You might also like
- NCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!From EverandNCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!Rating: 5 out of 5 stars5/5 (4)
- Pharmacology For Nursing Care Lehne 8th Edition Test BankDocument24 pagesPharmacology For Nursing Care Lehne 8th Edition Test BankChadReillynopa100% (31)
- Test Bank For Pharmacology Clear and Simple A Guide To Drug Classifications and Dosage Calculations 3rd Edition WatkinsDocument6 pagesTest Bank For Pharmacology Clear and Simple A Guide To Drug Classifications and Dosage Calculations 3rd Edition WatkinsJean Taylor100% (39)
- Tamoxifen NolvadexDocument1 pageTamoxifen NolvadexAdrianne Bazo100% (1)
- M. Pharm Review NAPLEX 47Document1 pageM. Pharm Review NAPLEX 47JUSASBNo ratings yet
- AEMT Medication AdministrationDocument24 pagesAEMT Medication AdministrationEmily KeenNo ratings yet
- Pharmacy Exam 3Document150 pagesPharmacy Exam 3SEIYADU IBRAHIM KNo ratings yet
- Aminoglycoside Dosing GuidelinesDocument3 pagesAminoglycoside Dosing GuidelinesaeromintNo ratings yet
- Borea, P. A., Varani, K., Gessi, S., Merighi, S., & Vincenzi, F. (Eds.) - (2018) - The Adenosine Receptors PDFDocument603 pagesBorea, P. A., Varani, K., Gessi, S., Merighi, S., & Vincenzi, F. (Eds.) - (2018) - The Adenosine Receptors PDFBreiner PeñarandaNo ratings yet
- Bioptron Brochure ColorDocument43 pagesBioptron Brochure Colorvcurcubeului100% (1)
- NCM 112 Eval ExamDocument11 pagesNCM 112 Eval ExamMartin T Manuel100% (1)
- Allergic PDFDocument17 pagesAllergic PDFSiska HarapanNo ratings yet
- Drug Study HepatitisDocument7 pagesDrug Study Hepatitisjulesubayubay5428100% (1)
- Trays To Be Kept in Labour Room (As Per Goi'S MNH Toolkit)Document2 pagesTrays To Be Kept in Labour Room (As Per Goi'S MNH Toolkit)Shankar Murari100% (2)
- Dipiro 9 (012-047) PDFDocument36 pagesDipiro 9 (012-047) PDFNingrumSindayaniNo ratings yet
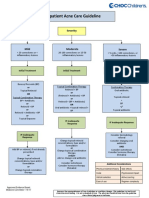
- Outpatient Acne Care Guideline: SeverityDocument5 pagesOutpatient Acne Care Guideline: SeverityMarrauNo ratings yet
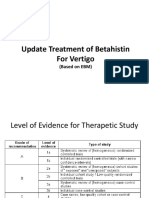
- Update Treatment of Betahistin For VertigoDocument27 pagesUpdate Treatment of Betahistin For VertigoPanggah AnanditaNo ratings yet
- JR 3 Dr. Danisa Edit - Efficacy and Safety of 250 MG Versus 500 MG Oral Terbinafine in The TreatmeDocument13 pagesJR 3 Dr. Danisa Edit - Efficacy and Safety of 250 MG Versus 500 MG Oral Terbinafine in The Treatmedanisa.dvjuli23No ratings yet
- Top 10 Perlas Clã Nicas en Acne Dermatologic Clinics 2015Document11 pagesTop 10 Perlas Clã Nicas en Acne Dermatologic Clinics 2015Yulay HBNo ratings yet
- Pillar ComparisonDocument1 pagePillar ComparisonSatya PNo ratings yet
- Management of Asthma: Dr. Md. Khairul Hassan JessyDocument42 pagesManagement of Asthma: Dr. Md. Khairul Hassan JessyDr. NasrumminallahNo ratings yet
- Menieres Disease 1Document66 pagesMenieres Disease 1Kevin DareNo ratings yet
- Wiser Choice of Antibiotic From Bench To Bedside and Back Again - Sri Rezeki HadinegoroDocument35 pagesWiser Choice of Antibiotic From Bench To Bedside and Back Again - Sri Rezeki HadinegoroIfah Inayah D'zatrichaNo ratings yet
