carolina-Chapel HillThe College FixNo ratings yet
- CDPH 8657Document6 pagesCDPH 8657Akshat SharmaNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormPresinto Dos Parañaque KnightsNo ratings yet
- Communicable Disease Report FormDocument1 pageCommunicable Disease Report FormBeyza GemiciNo ratings yet
- Typhoid Fever Surveillance ReportDocument2 pagesTyphoid Fever Surveillance ReportMarketing HydNo ratings yet
- Typhoid and Paratyphoid Fever Case ReportDocument6 pagesTyphoid and Paratyphoid Fever Case ReportMohan ChikkalaNo ratings yet
- Typhoid Carrier Case Report: Please Complete This Form Only For Chronic Typhoid CarriersDocument5 pagesTyphoid Carrier Case Report: Please Complete This Form Only For Chronic Typhoid CarriersVinay PantNo ratings yet
- Application For ServicesDocument4 pagesApplication For ServicesNermeen ElsayedNo ratings yet
- 2019 Coronavirus Disease (Covid-19) : 1. Patient ProfileDocument1 page2019 Coronavirus Disease (Covid-19) : 1. Patient ProfileMarythel CamachoNo ratings yet
- New Cif FormDocument2 pagesNew Cif FormNovie FeneciosNo ratings yet
- Form No 3 Annexure C See Rule 5 of Himachal Pradesh Registration of Birth and Death Rules, 2003 Still Birth Report Form Still Birth ReportDocument2 pagesForm No 3 Annexure C See Rule 5 of Himachal Pradesh Registration of Birth and Death Rules, 2003 Still Birth Report Form Still Birth ReportvijayNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormBabiejoy Beltran AceloNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormBabiejoy Beltran AceloNo ratings yet
- Unit 3 Lab Suspicious BehaviorDocument5 pagesUnit 3 Lab Suspicious BehaviorDanielle Jessica PatrickNo ratings yet
- Adr 2Document2 pagesAdr 2ok2bwellNo ratings yet
- Local Record Id: H. Local Subject Id:: Specimen Type CDC ID (From 50.34 Submission) Other Specimen (Specify)Document5 pagesLocal Record Id: H. Local Subject Id:: Specimen Type CDC ID (From 50.34 Submission) Other Specimen (Specify)Ashwin babuNo ratings yet
- Saric CifDocument1 pageSaric CifMarav SymbNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormShiela E. EladNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormMizraim TupazNo ratings yet
- Case Questionnaire COVID-19 (Novel Coronavirus) - Part A: InformationDocument11 pagesCase Questionnaire COVID-19 (Novel Coronavirus) - Part A: InformationHenrietta CookNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormHerbert Tierra Ponce Jr.100% (1)
- Travel Claim Form - Medical ExpensesDocument3 pagesTravel Claim Form - Medical Expensesshyamsundertripathi270No ratings yet
- Nicanor Reyes Medical Foundation: Far Eastern UniversityDocument2 pagesNicanor Reyes Medical Foundation: Far Eastern UniversitygAARaNo ratings yet
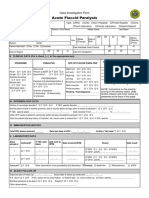
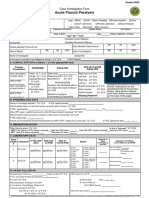
- Acute Flaccid Paralysis: Case Investigation FormDocument2 pagesAcute Flaccid Paralysis: Case Investigation FormBarbie CincoNo ratings yet
- Form 1Document1 pageForm 1Abdur RasyidNo ratings yet
- Household Questionnaires For CensusDocument29 pagesHousehold Questionnaires For Censussamurai.stewart.hamiltonNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument2 pagesCoronavirus Disease (COVID-19) : Case Investigation FormChamee MallillinNo ratings yet
- Case Investigation Form - Acute Flaccid ParalysisDocument2 pagesCase Investigation Form - Acute Flaccid Paralysisclaverialc10No ratings yet
- CIF TemplateDocument2 pagesCIF Templateluvaire23No ratings yet
- Cif AfpDocument2 pagesCif Afpninzah wanzahNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormmaelisaNo ratings yet
- Adult Passport AppDocument7 pagesAdult Passport AppAnonymous x0xGvegk8No ratings yet
- VHemorrhagic Fev RepDocument7 pagesVHemorrhagic Fev RepJayanth NayakNo ratings yet
- Position Applied For: Other Position(s) of Interest: Salary Expected: (Net/ Gross) Date Available To StartDocument4 pagesPosition Applied For: Other Position(s) of Interest: Salary Expected: (Net/ Gross) Date Available To StartalfathNo ratings yet
