You might also like
- Brand Plan - SingulairDocument11 pagesBrand Plan - Singulairshashank100% (2)
- Pumpkin Cultivation and PracticesDocument11 pagesPumpkin Cultivation and PracticesGhorpade GsmNo ratings yet
- Lululemon Style GuideDocument15 pagesLululemon Style Guideapi-263257893No ratings yet
- C28x WorkshopDocument400 pagesC28x WorkshopMarcio De Andrade VogtNo ratings yet
- GMDS - Course - FinalDocument282 pagesGMDS - Course - FinalLuisPazPerdomo100% (1)
- PosdmDocument29 pagesPosdmChandraBhushan67% (3)
- SF 10 23Document6 pagesSF 10 23Gusman TriadyNo ratings yet
- SF 15 23Document7 pagesSF 15 23Shivkumar JadhavNo ratings yet
- SF 29 23Document6 pagesSF 29 23Shivkumar JadhavNo ratings yet
- SF 26 23Document6 pagesSF 26 23Shivkumar JadhavNo ratings yet
- SF 17 22Document5 pagesSF 17 22Shivkumar JadhavNo ratings yet
- SF 02 24Document6 pagesSF 02 24Shivkumar JadhavNo ratings yet
- SF 23 22Document6 pagesSF 23 22Shivkumar JadhavNo ratings yet
- SF 06 24Document6 pagesSF 06 24Shivkumar JadhavNo ratings yet
- SF 22 23Document6 pagesSF 22 23Shivkumar JadhavNo ratings yet
- SF 24 23Document5 pagesSF 24 23Shivkumar JadhavNo ratings yet
- SF 06 22Document5 pagesSF 06 22Shivkumar JadhavNo ratings yet
- SF 23 23Document5 pagesSF 23 23Shivkumar JadhavNo ratings yet
- SF-34-21-January 2021Document6 pagesSF-34-21-January 2021Shivkumar JadhavNo ratings yet
- SF 16 23Document6 pagesSF 16 23Shivkumar JadhavNo ratings yet
- SF 18 23Document6 pagesSF 18 23Shahriyar ShahNo ratings yet
- Imcasf 22 19Document5 pagesImcasf 22 19Pippo TopolinoNo ratings yet
- IMCASF - Oct 20Document6 pagesIMCASF - Oct 20Shivkumar JadhavNo ratings yet
- SF 17 22Document6 pagesSF 17 22Shivkumar JadhavNo ratings yet
- SF 16 22Document6 pagesSF 16 22Shivkumar JadhavNo ratings yet
- SF 01 24Document7 pagesSF 01 24Shahriyar ShahNo ratings yet
- SF 11 23Document6 pagesSF 11 23Shivkumar JadhavNo ratings yet
- IMCASF - Sept 20Document6 pagesIMCASF - Sept 20Shivkumar JadhavNo ratings yet
- Imcasf 31 21Document6 pagesImcasf 31 21Paulo IsabelNo ratings yet
- SF 05 22Document5 pagesSF 05 22Shivkumar JadhavNo ratings yet
- SF 28 22Document5 pagesSF 28 22Shivkumar JadhavNo ratings yet
- IMCASF - Aug 17Document7 pagesIMCASF - Aug 17Shivkumar JadhavNo ratings yet
- IMCASF - Oct 18Document5 pagesIMCASF - Oct 18Shivkumar JadhavNo ratings yet
- SF 03 24sssDocument6 pagesSF 03 24sssShahriyar ShahNo ratings yet
- IMCASF - Jan 18Document5 pagesIMCASF - Jan 18Shivkumar JadhavNo ratings yet
- SF 08 22Document6 pagesSF 08 22Shivkumar JadhavNo ratings yet
- SF 08 24Document6 pagesSF 08 24Shivkumar JadhavNo ratings yet
- IMCASF - Feb 19Document6 pagesIMCASF - Feb 19Shivkumar JadhavNo ratings yet
- IMCASF - Oct 17Document6 pagesIMCASF - Oct 17Shivkumar JadhavNo ratings yet
- IMCASF - Jun 17Document5 pagesIMCASF - Jun 17Shivkumar JadhavNo ratings yet
- SF 19 22Document6 pagesSF 19 22Shivkumar JadhavNo ratings yet
- IMCASF - Dec 17Document6 pagesIMCASF - Dec 17Shivkumar JadhavNo ratings yet
- IMCASF - Jun 18Document5 pagesIMCASF - Jun 18Shivkumar JadhavNo ratings yet
- IMCASF - Feb 16Document6 pagesIMCASF - Feb 16Shivkumar JadhavNo ratings yet
- IMCASF - May 20Document6 pagesIMCASF - May 20Shivkumar JadhavNo ratings yet
- Differential PressureDocument3 pagesDifferential Pressurethanhbem301No ratings yet