- PARGAD - CON1A - Module 11 Assignment (Endocrine Drugs and Diabetes Mellitus Drugs)Document9 pagesPARGAD - CON1A - Module 11 Assignment (Endocrine Drugs and Diabetes Mellitus Drugs)Samantha PargadNo ratings yet
- A Case Report of Acne Vulgaris Treated by Combination of Acupuncture 2155 9570 1000446Document2 pagesA Case Report of Acne Vulgaris Treated by Combination of Acupuncture 2155 9570 1000446Ran NisNo ratings yet
- CAP AlgorithmDocument1 pageCAP AlgorithmdamondouglasNo ratings yet
- Management of Asthma: Dr. Md. Khairul Hassan JessyDocument42 pagesManagement of Asthma: Dr. Md. Khairul Hassan JessyWafaa AbdullahNo ratings yet
- Ch34 PharmDocument8 pagesCh34 PharmShaneka WilliamsNo ratings yet
- Psoriasis AlgorithmDocument1 pagePsoriasis AlgorithmSeun MosesNo ratings yet
- Stroke Physician: Clinical Decision FormDocument6 pagesStroke Physician: Clinical Decision FormBaiq PritaNo ratings yet
- Drug Nam1Document3 pagesDrug Nam1deewagsabadoNo ratings yet
- Adverse Drug Reaction: BY Dr.G.Aarthipriyanka Post Graduate Department of PharmacologyDocument19 pagesAdverse Drug Reaction: BY Dr.G.Aarthipriyanka Post Graduate Department of PharmacologyArya BTSNo ratings yet
- CH 008 Enteric Fever PDFDocument7 pagesCH 008 Enteric Fever PDFVibojaxNo ratings yet
- OmeprazoleDocument2 pagesOmeprazoleIvan Matthew SuperioNo ratings yet
- Journal DermatologyDocument4 pagesJournal DermatologyKoas PatoNo ratings yet
- Pharma 2018 PDFDocument29 pagesPharma 2018 PDFriczen vilaNo ratings yet
- CEM4681 CEC Guideline For The Management of Pain in Adults June 2010 Rev1Document7 pagesCEM4681 CEC Guideline For The Management of Pain in Adults June 2010 Rev1arijitkgNo ratings yet
- Oncology Supportive Care Update BCPS 2021-1Document106 pagesOncology Supportive Care Update BCPS 2021-1Mr.ShazNo ratings yet
- Antimicrobial Stewardship Clinical Pathways For Management of CommonDocument11 pagesAntimicrobial Stewardship Clinical Pathways For Management of CommonYusran YusoffNo ratings yet
- SteroidDocument26 pagesSteroidzhakaNo ratings yet
- Ampisul, Hydrocort, Salbu, Mupirocin DrugsDocument4 pagesAmpisul, Hydrocort, Salbu, Mupirocin DrugsClarissa GuifayaNo ratings yet
- PTO Infeksi WidyDocument28 pagesPTO Infeksi WidyNurhasna Sushmita SariNo ratings yet
- Pre Clinical Prep 2Document8 pagesPre Clinical Prep 2Laura MastantuonoNo ratings yet
- CSS-Diet For EczemaDocument32 pagesCSS-Diet For Eczemaariella krisnandaNo ratings yet
- GL PresentationDocument29 pagesGL Presentationapi-586369243No ratings yet
- Chapter 34. Pain Management, Self-Assessment QuestionsDocument7 pagesChapter 34. Pain Management, Self-Assessment Questionstsegaab yosephNo ratings yet
- Protocol 010Document12 pagesProtocol 010hatem newishyNo ratings yet
- Anaesthetics & Pain ManagementDocument155 pagesAnaesthetics & Pain ManagementUmair ShafqatNo ratings yet
- Prometric NotesDocument4 pagesPrometric NotesPharma Tech AcademyNo ratings yet
