You might also like
- Cline y Angier (2010) - The Arvon Book of Life Writing. Writing Biography, Autobiography and MemoirDocument289 pagesCline y Angier (2010) - The Arvon Book of Life Writing. Writing Biography, Autobiography and MemoirConstanza Arraño100% (5)
- The Ultimate Guide to Physician Associate OSCEs: Written by a Physician Associate for Physician AssociatesFrom EverandThe Ultimate Guide to Physician Associate OSCEs: Written by a Physician Associate for Physician AssociatesNo ratings yet
- Format Pre EmploymentDocument10 pagesFormat Pre EmploymentNurman HidayatNo ratings yet
- Medical ReportDocument5 pagesMedical ReportMZALENDO.NETNo ratings yet
- Metal Gear Solid - Characters Profile and TimelineDocument65 pagesMetal Gear Solid - Characters Profile and Timelinekrevorkian1653100% (1)
- Pre Medical Evaluatiom Form PFT 1 PDFDocument2 pagesPre Medical Evaluatiom Form PFT 1 PDFAIEN WENDELEIH Q. CAPINPIN100% (2)
- Medical Examination: Subang Polyclinic SDN BHDDocument5 pagesMedical Examination: Subang Polyclinic SDN BHDSubang polylinicNo ratings yet
- Medical Evaluation Form 2022Document2 pagesMedical Evaluation Form 2022jimmy p. lamhi50% (2)
- Health HistoryDocument19 pagesHealth HistoryAngelene Caliva100% (1)
- PSM Case ProformaDocument28 pagesPSM Case ProformaSathish100% (1)
- Ralph Alan Dale 1972 Hypnotism and EducationDocument21 pagesRalph Alan Dale 1972 Hypnotism and EducationFrancis Gladstone-Quintuplet100% (2)
- Outpatient Consultation: Rural Health UnitDocument25 pagesOutpatient Consultation: Rural Health UnitAntonio RegasaNo ratings yet
- Week 1: Item PointsDocument112 pagesWeek 1: Item PointsAngel Lynn YlayaNo ratings yet
- Medical Report FormDocument7 pagesMedical Report FormShazni Afandi RusliNo ratings yet
- Medical Certificate 2Document2 pagesMedical Certificate 2Aditeya Shukla100% (1)
- Medical ReportDocument5 pagesMedical ReportShoaib Mirza0% (1)
- Optional Module 5 - Quality of Life 050713Document5 pagesOptional Module 5 - Quality of Life 050713Saputri AnggiNo ratings yet
- Admission Audit ToolDocument3 pagesAdmission Audit ToolDewi Ratna SariNo ratings yet
- LymphomaDocument20 pagesLymphomaChairul Adilla Ardy100% (1)
- Community Medicine Osce ReviewersDocument2 pagesCommunity Medicine Osce ReviewersJoy FucananNo ratings yet
- Supportive Supervision Checklist For AFHCDocument5 pagesSupportive Supervision Checklist For AFHCDr. Ankur SangwanNo ratings yet
- GIDA Community Profile 04 May 2015Document7 pagesGIDA Community Profile 04 May 2015SamNo ratings yet
- Health Booklet 2014Document68 pagesHealth Booklet 2014Tan KMNo ratings yet
- Pimento ResearchDocument6 pagesPimento ResearchgashugipackoNo ratings yet
- Appendix A - FDocument54 pagesAppendix A - Fbakson college gr. noidaNo ratings yet
- Adult Health Status Summary: Page 1 of 3Document3 pagesAdult Health Status Summary: Page 1 of 3safasayedNo ratings yet
- WCM Medical FormDocument4 pagesWCM Medical Formjewel_meltonNo ratings yet
- G4S Churchill: Work Health Assessment Form For Employees With Patient or Body Fluid ContactDocument5 pagesG4S Churchill: Work Health Assessment Form For Employees With Patient or Body Fluid ContactAugusto Dos Santos De JesusNo ratings yet
- Nursing Assessment Template 11Document48 pagesNursing Assessment Template 11metrohealth shankarappasNo ratings yet
- Envelope - Medical Application Form - New - V3 - Mednet - 1Document3 pagesEnvelope - Medical Application Form - New - V3 - Mednet - 1muhdm7771No ratings yet
- Survey July To September 3Document4 pagesSurvey July To September 3Harry PoterNo ratings yet