- IMCASF - Nov 16Document7 pagesIMCASF - Nov 16Shivkumar JadhavNo ratings yet
- IMCASF - Aug 19Document6 pagesIMCASF - Aug 19Shivkumar JadhavNo ratings yet
- SF 07 24Document6 pagesSF 07 24Shivkumar JadhavNo ratings yet
- IMCA Safety Flashes 2009 07Document6 pagesIMCA Safety Flashes 2009 07Francisco TajúNo ratings yet
- IMCASF - Nov 18Document5 pagesIMCASF - Nov 18Shivkumar JadhavNo ratings yet
- SF 27 22Document5 pagesSF 27 22Shivkumar JadhavNo ratings yet
- IMCASF - Oct 17Document6 pagesIMCASF - Oct 17Shivkumar JadhavNo ratings yet
- IMCASF - Jun 18Document4 pagesIMCASF - Jun 18Shivkumar JadhavNo ratings yet
- Imcasf 14 20 PDFDocument6 pagesImcasf 14 20 PDFsameer hiiNo ratings yet
- SF 04 24Document6 pagesSF 04 24Shivkumar JadhavNo ratings yet
- IMCASF - Oct 18Document6 pagesIMCASF - Oct 18Shivkumar JadhavNo ratings yet
- Imcasf20 18Document6 pagesImcasf20 18Era ErmerraNo ratings yet
- SF 21 21Document6 pagesSF 21 21Natraj RamanNo ratings yet
- IMCASF - Feb 16Document7 pagesIMCASF - Feb 16Shivkumar JadhavNo ratings yet
- IMCASF - Sept 16Document7 pagesIMCASF - Sept 16Shivkumar JadhavNo ratings yet
- IMCASF - Jan 16Document6 pagesIMCASF - Jan 16Shivkumar JadhavNo ratings yet
- SF 24 22Document7 pagesSF 24 22Shivkumar JadhavNo ratings yet
- IMCASF - Jun 17Document6 pagesIMCASF - Jun 17Shivkumar JadhavNo ratings yet
- IMCASF - Sept 17Document4 pagesIMCASF - Sept 17Shivkumar JadhavNo ratings yet
- IMCASF - Oct 18Document5 pagesIMCASF - Oct 18Shivkumar JadhavNo ratings yet
- IMCASF - Mar 18Document3 pagesIMCASF - Mar 18Shivkumar JadhavNo ratings yet
- Imcasf20 18Document6 pagesImcasf20 18Era ErmerraNo ratings yet
- Imcasf21 18Document6 pagesImcasf21 18Era ErmerraNo ratings yet
- IMCASF - Mar 18Document4 pagesIMCASF - Mar 18Shivkumar JadhavNo ratings yet
- IMCASF - Mar 17Document5 pagesIMCASF - Mar 17Shivkumar JadhavNo ratings yet
- IMCASF - Jul 18Document6 pagesIMCASF - Jul 18Shivkumar JadhavNo ratings yet
- IMCASF - Feb 17Document3 pagesIMCASF - Feb 17Shivkumar JadhavNo ratings yet
- IMCASF - Nov 16Document4 pagesIMCASF - Nov 16Shivkumar JadhavNo ratings yet
- IMCASF - Jul 17Document6 pagesIMCASF - Jul 17Shivkumar JadhavNo ratings yet
- IMCASF - Jun 17Document5 pagesIMCASF - Jun 17Shivkumar JadhavNo ratings yet
- IMCASF - Jan 17Document7 pagesIMCASF - Jan 17Shivkumar JadhavNo ratings yet
- IMCA Safety Flash 29/17: What HappenedDocument5 pagesIMCA Safety Flash 29/17: What Happenedinbox012No ratings yet
- IMCASF - May 17Document7 pagesIMCASF - May 17Shivkumar JadhavNo ratings yet
- IMCASF - Mar 17Document6 pagesIMCASF - Mar 17Shivkumar JadhavNo ratings yet
- IMCASF - Jan 17Document2 pagesIMCASF - Jan 17Shivkumar JadhavNo ratings yet
- IMCASF - Feb 17Document4 pagesIMCASF - Feb 17Shivkumar JadhavNo ratings yet
- IMCASF - Aug 16Document10 pagesIMCASF - Aug 16Shivkumar JadhavNo ratings yet
- IMCASF - Jun 17Document6 pagesIMCASF - Jun 17Shivkumar JadhavNo ratings yet
- IMCASF - Oct 16Document2 pagesIMCASF - Oct 16Shivkumar JadhavNo ratings yet
- IMCASF - Nov 16Document4 pagesIMCASF - Nov 16Shivkumar JadhavNo ratings yet
- IMCASF - Oct 16Document4 pagesIMCASF - Oct 16Shivkumar JadhavNo ratings yet
- IMCASF - Oct 16Document6 pagesIMCASF - Oct 16Shivkumar JadhavNo ratings yet