- Hydrocortisone (Final)Document11 pagesHydrocortisone (Final)Zyla KrisshaNo ratings yet
- Terapi Akne Ciproterone Acetate Oleh Dr. Abraham Arimuko SPKK Mars Finsdv FaadvDocument32 pagesTerapi Akne Ciproterone Acetate Oleh Dr. Abraham Arimuko SPKK Mars Finsdv FaadvshabrinaerinNo ratings yet
- CA PretestDocument37 pagesCA PretestJoanna TaylanNo ratings yet
- ImmunosuppressantsDocument7 pagesImmunosuppressantsYaser ZaherNo ratings yet
- Antibiotik IV Ke PODocument3 pagesAntibiotik IV Ke POFarmasi RSUD Kramat JatiNo ratings yet
- Nausea, VomitingDocument8 pagesNausea, VomitingEmily Hon (Emalai)No ratings yet
- Dyslipidemia Guide AlnajahDocument47 pagesDyslipidemia Guide Alnajahsafwan fayyadNo ratings yet
- Intravenous To Oral ConversionDocument6 pagesIntravenous To Oral ConversiondoodrillNo ratings yet
- IV To PO Conversion PolicyDocument4 pagesIV To PO Conversion PolicyIrham NiNo ratings yet
- Breast Cancer LowDocument30 pagesBreast Cancer LowlagundaNo ratings yet
- Analysis of Clinical Efficacy, Sideeffects, and Laboratory Changesamong Patients With Acnevulgaris Receiving Single Versustwice Daily Dose Oforal IsotretinoinDocument7 pagesAnalysis of Clinical Efficacy, Sideeffects, and Laboratory Changesamong Patients With Acnevulgaris Receiving Single Versustwice Daily Dose Oforal IsotretinoinKadir KUCUKNo ratings yet
- Antiemetic Drug Use in Children What The.3Document6 pagesAntiemetic Drug Use in Children What The.3Zafitri AsrulNo ratings yet
- Guidelines For The Management of Psoriasis in Primary Care v12Document6 pagesGuidelines For The Management of Psoriasis in Primary Care v12ShamlazaghNo ratings yet
- Nursing Exam Questions 2023 Part 3Document6 pagesNursing Exam Questions 2023 Part 3Lejo SunnyNo ratings yet
- Drug Study Cushing DiseaseDocument8 pagesDrug Study Cushing DiseaseRachel QuionNo ratings yet
- Pain in Pediatric: Nur Surya WirawanDocument27 pagesPain in Pediatric: Nur Surya WirawanaswalbasukiNo ratings yet
- AM DrugsDocument17 pagesAM Drugsstella.gillesania.chenNo ratings yet
- Clinical Pharmacy Roger Walker Clinical Pharmacy and Therapeutics 5th EdDocument14 pagesClinical Pharmacy Roger Walker Clinical Pharmacy and Therapeutics 5th Edstella.gillesania.chenNo ratings yet
- Clinical Pharmacy and Therapeutics by Cate Whittlesea and Karen HodsonDocument15 pagesClinical Pharmacy and Therapeutics by Cate Whittlesea and Karen Hodsonstella.gillesania.chenNo ratings yet
- F4) P-Rheumatoid ArthritisDocument11 pagesF4) P-Rheumatoid Arthritisstella.gillesania.chenNo ratings yet
- Pharmacotherapy Handbook - ALLERGIC RHINITISDocument8 pagesPharmacotherapy Handbook - ALLERGIC RHINITISstella.gillesania.chenNo ratings yet
- Drug StudyDocument7 pagesDrug StudyCarson BirthNo ratings yet
- Swertia Chirayita - An Overview: P. Joshi and V. DhawanDocument6 pagesSwertia Chirayita - An Overview: P. Joshi and V. DhawanLalit Jung RanaNo ratings yet
- Sistem Perkemihan: Indargairi Universitas Mega RezkyDocument46 pagesSistem Perkemihan: Indargairi Universitas Mega RezkyMaria GabrielaNo ratings yet
- Ajtcam V10i4 26Document10 pagesAjtcam V10i4 26RiscoriaNo ratings yet
