You might also like
- Careplan Medication ListDocument17 pagesCareplan Medication ListGiorgia ScorsoneNo ratings yet
- Nursing Care Plan For Palliative Care Nursing NotesDocument2 pagesNursing Care Plan For Palliative Care Nursing NotesblaireNo ratings yet
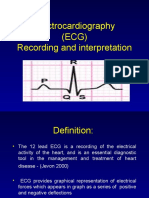
- Electrocardiography (ECG) Recording and InterpretationDocument59 pagesElectrocardiography (ECG) Recording and Interpretationkhushsandhu0% (1)
- IsoketDocument2 pagesIsoketJaessa FelicianoNo ratings yet
- IsoketDocument2 pagesIsoketJaessa Feliciano100% (1)
- Antihypertensive - ABCDDocument5 pagesAntihypertensive - ABCDTingCheung100% (1)
- In Premature Ventricular Complex, An Impulse That Starts in A Ventricle and Is Conducted Through The Ventricles Before The Next Normal SinusDocument7 pagesIn Premature Ventricular Complex, An Impulse That Starts in A Ventricle and Is Conducted Through The Ventricles Before The Next Normal SinushelloaNo ratings yet
- DR Fadillah Maricar, SPJP Angina Pectoris Dan Infark MiokardDocument50 pagesDR Fadillah Maricar, SPJP Angina Pectoris Dan Infark MiokardMuhaswadNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Planning Interventions Rationale EvaluationDocument11 pagesNursing Care Plan: Assessment Diagnosis Planning Interventions Rationale EvaluationDa NicaNo ratings yet
- Tolleno Drug Study LONGDocument9 pagesTolleno Drug Study LONGHannah TollenoNo ratings yet
- MSN Differentiate BetweenDocument17 pagesMSN Differentiate Between27-Fahima MNo ratings yet
- Drug StudyDocument7 pagesDrug StudyArnel MacabalitaoNo ratings yet
- Drug Study - Omeprazole & LosartanDocument4 pagesDrug Study - Omeprazole & LosartanCarla Tongson MaravillaNo ratings yet
- Drug Study LanoxinDocument2 pagesDrug Study LanoxinRaidis PangilinanNo ratings yet
- BHC - Drug StudyDocument3 pagesBHC - Drug Studyboxed juiceNo ratings yet
- Generic Name T Rade Name Classification Diltiazem Cardizem Antianginals, AntiarrhythmicsDocument1 pageGeneric Name T Rade Name Classification Diltiazem Cardizem Antianginals, AntiarrhythmicsChristopher LeeNo ratings yet
- Anti Hypertensive DrugsDocument40 pagesAnti Hypertensive DrugsjawadNo ratings yet
- Nursing Care PlanDocument7 pagesNursing Care PlanXy-Za Roy Marie67% (3)
- Velez College - Nursing F. Ramos ST., Cebu CityDocument26 pagesVelez College - Nursing F. Ramos ST., Cebu Cityfebie pachecoNo ratings yet
- AmlodipineDocument1 pageAmlodipineHsintan HsuNo ratings yet
- 3 Ncp'sDocument3 pages3 Ncp'sJohn Michael EstevesNo ratings yet
- Categorize The Treatment Options For Patients With Existing Medical ConditionDocument3 pagesCategorize The Treatment Options For Patients With Existing Medical ConditionMicah LatosaNo ratings yet
- Brand Name: Cardizem Generic Name: Diltiazem Drug Classification: Calcium Channel BlockersDocument2 pagesBrand Name: Cardizem Generic Name: Diltiazem Drug Classification: Calcium Channel BlockersChristine Pialan SalimbagatNo ratings yet
- Ds Week 6 Nrg301 ValenzonaDocument2 pagesDs Week 6 Nrg301 ValenzonaJoshennaNo ratings yet
- Amlodipine Drug StudyDocument1 pageAmlodipine Drug StudyaagNo ratings yet
- Amlodipine Drug StudyDocument1 pageAmlodipine Drug Studyjuan carlosNo ratings yet
- Management of Asthma Attacks in Childhood AsthmaDocument43 pagesManagement of Asthma Attacks in Childhood AsthmaGilankNo ratings yet
- Drug StudyDocument10 pagesDrug StudyKent Jerimhe Daileg ManiaulNo ratings yet
