You might also like
- Oxford Textbook of Medicine, 5th EdDocument101 pagesOxford Textbook of Medicine, 5th EdIzni Zinin75% (4)
- كل أسئلة اللثة لامتحان الهيئةDocument40 pagesكل أسئلة اللثة لامتحان الهيئةMohamed Kudaih100% (1)
- Jakobiec 039 S Principles Amp Practice of Ophthalmology Volume OneDocument1,638 pagesJakobiec 039 S Principles Amp Practice of Ophthalmology Volume OneAndi Meidin Anugerah75% (4)
- Alberts Principles and Practice of Ophthalmology - Volume I PDFDocument1,638 pagesAlberts Principles and Practice of Ophthalmology - Volume I PDFJorge Flores100% (2)
- Laminates and VeneersDocument125 pagesLaminates and VeneersSURBHI MEHDIRATTA100% (1)
- FasciaResearchBook ExcerptDocument31 pagesFasciaResearchBook ExcerptPedro FonsecaNo ratings yet
- Comprehensive Manuals in Radiology: Harold G. Jacobson, EditorDocument140 pagesComprehensive Manuals in Radiology: Harold G. Jacobson, Editorsimona mariana dutuNo ratings yet
- Cleft Lip & PalateDocument13 pagesCleft Lip & PalateMahsaNo ratings yet
- NBDHE Board Review 2013 Oral Pathology Flashcards - QuizletDocument15 pagesNBDHE Board Review 2013 Oral Pathology Flashcards - QuizletDENTAL REVIEWER ONLY100% (1)
- Alberts Principles and Practice of Ophthalmology - Volume II PDFDocument1,373 pagesAlberts Principles and Practice of Ophthalmology - Volume II PDFPrep Neet PG100% (3)
- Congenital Dysplasia & DislocatiDocument558 pagesCongenital Dysplasia & DislocatiWilson A. QuinteroNo ratings yet
- Tracy Batchelor, Ryo Nishikawa, Nancy Tarbell, Michael Weller - Oxford Textbook of Neuro-Oncology-Oxford University Press (2017)Document269 pagesTracy Batchelor, Ryo Nishikawa, Nancy Tarbell, Michael Weller - Oxford Textbook of Neuro-Oncology-Oxford University Press (2017)gaanbazar100% (1)
- @MedicalBooksStore 2017 Osteoporosis PDFDocument501 pages@MedicalBooksStore 2017 Osteoporosis PDFHeri Gunawan100% (1)
- TRUMPET 6-MPPA - Dec2016 - Wold20161011Document13 pagesTRUMPET 6-MPPA - Dec2016 - Wold20161011Percy Stanbury Malaga100% (1)
- 1 4954122304943554897Document445 pages1 4954122304943554897Hady SpinNo ratings yet
- Treatment of Angular Cheilitis A Narrative Review and AuthorsDocument9 pagesTreatment of Angular Cheilitis A Narrative Review and AuthorsElizabeth SihiteNo ratings yet
- A Guide To Writing Case Reports For The Journal ofDocument9 pagesA Guide To Writing Case Reports For The Journal ofSiLfia SahrinNo ratings yet
- Meta Analise?Document4 pagesMeta Analise?AllyssonNo ratings yet
- The Dental Anomaly: How and Why Dental Caries and Periodontitis Are Phenomenologically AtypicalDocument7 pagesThe Dental Anomaly: How and Why Dental Caries and Periodontitis Are Phenomenologically AtypicalNicolle DonayreNo ratings yet
- STAB-A Response To The Commentary Questions On TheDocument3 pagesSTAB-A Response To The Commentary Questions On Thesolodont1No ratings yet
- Research and Publication Ethics: What Have We Learned Thus Far?Document3 pagesResearch and Publication Ethics: What Have We Learned Thus Far?Jose ContrerasNo ratings yet
- Review of Oncology Oxford Core Text 2edition by MaDocument2 pagesReview of Oncology Oxford Core Text 2edition by MaAksha PraiselinNo ratings yet