- Drug Study BenadrylDocument2 pagesDrug Study BenadrylJohn Karl Garcia RazalanNo ratings yet
- Study Design: Condition or Disease Intervention/treatmentDocument36 pagesStudy Design: Condition or Disease Intervention/treatmentMihu DragostinNo ratings yet
- British J Pharmacology - 2021 - ZobdehDocument20 pagesBritish J Pharmacology - 2021 - ZobdehRenju KuriakoseNo ratings yet
- Zantac (Ranitidine) - Safety Information - NDMA Found in Samples of Some Ranitidine Medicines - FDADocument2 pagesZantac (Ranitidine) - Safety Information - NDMA Found in Samples of Some Ranitidine Medicines - FDACuam CaracasNo ratings yet
- Pharma Cardio Respi and Repro NclexdocxDocument8 pagesPharma Cardio Respi and Repro NclexdocxJhayneNo ratings yet
- Product NDC # Compare To Strength Size Form Case Pack Abcoe# Cardinal Cin # Mckesson Oe # M&Doe#Document14 pagesProduct NDC # Compare To Strength Size Form Case Pack Abcoe# Cardinal Cin # Mckesson Oe # M&Doe#Paras ShardaNo ratings yet
- Neurologic Complications in Diabetes Mellitus: Done By-Fatema Burhan Ravat Dtmu 4Th Year January 2020Document27 pagesNeurologic Complications in Diabetes Mellitus: Done By-Fatema Burhan Ravat Dtmu 4Th Year January 2020Fatema RavatNo ratings yet
- Stok Per TGL 28 Mei 2022Document93 pagesStok Per TGL 28 Mei 2022Bambang hendrawanNo ratings yet
- 15 Patients With Altered VentilationDocument66 pages15 Patients With Altered VentilationErshelle Mae MorlaNo ratings yet
- Maco CaliculationDocument5 pagesMaco CaliculationkevinNo ratings yet
- Endorsement Week 9Document13 pagesEndorsement Week 9MICHELLE FACTONo ratings yet
- ContinueDocument2 pagesContinuesamsonNo ratings yet
- Absorption and Half-Life: Nick Holford Dept Pharmacology & Clinical Pharmacology University of Auckland, New ZealandDocument7 pagesAbsorption and Half-Life: Nick Holford Dept Pharmacology & Clinical Pharmacology University of Auckland, New ZealandkbnarkhedeNo ratings yet
- Ecstatic (NSFW) - Exceed and LeadDocument5 pagesEcstatic (NSFW) - Exceed and LeadVal KerryNo ratings yet
- Adr Enaline (Epinephrine) 1mg/ml (1:1000) : Paediatric Cardiac Arrest AlgorhytmDocument13 pagesAdr Enaline (Epinephrine) 1mg/ml (1:1000) : Paediatric Cardiac Arrest AlgorhytmwawaNo ratings yet
- Comparative Study of A Low-Dose With Standard Dose Propofol in Electroconvulsive Therapy (ECT) in Federal Neuropsychiatric Hospital, KadunaDocument5 pagesComparative Study of A Low-Dose With Standard Dose Propofol in Electroconvulsive Therapy (ECT) in Federal Neuropsychiatric Hospital, KadunaAdeyemi OlusolaNo ratings yet
- Clinical Pharmacy PINK PACOPDocument3 pagesClinical Pharmacy PINK PACOPEunice SofiaNo ratings yet
- Usmle Pharmacology RecallDocument496 pagesUsmle Pharmacology Recalllorre316100% (9)
- Clinical Pharma 3 فودةDocument210 pagesClinical Pharma 3 فودةRebwarNo ratings yet
- Saeed Book Bank: Leading Importers, Exporter, Distributors, Booksellers & Publishers of PakistanDocument15 pagesSaeed Book Bank: Leading Importers, Exporter, Distributors, Booksellers & Publishers of Pakistantalisella50% (2)