- CHF Right Side NCPDocument4 pagesCHF Right Side NCPsherlythrea22No ratings yet
- Amlodipine Drug StudyDocument2 pagesAmlodipine Drug StudyJoseph Dann Enero Jr.100% (3)
- MethergineDocument2 pagesMethergineKyla VillafrancaNo ratings yet
- Ace Inhibitors Simple NursingDocument2 pagesAce Inhibitors Simple NursingMM J30No ratings yet
- Concept Map Pleural EffusionDocument1 pageConcept Map Pleural Effusionapi-341263362No ratings yet
- College of Nursing: Brand Name: Cardizem Generic Name: Diltiazem Drug Classification: Calcium Channel BlockersDocument2 pagesCollege of Nursing: Brand Name: Cardizem Generic Name: Diltiazem Drug Classification: Calcium Channel BlockersChristine Pialan SalimbagatNo ratings yet
- Final Drug Study and Nursing Care For Cs Final Na GidDocument7 pagesFinal Drug Study and Nursing Care For Cs Final Na GidMor Shi DA BalutintikNo ratings yet
- NCP Acute PainDocument3 pagesNCP Acute PainNathalie kate petallarNo ratings yet
- CVD HypertensionDocument15 pagesCVD HypertensionAbigail BascoNo ratings yet
- ASSESMENTDocument2 pagesASSESMENTgep4617_rayNo ratings yet
- Emergency DrugsDocument16 pagesEmergency DrugsDavid Hines LopezNo ratings yet
- NCP PPHDocument2 pagesNCP PPHMark Joseph Christian100% (1)
- EKG Study GuideDocument14 pagesEKG Study GuidesydNo ratings yet
- Captopril Is An ACE Inhibitor and Works by Relaxing Blood Vessels So That Blood Can Flow More EasilyDocument4 pagesCaptopril Is An ACE Inhibitor and Works by Relaxing Blood Vessels So That Blood Can Flow More EasilyKsksksksNo ratings yet
- Assess Men 1Document2 pagesAssess Men 1Jenesis BilogNo ratings yet
- Nursing Care of HypertensionDocument14 pagesNursing Care of HypertensionRaju KaharNo ratings yet
- NCM 106 - Week 2 (Cardiovascular P1) (Midterm)Document7 pagesNCM 106 - Week 2 (Cardiovascular P1) (Midterm)MARIA KAWILANNo ratings yet
- Nursing Care PlanDocument7 pagesNursing Care Planlilac_jasminNo ratings yet
- NCP Chest PainDocument2 pagesNCP Chest PainCG Patron BamboNo ratings yet
- Physical Assessment Measurements Measurements Norms Findings Interpretation Deviation From NormalDocument30 pagesPhysical Assessment Measurements Measurements Norms Findings Interpretation Deviation From NormalAbie Jewel Joy RoqueNo ratings yet
- AntihypertensivesDocument32 pagesAntihypertensivesJianne CaloNo ratings yet
- NCP - Decreased Cardiac Output Related To Altered Heart RateDocument2 pagesNCP - Decreased Cardiac Output Related To Altered Heart RateKian Herrera100% (1)
- NCP Chest PainDocument2 pagesNCP Chest PainLinsae Troy50% (2)
- Drug Study IcuDocument6 pagesDrug Study IcuJenny Juniora AjocNo ratings yet
- Adenosine: Facial Flushing, SweatingDocument26 pagesAdenosine: Facial Flushing, SweatingAnna Sofia ReyesNo ratings yet
- Do Your Part, Care For Your HeartDocument2 pagesDo Your Part, Care For Your HeartHannah BangkilingNo ratings yet
- Pathophysiology of Heart FailureDocument2 pagesPathophysiology of Heart FailureJaysellePuguonTabijeNo ratings yet
- Amniodarone (Norvasc) Drug SummDocument1 pageAmniodarone (Norvasc) Drug SummWarrenNo ratings yet
- Drug Study: Colleen S. de La Rosa BSN IiiDocument2 pagesDrug Study: Colleen S. de La Rosa BSN IiiColleen De la RosaNo ratings yet
- NCP SGHDocument2 pagesNCP SGHdaniloabautista44No ratings yet