- (1979) Genetic Diseases of The SkinDocument352 pages(1979) Genetic Diseases of The SkinfauzNo ratings yet
- Osteoarthritis Year in Review 2019 Epidemiology AnDocument8 pagesOsteoarthritis Year in Review 2019 Epidemiology AnWALKING MORE STORE IDNo ratings yet
- tmpBE69 TMPDocument2 pagestmpBE69 TMPFrontiersNo ratings yet
- 1996 - A - Field - Guide - To - Joint - Disease - in - ArchaeologyDocument3 pages1996 - A - Field - Guide - To - Joint - Disease - in - ArchaeologyAlejandro LealNo ratings yet
- 2015 - Swanson - How To Practice Evidence-Based MedicineDocument14 pages2015 - Swanson - How To Practice Evidence-Based MedicineAudrey VivierNo ratings yet
- Contemporary Orthodontics, 5th EditionDocument2 pagesContemporary Orthodontics, 5th EditionAasharAshrafNo ratings yet
- Orthodontics PDFDocument2 pagesOrthodontics PDFNurul Andika Virginia PutriNo ratings yet
- Apsm 2017 17 4 (1) 54Document3 pagesApsm 2017 17 4 (1) 54bose_lowe11No ratings yet
- BIFOSFONATOSDocument9 pagesBIFOSFONATOSClaudia Lizeth Ibarra DomínguezNo ratings yet
- Who Classification An AppraisalDocument10 pagesWho Classification An AppraisalKhánh VũNo ratings yet
- JVRJDocument2 pagesJVRJRMGNo ratings yet
- Oem 15 2 135-ADocument3 pagesOem 15 2 135-Agasai gasaiNo ratings yet
- Animals and The Shaping of Modern Medicine One Health and Its Histories 1St Edition Abigail Woods Full ChapterDocument67 pagesAnimals and The Shaping of Modern Medicine One Health and Its Histories 1St Edition Abigail Woods Full Chaptermatthew.grasso983100% (2)
- Califmed00247 0078aDocument1 pageCalifmed00247 0078aAndi AdeNo ratings yet
- The Clinical Case Report: A Review of Its Merits and LimitationsDocument8 pagesThe Clinical Case Report: A Review of Its Merits and LimitationsLinh HươngNo ratings yet
- Free Download Oxford Handbook of Rheumatology 4E True 4Th Edition Edition Gavin Clunie Full Chapter PDFDocument51 pagesFree Download Oxford Handbook of Rheumatology 4E True 4Th Edition Edition Gavin Clunie Full Chapter PDFlawrence.hendrix951100% (16)
- Oxford Handbook of Rheumatology 4E True 4Th Edition Edition Gavin Clunie Full ChapterDocument67 pagesOxford Handbook of Rheumatology 4E True 4Th Edition Edition Gavin Clunie Full Chapterbernice.padilla474No ratings yet
- Documentm 9373Document51 pagesDocumentm 9373priscilla.villegas794No ratings yet
- Orthopaedic Management in Cerebral PalsyDocument3 pagesOrthopaedic Management in Cerebral PalsyUsuario de CrackNo ratings yet
- 596 1 FullDocument1 page596 1 FullIshfaq LoneNo ratings yet
- Journal Reading 1Document16 pagesJournal Reading 1Rizky Amalia SaputriNo ratings yet
- Oxford Textbook of Medical Mycology Oxford Textbooks in Infectious Disease and Microbiology 1St Edition Christopher C Kibbler Editor Full ChapterDocument68 pagesOxford Textbook of Medical Mycology Oxford Textbooks in Infectious Disease and Microbiology 1St Edition Christopher C Kibbler Editor Full Chaptervirginia.cunningham147100% (4)
- l56249 Copy 151228151622Document8 pagesl56249 Copy 151228151622Naliana LupascuNo ratings yet