- Florida School Entry Health ExamDocument2 pagesFlorida School Entry Health ExamPeterBurkeNo ratings yet
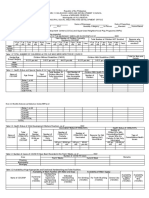
- Form 1.1 (Temporary) Monthly Outcome & Indicators - Center LevelDocument6 pagesForm 1.1 (Temporary) Monthly Outcome & Indicators - Center Levelmariegold mortola fabelaNo ratings yet
- Health DeclarationDocument5 pagesHealth Declarationust dol100% (1)
- Gordon'S Functional Health PatternDocument8 pagesGordon'S Functional Health PatternChill Jayson MarcaidaNo ratings yet
- State: District: Block: City/ Town/ Village: Facility Name: Due For Submission On 5th of Following MonthDocument5 pagesState: District: Block: City/ Town/ Village: Facility Name: Due For Submission On 5th of Following MonthDipanwita DasNo ratings yet
- Social Support in DiabetesDocument40 pagesSocial Support in DiabetesWajiha ArshadNo ratings yet
- Gordon'S Functional Health PatternDocument10 pagesGordon'S Functional Health PatternNurr AndigNo ratings yet
- 11 Functional Gordon Health Pattern QuestionsDocument5 pages11 Functional Gordon Health Pattern QuestionsShaina MillanNo ratings yet
- Health Booklet 2014Document68 pagesHealth Booklet 2014QwesxzNo ratings yet
- VHND Field Form Cum Check List Rev 01Document3 pagesVHND Field Form Cum Check List Rev 01nishantojha0% (1)
- Patient Survey QuestionnaireDocument3 pagesPatient Survey QuestionnaireVivek DasNo ratings yet
- Medical Application Form (New) - V3-2021!10!12 - RAKDocument3 pagesMedical Application Form (New) - V3-2021!10!12 - RAKAnkita NiravNo ratings yet
- Checklist For HP Revised Health Promotion &DPDocument13 pagesChecklist For HP Revised Health Promotion &DPAbdiresak AbdusemedNo ratings yet
- Health AsssDocument2 pagesHealth AsssLLORITO Cristell Joy M.No ratings yet
- Clinic Services Presentation-CheDocument10 pagesClinic Services Presentation-CheChe BecerilNo ratings yet
- The Updated, Adapted&modified QuestionnaireDocument8 pagesThe Updated, Adapted&modified Questionnairesamson felekeNo ratings yet
- Adult Full Assessment With MSEDocument7 pagesAdult Full Assessment With MSEmary grace bialenNo ratings yet
- My Community Healthcare SurveyDocument8 pagesMy Community Healthcare SurveyJohn Patrick Valera100% (2)
- Brendahs Medical FormDocument2 pagesBrendahs Medical FormBaluku GeofreyNo ratings yet
- Area /village: Name Number: .... Health Center: Name .......................... Number: ..... DateDocument8 pagesArea /village: Name Number: .... Health Center: Name .......................... Number: ..... DateMuna Hassan MustafaNo ratings yet
- WWW - Csc.gov - PH: Additional RequirementsDocument4 pagesWWW - Csc.gov - PH: Additional RequirementsMaria JessaNo ratings yet
- Antepartum-Haemorrhage APHDocument9 pagesAntepartum-Haemorrhage APHAjoy DasNo ratings yet
- Community Unit AWP Planning Template - 5.9.18 yDocument17 pagesCommunity Unit AWP Planning Template - 5.9.18 yNEVIAN SHANTEL100% (1)
- HDFC MerDocument3 pagesHDFC Merseenasrinivas113No ratings yet
- BwergnwoienbDocument3 pagesBwergnwoienbpobayed154No ratings yet
- School Medical Examination FormDocument2 pagesSchool Medical Examination FormElite Mission HospitalNo ratings yet
- Groups ABCD - Family Medicine End Block QuestionsDocument10 pagesGroups ABCD - Family Medicine End Block QuestionsHisham ChomanyNo ratings yet
- Health Action PlanDocument20 pagesHealth Action PlanCielito GumbanNo ratings yet
- For ME Plan Indicator Tracking Template - GK MI Proejct - Updated - On - 5thjan21Document55 pagesFor ME Plan Indicator Tracking Template - GK MI Proejct - Updated - On - 5thjan21sammam mahdi samiNo ratings yet
- Report Writting of Kailali VDCDocument69 pagesReport Writting of Kailali VDCGaurav Bohara100% (1)
