You might also like
- BaddiDocument43 pagesBaddi01copy100% (3)
- Chest X Ray Detection Project ReportDocument45 pagesChest X Ray Detection Project ReportNikhil Sharma100% (1)
- Pneumonia Lung Opacity Detection and Segmentation in Chest X-Rays by Using Transfer Learning of The Mask R-CNNDocument9 pagesPneumonia Lung Opacity Detection and Segmentation in Chest X-Rays by Using Transfer Learning of The Mask R-CNNWeb ResearchNo ratings yet
- A Survey Paper On Pneumonia Detection in Chest X-Ray Images Using An Ensemble of Deep LearningDocument9 pagesA Survey Paper On Pneumonia Detection in Chest X-Ray Images Using An Ensemble of Deep LearningIJRASETPublicationsNo ratings yet
- Decoding Pneumonia: Leveraging CNNS For Accurate Chest X-Ray ClassificationDocument7 pagesDecoding Pneumonia: Leveraging CNNS For Accurate Chest X-Ray ClassificationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Covid 19Document18 pagesCovid 19AISHWARYA PANDITNo ratings yet
- Diagnosis of Pneumonia From Chest X-Ray Images Using Deep LearningDocument5 pagesDiagnosis of Pneumonia From Chest X-Ray Images Using Deep LearningShoumik MuhtasimNo ratings yet
- 2004 06578 PDFDocument19 pages2004 06578 PDFSumaNo ratings yet
- ChapterDocument22 pagesChapterAparna MittalNo ratings yet
- 2023 An Improved Faster R-CNN Algorithm For Assisted Detection of Lung NodulesDocument9 pages2023 An Improved Faster R-CNN Algorithm For Assisted Detection of Lung NodulesgraythomasinNo ratings yet
- Automatic Detection of Pneumonia On Compressed Sensing Images Using Deep LearningDocument4 pagesAutomatic Detection of Pneumonia On Compressed Sensing Images Using Deep LearningRahul ShettyNo ratings yet
- Development of Hybrid Convolutional Neural Network and Autoregressive Integrated Moving Average On Computed Tomography Image ClassificationDocument9 pagesDevelopment of Hybrid Convolutional Neural Network and Autoregressive Integrated Moving Average On Computed Tomography Image ClassificationIAES IJAINo ratings yet
- Paper2 15pagesDocument15 pagesPaper2 15pagesCharlène Béatrice Bridge NduwimanaNo ratings yet
- ICMR - Reproducible AI in Medicine and HealthDocument9 pagesICMR - Reproducible AI in Medicine and Healthvignesh16vlsiNo ratings yet
- Ies50839 2020 9231540Document5 pagesIes50839 2020 9231540AhdiatShinigamiNo ratings yet
- Detecting Tuberculosis in Chest X-Ray Images UsingDocument5 pagesDetecting Tuberculosis in Chest X-Ray Images UsingShoumik MuhtasimNo ratings yet
- Anapub Paper TemplateDocument10 pagesAnapub Paper Templatebdhiyanu87No ratings yet
- Jurnal CNN PneumoniaDocument5 pagesJurnal CNN PneumoniadaffaNo ratings yet
- Detecting Pneumonia Using Convolutions and Dynamic Capsule Routing For Chest X-Ray ImagesDocument30 pagesDetecting Pneumonia Using Convolutions and Dynamic Capsule Routing For Chest X-Ray ImagesShoumik MuhtasimNo ratings yet
- 项目论文2:美国有线电视新闻网医学影像诊断新冠肺炎感染综述Document8 pages项目论文2:美国有线电视新闻网医学影像诊断新冠肺炎感染综述lujunNo ratings yet
- Prediction of Pneumonia Using CNNDocument9 pagesPrediction of Pneumonia Using CNNIJRASETPublicationsNo ratings yet
- Measurement: Amit Kumar Jaiswal, Prayag Tiwari, Sachin Kumar, Deepak Gupta, Ashish Khanna, Joel J.P.C. RodriguesDocument8 pagesMeasurement: Amit Kumar Jaiswal, Prayag Tiwari, Sachin Kumar, Deepak Gupta, Ashish Khanna, Joel J.P.C. RodriguesDiego Alejandro Betancourt PradaNo ratings yet
- Deep Convolutional Neural Networks For Lung Nodule Detection: Improvement in Small Nodule IdentificationDocument9 pagesDeep Convolutional Neural Networks For Lung Nodule Detection: Improvement in Small Nodule Identificationdreadrebirth2342No ratings yet