- SF 02 24Document6 pagesSF 02 24Shivkumar JadhavNo ratings yet
- SF 04 24Document6 pagesSF 04 24Shivkumar JadhavNo ratings yet
- IMCASF - Apr 16Document6 pagesIMCASF - Apr 16Shivkumar JadhavNo ratings yet
- IMCASF - Apr 16Document3 pagesIMCASF - Apr 16Shivkumar JadhavNo ratings yet
- IMCASF - May 20Document3 pagesIMCASF - May 20Shivkumar JadhavNo ratings yet
- IMCASF - May 20Document6 pagesIMCASF - May 20Shivkumar JadhavNo ratings yet
- SF 28 23Document8 pagesSF 28 23Shivkumar JadhavNo ratings yet
- Disaster Management in Schools: Status ReportDocument28 pagesDisaster Management in Schools: Status ReportRamalingam VaradarajuluNo ratings yet
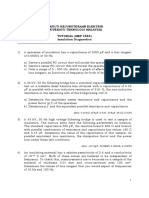
- Tutorial MEP1553 - Insulation DiagnosticsDocument4 pagesTutorial MEP1553 - Insulation DiagnosticsSharin Bin Ab GhaniNo ratings yet
- For Visual Studio User'S Manual: Motoplus SDKDocument85 pagesFor Visual Studio User'S Manual: Motoplus SDKMihail AvramovNo ratings yet
- Design, Analysis &optimization of Crankshaft Using CAEDocument6 pagesDesign, Analysis &optimization of Crankshaft Using CAEInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- Trabajo Final CERVEZA OLMECADocument46 pagesTrabajo Final CERVEZA OLMECAramon nemeNo ratings yet
- Stirling Bio Power GeneratorDocument5 pagesStirling Bio Power GeneratorAvram Stefan100% (2)
- Diagrame Des MomentsDocument1 pageDiagrame Des Momentsabdoul ndiayeNo ratings yet
- 8th Mode of FinancingDocument30 pages8th Mode of FinancingYaseen IqbalNo ratings yet
- Logcat 1676535419488Document174 pagesLogcat 1676535419488Mungkin SayaNo ratings yet
- 5GMF WP101 11 5G Rat PDFDocument26 pages5GMF WP101 11 5G Rat PDFAvik ModakNo ratings yet
- Serra Do Mel 3 A 6 - Project - VC1-ReportDocument13 pagesSerra Do Mel 3 A 6 - Project - VC1-Reportjosimar gomes da silva filhoNo ratings yet
- MCQ (Chapter 6)Document4 pagesMCQ (Chapter 6)trail meNo ratings yet
- FairyDocument1 pageFairyprojekti.jasminNo ratings yet
- Turn Pet1 Plastic Bottles Into 3d Filament With The Recreator 3d Mk5kit Ender3 b7936987 A5e5 4b10 80fa 8754423f3ee8Document11 pagesTurn Pet1 Plastic Bottles Into 3d Filament With The Recreator 3d Mk5kit Ender3 b7936987 A5e5 4b10 80fa 8754423f3ee8Meet MehtaNo ratings yet
- Area & Perimeter - CRACK SSC PDFDocument10 pagesArea & Perimeter - CRACK SSC PDFSai Swaroop AttadaNo ratings yet
- Magnetic Properties of MaterialsDocument10 pagesMagnetic Properties of MaterialsNoviNo ratings yet
- Universal Beams PDFDocument2 pagesUniversal Beams PDFArjun S SanakanNo ratings yet
- PlayAGS, Inc.Document309 pagesPlayAGS, Inc.vicr100No ratings yet
- Aircraft Materials and Hardware: (Nuts, Studs, Screws)Document25 pagesAircraft Materials and Hardware: (Nuts, Studs, Screws)PakistaniTalent cover songsNo ratings yet
- TUV300 T4 Plus Vs TUV300 T6 Plus Vs TUV300 T8 Vs TUV300 T10 - CarWaleDocument12 pagesTUV300 T4 Plus Vs TUV300 T6 Plus Vs TUV300 T8 Vs TUV300 T10 - CarWalernbansalNo ratings yet
- Practice Career Professionalis PDFDocument29 pagesPractice Career Professionalis PDFRo Ma SantaNo ratings yet
- Retdem CathDocument17 pagesRetdem CathShane Aileen AngelesNo ratings yet
- 001-026 Labor RevDocument64 pages001-026 Labor RevDexter GasconNo ratings yet
- Arslan 20 Bba 11Document11 pagesArslan 20 Bba 11Arslan Ahmed SoomroNo ratings yet