- Case Investigation Form - Meningococcal DiseaseDocument2 pagesCase Investigation Form - Meningococcal Diseaseclaverialc10No ratings yet
- COVID 19 Form 1 1 PDFDocument1 pageCOVID 19 Form 1 1 PDFTuguinay EmilynNo ratings yet
- PNC - A3-1Document5 pagesPNC - A3-1dabashgetNo ratings yet
- REDACTED Stanley Fairfax Form5 ChargeDocument12 pagesREDACTED Stanley Fairfax Form5 ChargeWUSA9 TVNo ratings yet
- Coronavirus Disease (COVID-19) : Case Investigation FormDocument1 pageCoronavirus Disease (COVID-19) : Case Investigation FormChum ChitaruNo ratings yet
- Avon Recruiting Appointment FormDocument1 pageAvon Recruiting Appointment FormkallieNo ratings yet
- Drug Study 1Document2 pagesDrug Study 1Hafza MacabatoNo ratings yet
- CONSENT FOR BIOPSY v2Document1 pageCONSENT FOR BIOPSY v2Bhumika SharmaNo ratings yet
- Acute AbdomenDocument60 pagesAcute AbdomenAnish DhamiNo ratings yet
- Bacterial Skin InfectionsDocument9 pagesBacterial Skin InfectionskateverdadNo ratings yet
- Paragonimus Family NEWDocument19 pagesParagonimus Family NEWADARSH ARUNNo ratings yet
- Nail DisordersDocument42 pagesNail DisordersJessica MotarNo ratings yet
- Guidelines For PMDT in India-Low PDFDocument334 pagesGuidelines For PMDT in India-Low PDFjai kishanNo ratings yet
- BINGE EATING DISORDER, WLM Cia 3Document6 pagesBINGE EATING DISORDER, WLM Cia 3PrathibaNo ratings yet
- Malignant Salivary Gland Tumors - StatPearls - NCBI BookshelfDocument31 pagesMalignant Salivary Gland Tumors - StatPearls - NCBI BookshelfGisela LalitaNo ratings yet
- How To Code StrokeDocument13 pagesHow To Code StrokePanelqy AninditoNo ratings yet
- DRUG STUDY (Sertraline) - SANGUYO, CB.Document5 pagesDRUG STUDY (Sertraline) - SANGUYO, CB.Camille SanguyoNo ratings yet
- Certificate of IsolationDocument19 pagesCertificate of IsolationSweet SimyunnNo ratings yet
- Wong 1996Document6 pagesWong 1996irfan ahmad hNo ratings yet
- Gero Aging Review 2023-1Document41 pagesGero Aging Review 2023-1indo 5S100% (1)
- BronchitisDocument2 pagesBronchitisАнастасия ПащенкоNo ratings yet
- 2020 Ehra-hrs-Aphrs-lahrs Risk AssessmentDocument48 pages2020 Ehra-hrs-Aphrs-lahrs Risk AssessmentRui FonteNo ratings yet
- Carvedilol Vs Metoprolol A Comparison of Effects oDocument6 pagesCarvedilol Vs Metoprolol A Comparison of Effects oBenjamin GonzalezNo ratings yet
- Ferrum PhosphoricumDocument4 pagesFerrum PhosphoricumDr-Sayantan BasuNo ratings yet
- ABI Beat The Heat 2023Document15 pagesABI Beat The Heat 2023VinodNo ratings yet
- Cycloid Vibration WEBDocument19 pagesCycloid Vibration WEBFabian DeeNo ratings yet
- DS (Fenofibrate)Document5 pagesDS (Fenofibrate)Mary April MendezNo ratings yet
- Chronic Immune Sensory Polyradiculopathy (CISP) : Stephanie Ong, Adam CassidyDocument4 pagesChronic Immune Sensory Polyradiculopathy (CISP) : Stephanie Ong, Adam Cassidylors93No ratings yet
- Research Proposal On Diabetes Mellitus Screening by Masafu Hospital GroupDocument11 pagesResearch Proposal On Diabetes Mellitus Screening by Masafu Hospital GroupAli emillyNo ratings yet
- 366-Article Text-1782-1-10-20230930Document6 pages366-Article Text-1782-1-10-20230930Elang kurniati Elang kurniatiNo ratings yet
- IM RheumatologyDocument56 pagesIM RheumatologySujoud AbuserdanehNo ratings yet
- Chemotherapy in Ent My PTDocument25 pagesChemotherapy in Ent My PTRajarshi Sannigrahi0% (1)
- Liver CancerDocument1 pageLiver CancerTarantado67% (3)
- Infantile Hemangioendothelioma: Bafana Elliot Hlatshwayo, Daba Ipfi, Sipho SitholeDocument4 pagesInfantile Hemangioendothelioma: Bafana Elliot Hlatshwayo, Daba Ipfi, Sipho SitholeDrAbdullah HajarNo ratings yet
- Final Health Care Associated InfectionDocument23 pagesFinal Health Care Associated Infectionramanand chaudharyNo ratings yet
- Literature Review On Cancer PDFDocument4 pagesLiterature Review On Cancer PDFafmzinuvouzeny100% (1)