- Research Paper On Lung DetecionDocument5 pagesResearch Paper On Lung DetecionHirdesh KumarNo ratings yet
- Medical Image Classification Using CNN ReportDocument19 pagesMedical Image Classification Using CNN ReportSameer Thadimarri AP20110010028No ratings yet
- 1 s2.0 S0957417422016372 MainDocument14 pages1 s2.0 S0957417422016372 MainMd NahiduzzamanNo ratings yet
- (IJCST-V11I2P5) :Dr.S.Selvakani, K.Vasumathi, M.GopiDocument5 pages(IJCST-V11I2P5) :Dr.S.Selvakani, K.Vasumathi, M.GopiEighthSenseGroupNo ratings yet
- IJEET TemplateDocument5 pagesIJEET TemplateIgt SuryawanNo ratings yet
- An Efficient CNN Model For COVID-19 Disease DetectDocument12 pagesAn Efficient CNN Model For COVID-19 Disease Detectnasywa rahmatullailyNo ratings yet
- Deep Neural Network Ensemble For Pneumonia LocalizationDocument12 pagesDeep Neural Network Ensemble For Pneumonia LocalizationAmílcar CáceresNo ratings yet
- Lung Tumor Localization and Visualization in ChestDocument17 pagesLung Tumor Localization and Visualization in ChestAida Fitriyane HamdaniNo ratings yet
- 2023 Detection and Classification of COVID-19 by Using Faster R-CNN and Mask R-CNN On CT ImagesDocument15 pages2023 Detection and Classification of COVID-19 by Using Faster R-CNN and Mask R-CNN On CT ImagesgraythomasinNo ratings yet
- Identifying Drug-Resistant Tuberculosis in Chest Radiographs Evaluation of CNN Architectures and Training StrategiesDocument4 pagesIdentifying Drug-Resistant Tuberculosis in Chest Radiographs Evaluation of CNN Architectures and Training StrategiesManya K MNo ratings yet
- Chest X-Ray Outlier Detection Model Using Dimension Reduction and Edge DetectionDocument11 pagesChest X-Ray Outlier Detection Model Using Dimension Reduction and Edge DetectionHardik AgrawalNo ratings yet
- 1 s2.0 S138650562030959X MainDocument9 pages1 s2.0 S138650562030959X Main1No ratings yet
- Lung and Pancreatic Tumor Characterization in The Deep Learning Era: Novel Supervised and Unsupervised Learning ApproachesDocument11 pagesLung and Pancreatic Tumor Characterization in The Deep Learning Era: Novel Supervised and Unsupervised Learning ApproachesVipin GeorgeNo ratings yet
- Deep Learning Approach For Unprecedented Lung Disease PrognosisDocument5 pagesDeep Learning Approach For Unprecedented Lung Disease PrognosisMulla Abdul FaheemNo ratings yet
- Survey PneumoniaDocument7 pagesSurvey Pneumonia20220804039No ratings yet
- Pneumonia Disease Detection Using Deep LearningDocument6 pagesPneumonia Disease Detection Using Deep LearningIJRASETPublicationsNo ratings yet
- Lung CancerDocument10 pagesLung Cancerbvkarthik2711No ratings yet
- Comparison of Deep Learning Algorithms For Pneumonia DetectionDocument5 pagesComparison of Deep Learning Algorithms For Pneumonia DetectionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Enhancing Early Detection of Lung Cancer With An Advanced ALCDC System Utilizing Convolutional Neural NetworkDocument5 pagesEnhancing Early Detection of Lung Cancer With An Advanced ALCDC System Utilizing Convolutional Neural NetworkInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Research Article An Improved Covid-19 Detection Using Gan-Based Data Augmentation and Novel Qunet-Based ClassificationDocument9 pagesResearch Article An Improved Covid-19 Detection Using Gan-Based Data Augmentation and Novel Qunet-Based ClassificationNaoual NassiriNo ratings yet