- Pacemaker Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPacemaker Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- The S.K.A.L.-Method: Out of the stress trap in just 64 seconds!From EverandThe S.K.A.L.-Method: Out of the stress trap in just 64 seconds!No ratings yet
- Chapter 14-Nervous System Disorders: Payton Kesselring Case Study 6Document3 pagesChapter 14-Nervous System Disorders: Payton Kesselring Case Study 6josephNo ratings yet
- Fat Embolism and Pulmonary Embolism PDFDocument1 pageFat Embolism and Pulmonary Embolism PDFSubbie OutlierNo ratings yet
- Advanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineDocument88 pagesAdvanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineRoroNo ratings yet
- 111 Cardiac Disease in PregnancyDocument7 pages111 Cardiac Disease in PregnancyAfiat WijayaNo ratings yet
- Acls MegacodeDocument8 pagesAcls Megacodes33d_destinyNo ratings yet
- PG Sedici - BookDocument240 pagesPG Sedici - BookHoàng Anh NguyễnNo ratings yet
- Acute Coronary SyndromeDocument84 pagesAcute Coronary SyndromeRinkita MallickNo ratings yet
- Tachycardia Complicated by Bradycardia Then Another Form of TachycardiaDocument7 pagesTachycardia Complicated by Bradycardia Then Another Form of TachycardiaLam Sin WingNo ratings yet
- ELECTROCARDIOGRAPHYDocument75 pagesELECTROCARDIOGRAPHYMeliaNo ratings yet
- Drug Name Mode of Action Indications Contraindications Side Effects/ Advserse Effects (Specify) Nursing InterventionsDocument4 pagesDrug Name Mode of Action Indications Contraindications Side Effects/ Advserse Effects (Specify) Nursing InterventionsKaterina Petrova100% (1)
- Hi-Yield Notes in Im & PediaDocument20 pagesHi-Yield Notes in Im & PediaJohn Christopher LucesNo ratings yet
- Week 2Document2 pagesWeek 2Elaine Marie SemillanoNo ratings yet
- Cardio Script OSCEDocument2 pagesCardio Script OSCEbarb gNo ratings yet
- Ischemic Heart DiseaseDocument8 pagesIschemic Heart DiseaseNina Natalia Bautista100% (1)
- DDD Vs VVIDocument48 pagesDDD Vs VVIGreen ButtercupNo ratings yet
- Cardiac ArrhythmiasDocument5 pagesCardiac ArrhythmiasHohl LuminitaNo ratings yet
- 2.04C Pediatric Cardiology Summary TablesDocument1 page2.04C Pediatric Cardiology Summary TablesDarnell DelgadoNo ratings yet
- Hridroga Samprapti and Modern Pathology of IhdDocument11 pagesHridroga Samprapti and Modern Pathology of IhdGAURAVNo ratings yet
- Ambulatory Elaphic MonitoDocument3 pagesAmbulatory Elaphic Monitocap tainNo ratings yet
- Causes of AneurysmsDocument11 pagesCauses of AneurysmsMathew Ace M. OmilaNo ratings yet
- AHA ACC Test Ergo Met RicoDocument56 pagesAHA ACC Test Ergo Met RicoValentina VaccaroNo ratings yet
- Unstable AnginaDocument29 pagesUnstable AnginaniaNo ratings yet
- ArrythmiaDocument81 pagesArrythmiaamalia ifanasariNo ratings yet
- Aorta Replacement and Repair Thoracic Aortic DissectionDocument3 pagesAorta Replacement and Repair Thoracic Aortic DissectionprofarmahNo ratings yet
- CHF Concept MapDocument1 pageCHF Concept MapChristy Wegner Cooper100% (4)
- 2018CV03Document22 pages2018CV03Cheng-Ting WuNo ratings yet
- EkgDocument121 pagesEkgElmir Tarani100% (1)
- JAAD CME Aug 2023 - Cutaneous Manifestations of Cardiovascular and Vascular DiseaseDocument39 pagesJAAD CME Aug 2023 - Cutaneous Manifestations of Cardiovascular and Vascular DiseasejchengwangNo ratings yet
- Diagnosis and Management in Peripheral Artery Disease EditedDocument5 pagesDiagnosis and Management in Peripheral Artery Disease Editedwahyu suparnoNo ratings yet