- The Neurologist's Dilemma: A Comprehensive Clinical Review of Bell's Palsy, With Emphasis On Current Management TrendsDocument10 pagesThe Neurologist's Dilemma: A Comprehensive Clinical Review of Bell's Palsy, With Emphasis On Current Management TrendsMuhamad BenyaminNo ratings yet
- The Evidence-Based Health Care Debate - 2006. Where Are We Now ?Document9 pagesThe Evidence-Based Health Care Debate - 2006. Where Are We Now ?Andre LanzerNo ratings yet
- 173 Asynopsisofthehistoryof HansensdiseaseDocument5 pages173 Asynopsisofthehistoryof HansensdiseaseNinel López VillarrealNo ratings yet
- Vascular Surgery: Cases, Questions and CommentariesFrom EverandVascular Surgery: Cases, Questions and CommentariesGeorge GeroulakosNo ratings yet
- Australian Dental Journal - 2017 - Pedrosa - Oral Manifestations Related To Dengue Fever A Systematic Review of TheDocument8 pagesAustralian Dental Journal - 2017 - Pedrosa - Oral Manifestations Related To Dengue Fever A Systematic Review of TheYunita Permata Dewi NNo ratings yet
- GenreanalysisdraftDocument7 pagesGenreanalysisdraftapi-284913073No ratings yet
- Centric Relation From Red Giant To White DwarfDocument3 pagesCentric Relation From Red Giant To White DwarfjoaompradoNo ratings yet
- Brjgenprac00016 0058bDocument2 pagesBrjgenprac00016 0058bM EhabNo ratings yet
- Cholesteatoma Definition and Classification: A Literature ReviewDocument6 pagesCholesteatoma Definition and Classification: A Literature ReviewRamizFadhlillahNo ratings yet
- 6-MPPA Dec2016 Wold20161011Document13 pages6-MPPA Dec2016 Wold20161011André QianNo ratings yet
- Ijerph 19 08234 - KustaDocument14 pagesIjerph 19 08234 - KustaMeiyanti MeiyantiNo ratings yet
- 173 Asynopsisofthehistoryof HansensdiseaseDocument5 pages173 Asynopsisofthehistoryof HansensdiseaseThiago RavanelliNo ratings yet
- Centric Relation From Red Giant To White DwarfDocument3 pagesCentric Relation From Red Giant To White DwarfManuel CastilloNo ratings yet
- Structural and Chemical Organization of TeethFrom EverandStructural and Chemical Organization of TeethA MillsNo ratings yet
- Curroncol 29 00552 v3Document30 pagesCurroncol 29 00552 v3Arun AdhikariNo ratings yet
- Physician'S: Rhodes, (Edin.), Director, Hygiene, VirologistDocument1 pagePhysician'S: Rhodes, (Edin.), Director, Hygiene, VirologistLucas BauerNo ratings yet
- Tooth Brush ....... RochiraDocument11 pagesTooth Brush ....... RochiraSanjana RawatNo ratings yet
- Dentosphere World of Dentistry MCQs in Prosthodontics - Major and Minor Connectors - Removable Partial Dentures 3Document1 pageDentosphere World of Dentistry MCQs in Prosthodontics - Major and Minor Connectors - Removable Partial Dentures 3Assssss100% (2)
- FasesTratamento LuísNunezDocument16 pagesFasesTratamento LuísNunezCatia Sofia A PNo ratings yet
- Ornithischian Dinosaurs in Southeast Asia: A Review With Palaeobiogeographic ImplicationsDocument25 pagesOrnithischian Dinosaurs in Southeast Asia: A Review With Palaeobiogeographic ImplicationsJe suis un MicaschisteNo ratings yet