- Pneumonia Detection in X-Ray Chest Images BasedDocument7 pagesPneumonia Detection in X-Ray Chest Images BasedyuniNo ratings yet
- Resume Paper AgisDocument2 pagesResume Paper AgisAulia AgistaNo ratings yet
- Zhang Et Al. - 2022 - A Multi-Channel Deep Convolutional Neural NetworkDocument11 pagesZhang Et Al. - 2022 - A Multi-Channel Deep Convolutional Neural NetworkJamesLeeNo ratings yet
- Document3 TexDocument4 pagesDocument3 TexNavin M ANo ratings yet
- Artificial Intelligence 1Document8 pagesArtificial Intelligence 1Andy BaiNo ratings yet
- Artificial Intelligence in Respirato - 2021 - Archivos de Bronconeumolog A EnglDocument2 pagesArtificial Intelligence in Respirato - 2021 - Archivos de Bronconeumolog A EnglMomoh GaiusNo ratings yet
- Identifying Pulmonary Nodules or Masses On Chest Radiography Using Deep Learning: External Validation and Strategies To Improve Clinical PracticeDocument8 pagesIdentifying Pulmonary Nodules or Masses On Chest Radiography Using Deep Learning: External Validation and Strategies To Improve Clinical PracticeYuriansyah Dwi Rahma PutraNo ratings yet
- 10 1109@iccsp48568 2020 9182258Document4 pages10 1109@iccsp48568 2020 9182258mindaNo ratings yet
- SirishKaushik2020 Chapter PneumoniaDetectionUsingConvoluDocument14 pagesSirishKaushik2020 Chapter PneumoniaDetectionUsingConvoluMatiqul IslamNo ratings yet
- Pneumonia Detection Using Convolutional Neural Networks (CNNS)Document14 pagesPneumonia Detection Using Convolutional Neural Networks (CNNS)shekhar1405No ratings yet
- Ensemble Deep Learning For Tuberculosis Detection Using Chest X-Ray and Canny Edge Detected ImagesDocument7 pagesEnsemble Deep Learning For Tuberculosis Detection Using Chest X-Ray and Canny Edge Detected ImagesIAES IJAINo ratings yet
- Breast Cancer Classification in Ultrasound ImagesDocument4 pagesBreast Cancer Classification in Ultrasound ImagesTefeNo ratings yet
- CNN Architecture Optimization Using Bio Inspired Algor - 2022 - Computers in BioDocument13 pagesCNN Architecture Optimization Using Bio Inspired Algor - 2022 - Computers in BioFarhan MaulanaNo ratings yet
- Hybrid Deep Learning For Detecting Lung Diseases From X-Ray ImagesDocument23 pagesHybrid Deep Learning For Detecting Lung Diseases From X-Ray ImagesLK AnhDungNo ratings yet
- Application of Deep Learning Techniques For Detection of COVID-19 Casesusing Chest X-Ray Images A Comprehensive StudyDocument12 pagesApplication of Deep Learning Techniques For Detection of COVID-19 Casesusing Chest X-Ray Images A Comprehensive StudyHarshini N BNo ratings yet
- Deep Learning Assisted Predict of Lung Cancer On Computed Tomography Images Using The Adaptive Hierarchical Heuristic Mathematical ModelDocument11 pagesDeep Learning Assisted Predict of Lung Cancer On Computed Tomography Images Using The Adaptive Hierarchical Heuristic Mathematical Modelswathi sNo ratings yet
- 2D3D Clasification 01Document11 pages2D3D Clasification 01sadNo ratings yet
- Course: EC2P001 Introduction To Electronics Lab: Indian Institute of Technology Bhubaneswar School of Electrical ScienceDocument5 pagesCourse: EC2P001 Introduction To Electronics Lab: Indian Institute of Technology Bhubaneswar School of Electrical ScienceAnik ChaudhuriNo ratings yet
- Earning and Stock Split - Asquith Et Al 1989Document18 pagesEarning and Stock Split - Asquith Et Al 1989Fransiskus ShaulimNo ratings yet