- Health Assessment FormDocument2 pagesHealth Assessment Formshiela manalaysayNo ratings yet
- Sample Filled in MRDocument10 pagesSample Filled in MRAnn Bernadeth NavelinoNo ratings yet
- Mental Health Issues In Health Professionals : How to Improve and Balance Your Mental Health with Work and Life in the Health FieldFrom EverandMental Health Issues In Health Professionals : How to Improve and Balance Your Mental Health with Work and Life in the Health FieldNo ratings yet
- "L8" Drive End: Operation - Assembly Instructions and Parts List ForDocument7 pages"L8" Drive End: Operation - Assembly Instructions and Parts List ForACCA PumpsNo ratings yet
- Purification of Wastewater by Metal Oxide NanoparticlesDocument12 pagesPurification of Wastewater by Metal Oxide NanoparticlesEditor IJTSRDNo ratings yet
- Percakapan BHS Inggris Penerimaan PasienDocument5 pagesPercakapan BHS Inggris Penerimaan PasienYulia WyazztNo ratings yet
- The Enemy Within - v18Document8 pagesThe Enemy Within - v18Matt WillisNo ratings yet
- Pms 500 - International Mechanics KitDocument0 pagesPms 500 - International Mechanics KitArsul RNo ratings yet
- SDS - Molykote 1000Document8 pagesSDS - Molykote 1000Zarni KyawNo ratings yet
- Civic Ass JolaxDocument3 pagesCivic Ass JolaxEyob TeferaNo ratings yet
- HECKMAN, J. James - Schools, Skills and SynapsesDocument36 pagesHECKMAN, J. James - Schools, Skills and SynapsesAndré Gonçalves OliveiraNo ratings yet
- 1 Man Is The Crowning Glory of God's CreationDocument12 pages1 Man Is The Crowning Glory of God's CreationCaptainBreezy YeezyNo ratings yet
- Dr. Shikha Baskar: CHE154: Physical Chemistry For HonorsDocument22 pagesDr. Shikha Baskar: CHE154: Physical Chemistry For HonorsnishitsushantNo ratings yet
- BDU-BIT-Electromechanical Engineering Curriculum (Regular Program)Document187 pagesBDU-BIT-Electromechanical Engineering Curriculum (Regular Program)beselamu75% (4)
- Geometry Sparkcharts Geometry Sparkcharts: Book Review Book ReviewDocument3 pagesGeometry Sparkcharts Geometry Sparkcharts: Book Review Book ReviewAyman BantuasNo ratings yet
- What Is A CodebookDocument5 pagesWhat Is A CodebookAxmed YaasiinNo ratings yet
- RNR150 Syllabus1Document14 pagesRNR150 Syllabus1Shaun SarvisNo ratings yet
- 300 Top Fluid Mechanics Multiple Choice Questions With Answers PDFDocument20 pages300 Top Fluid Mechanics Multiple Choice Questions With Answers PDFpiluNo ratings yet
- Formula and Functions in MS ExcelDocument9 pagesFormula and Functions in MS ExcelBhavana SangamNo ratings yet
- Councillor Danny Thorpe: Leader, Royal Borough of GreenwichDocument2 pagesCouncillor Danny Thorpe: Leader, Royal Borough of GreenwichDr-Syed Ali TarekNo ratings yet
- Novena To Our Lady Queen of PeaceDocument4 pagesNovena To Our Lady Queen of PeaceGraciedion MediaNo ratings yet
- Artificial RainfallDocument20 pagesArtificial Rainfallsurajsingh100% (3)
- Ebook PDF Understanding Nutrition 2th by Eleanor Whitney PDFDocument41 pagesEbook PDF Understanding Nutrition 2th by Eleanor Whitney PDFedward.howard102100% (31)
- Public Value and Art For All?Document20 pagesPublic Value and Art For All?yolandaniguasNo ratings yet
- FCo Research Report Debit Card and Bitcoin in MenaDocument10 pagesFCo Research Report Debit Card and Bitcoin in MenaJhimy JeanNo ratings yet
- Proposal Project PrintingDocument13 pagesProposal Project PrintinglodewNo ratings yet
- ReportDocument1 pageReportyousufNo ratings yet
- TranscriptDocument1 pageTranscriptGursharanjit SinghNo ratings yet
- Activity Sheets Q1 - SVADocument5 pagesActivity Sheets Q1 - SVAAlma ReynaldoNo ratings yet