- Download pdf Fundamentals Of Orthognathic Surgery And Non Surgical Facial Aesthetics Third Edition Malcolm Harris Editor ebook full chapterDocument53 pagesDownload pdf Fundamentals Of Orthognathic Surgery And Non Surgical Facial Aesthetics Third Edition Malcolm Harris Editor ebook full chapterouida.hastings911100% (1)
- Principles of RG InterpretationDocument61 pagesPrinciples of RG InterpretationVeda samhithaNo ratings yet
- Curriculum Vitae: Personal IdentytyDocument6 pagesCurriculum Vitae: Personal IdentytyFirmansyah RizkyNo ratings yet
- 2 1 Anterior AnswerDocument10 pages2 1 Anterior AnswerOla AliNo ratings yet
- EPP Infodump VersionDocument16 pagesEPP Infodump Versionearthalla yaNo ratings yet
- Deep-Bite Fontaine-Sylvestre - CatherineDocument126 pagesDeep-Bite Fontaine-Sylvestre - CatherineEttore AccivileNo ratings yet
- July 6, 2018 Strathmore TimesDocument20 pagesJuly 6, 2018 Strathmore TimesStrathmore TimesNo ratings yet
- Jurnal Teledentistry 1Document7 pagesJurnal Teledentistry 1Dio Nella ArlinggaNo ratings yet
- Operative dentistry Lec.9 (Cavity liner and cement base) ىذش .دDocument9 pagesOperative dentistry Lec.9 (Cavity liner and cement base) ىذش .دvdtjqm8y4nNo ratings yet
- Organs of Speech & Airstream Mechanism: Ani SetyaningsihDocument13 pagesOrgans of Speech & Airstream Mechanism: Ani SetyaningsihAdelia RahmaNo ratings yet
- Community Dentistry Final Questions From Board Review Flashcards - QuizletDocument5 pagesCommunity Dentistry Final Questions From Board Review Flashcards - QuizletRMNo ratings yet
- Biomaterial: Selection of Materials Lect. 7Document19 pagesBiomaterial: Selection of Materials Lect. 7roseNo ratings yet
- Nutrition in Animals Notes PDFDocument7 pagesNutrition in Animals Notes PDFAryann GuptaNo ratings yet
- Amity Institute of Pharmacy: B. Pharm., Semester One Pharmacy Dr. Pawan Kumar PorwalDocument25 pagesAmity Institute of Pharmacy: B. Pharm., Semester One Pharmacy Dr. Pawan Kumar Porwalpawankumar guptaNo ratings yet
- Colgate Palmolive General OverviewDocument3 pagesColgate Palmolive General OverviewSrinivas NandikantiNo ratings yet
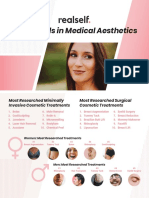
- RealSelf YearInReview OneSheetDocument2 pagesRealSelf YearInReview OneSheetDominico Adityo RaharjoNo ratings yet
- Operative Otolaryngology Head and Neck SurgeryDocument7 pagesOperative Otolaryngology Head and Neck SurgeryTugce InceNo ratings yet
- Introduction To PhoniticsDocument15 pagesIntroduction To PhoniticsLingua Academy-club LacNo ratings yet
- Case Report: Prosthodontic Management of Xerostomic Patient: A Technical ModificationDocument7 pagesCase Report: Prosthodontic Management of Xerostomic Patient: A Technical ModificationLisa Purnia CahyaniNo ratings yet
- Comparison of Tooth Shade Matching Using Visual and Digital Camera MethodsDocument5 pagesComparison of Tooth Shade Matching Using Visual and Digital Camera Methodsjanicesusanto2000No ratings yet
- Journal Homepage: - : IntroductionDocument9 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Bioactiverestorativedental Materials-Thenewfrontier: Mary Anne S. Melo,, Lamia Mokeem,, Jirun SunDocument16 pagesBioactiverestorativedental Materials-Thenewfrontier: Mary Anne S. Melo,, Lamia Mokeem,, Jirun SunDANTE DELEGUERYNo ratings yet