- Women's Safety Measures Through Sensor Device Using Iot: T.Sathyapriya, R.Auxilia Anitha MaryDocument3 pagesWomen's Safety Measures Through Sensor Device Using Iot: T.Sathyapriya, R.Auxilia Anitha MaryCSE ROHININo ratings yet
- Report On: Course: MKT 634, Section-1Document35 pagesReport On: Course: MKT 634, Section-1wasifNo ratings yet
- OSY - Chapter1Document11 pagesOSY - Chapter1Rupesh BavgeNo ratings yet
- Nokia Lumia 925 RM-892 - 893 - 910 L1L2 Service ManualDocument63 pagesNokia Lumia 925 RM-892 - 893 - 910 L1L2 Service ManualCretu PaulNo ratings yet
- General Purpose Engine: GX100T GX100UT GX100RTDocument66 pagesGeneral Purpose Engine: GX100T GX100UT GX100RTLupin GonzalezNo ratings yet
- A Covid-19 Based Temperature Detection and Contactless Attendance Monitoring System Using Iris RecognitionDocument18 pagesA Covid-19 Based Temperature Detection and Contactless Attendance Monitoring System Using Iris Recognitionshreya tripathiNo ratings yet
- English Theses PDFDocument630 pagesEnglish Theses PDFshakhy azadNo ratings yet
- Credential Harvestor FacebookDocument23 pagesCredential Harvestor FacebookJ Anthony GreenNo ratings yet
- Databricks Data Processing Addendum 25 Sept 2021 FINALDocument12 pagesDatabricks Data Processing Addendum 25 Sept 2021 FINALVaibhav AntilNo ratings yet
- Konica Minolta Bizhub C 6501 CatalogDocument0 pagesKonica Minolta Bizhub C 6501 CatalogDiscountCopierCenterNo ratings yet
- AC43-18 CHG 1-2 Fabrication of Parts by Maintenance Personnel PDFDocument20 pagesAC43-18 CHG 1-2 Fabrication of Parts by Maintenance Personnel PDFJesseNo ratings yet
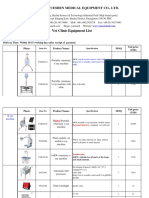
- 2017 Vet Clinic Equipment Pricelist From YuesenmedDocument24 pages2017 Vet Clinic Equipment Pricelist From YuesenmedVictor TomalaNo ratings yet
- Huawei GPON HG8247H WithRouter v2 PDFDocument4 pagesHuawei GPON HG8247H WithRouter v2 PDFJose Norton DoriaNo ratings yet
- CIVL 4750 Numerical Solutions To Geotechnical Problems: I: TA: T V: Tuesday/ C ODocument3 pagesCIVL 4750 Numerical Solutions To Geotechnical Problems: I: TA: T V: Tuesday/ C OChoffo YannickNo ratings yet
- Installation Guide: EV Power Chargers 3kW HEDocument12 pagesInstallation Guide: EV Power Chargers 3kW HEnikhom_dk1565No ratings yet
- HP Compac 4000 Pro Small PCDocument4 pagesHP Compac 4000 Pro Small PCHebert Castañeda FloresNo ratings yet
- Gmail - NMAT by GMAC Exam Appointment ConfirmationDocument2 pagesGmail - NMAT by GMAC Exam Appointment ConfirmationPankti BaxiNo ratings yet
- Moduino ENDocument4 pagesModuino ENaabejaroNo ratings yet
- GFK2749 - RX3i PSM PDFDocument100 pagesGFK2749 - RX3i PSM PDFgabsNo ratings yet
- MT 720 Transfer of A Documentary CreditDocument3 pagesMT 720 Transfer of A Documentary CreditA. T. M. Anisur Rabbani100% (1)
- Problem StatementDocument4 pagesProblem Statementjanardhan gortiNo ratings yet
- Diaphragm Pressure Gauge Guard MDM 902: Corrosion-Free Pressure Transmission For Aggressive MediaDocument4 pagesDiaphragm Pressure Gauge Guard MDM 902: Corrosion-Free Pressure Transmission For Aggressive Mediathiago weniskleyNo ratings yet
- JellDocument1 pageJellMuhammad DanuNo ratings yet
- Certificacion ORCA PDFDocument42 pagesCertificacion ORCA PDFedmuarizt7078No ratings yet
- Green ComputingDocument7 pagesGreen Computingerwin.dee.cicsNo ratings yet
- Kendriya Vidyalaya Sangathan Jaipur Region: Sample Question Paper (Term-I)Document7 pagesKendriya Vidyalaya Sangathan Jaipur Region: Sample Question Paper (Term-I)Samira FarooquiNo ratings yet
- Feed Manufacturing-GrindingDocument33 pagesFeed Manufacturing-GrindingDr Anais AsimNo ratings yet